Department of Archaeology, Anthropology and Forensic Science
Abstract
The objective of this work is to compare handheld to laboratory-based Raman instruments for the identification of counterfeit medicines obtained from the world market. More than 200 tablets of proprietary and generic pharmaceutical products were obtained worldwide. Handheld Raman spectroscopy offered many advantages with respect to cost, rapidity, mobility, operation in wide temperature ranges, on-spot identification of materials and ease of use by non-skilled personnel. However, there were still many drawbacks associated with the use of handheld Raman instruments related to spectral quality, fluorescence and Raman activity. However, this did not affect the accuracy of identification.
Introduction
Pharmaceutical counterfeiting has been increasing continuously causing threat to public health worldwide. According to the latest World Health Organization (WHO) updated definition in 2012: “Spurious/ Falselylabelled/ Falsified/ Counterfeit (SFFC) are medicines that are deliberately and fraudulently mislabelled with respect to identity and/ or source” [1]. It can occur in any class of medicines and can range from those containing no active pharmaceutical ingredient (API) to those containing a toxic chemical [2]. For instance, counterfeit Xenical with no API was detected in the USA in 2007 [1]. Also, counterfeit Lipitor, Zyprexa and Metakelfin lacking sufficient API were detected in the UK and Tanzania between 2006 and 2009 [1]. In other cases, counterfeit glibenclamide containing six times the normal dose was detected in China in 2009 [1]. Lately, in February 2012, counterfeit Avastin was detected in the US distribution chain [3]. The situation became worse in May 2012, when counterfeit capsules made from powdered baby flesh and sold as “miracle cure” were seized in South Korea [4]. Consequently, the threat caused by counterfeit medicines ranges from ineffective treatment to potentially lethal effects. The Internet and street markets represent two major places for counterfeit medicines to enter the market [5, 6]. This highlights the need for rapid and non-destructive techniques that can detect counterfeit medicines across the whole supply chain. Raman spectroscopy has emerged lately as a major analytical tool for critical applications in the pharmaceutical sector [7, 8] particularly for counterfeit medicines. These applications included the identification of counterfeit artesunate tablets [9 -12], Cialis tablets [13, 14], Lipitor tablets [15] and Viagra tablets [11, 14].
Raman spectroscopy in those cases was able to detect that these tablets either contained the wrong API, no API and/ or low dose of the API. Thus, instead of their label claim, these tablets contained: Artesunic acid, calcite, calcium carbonate, dipyridone, erythromycin, lovastatin, paracetamol, starch, talc and titanium dioxide.
The significance of this technique is due to several major factors. First, it offers rapidity; thus, it only takes from a few seconds to a few minutes to obtain a Raman spectrum depending on the Raman activity of the sample measured. Second, it is a non-destructive technique as it requires minimal or no sample preparation. Third, it has high structural selectivity so it is selective for APIs as the Raman spectra of excipients are often masked by fluorescence [16 - 18]. In addition, it offers a mobile analytical tool as handheld Raman instruments can be carried anywhere. Consequently, it has the potential to prevent life threatening conditions associated with counterfeit medicines. The objective of this work is to compare handheld to laboratory-based Raman instruments for the identification of counterfeit medicines obtained from the world market.
Experimental
In this study, a total of 200 medicines containing a total of 42 different APIs were obtained from 11 countries in the world: France, Ghana, India, Lebanon, New Zealand, Switzerland, Syria, Tanzania, Turkey, UK and USA. The Raman spectra of these products were taken using a laboratorybased Raman instrument and two handheld Raman instruments. The Raman workstation was a dispersive Raman spectrometer equipped with a diode laser source (785 nm), 400 mW laser power, 6 mm spot size, a CCD detector and a holographic grating. The handheld instruments had a 785 nm laser excitation wavelength, an output of 250 - 300 mW, 0.2 - 2.5 mm spot size and a 2048 element silicon charge coupled device (CCD) detector. Both handheld instruments were equipped with a vial holder and universal tablet holder.
The Raman spectra of the tablets were measured in reflection mode.
For spectral comparison, three methods were applied: The probability method which was the handheld instruments’ in-built identification method, correlation in wavelength space (CWS) and principal component analysis (PCA).
For quantitative analysis, two powder models were tested to predict the concentration of the API in Ciproxin tablets [19]. The models were made either by diluting ciprofloxacin (the API) or Ciproxin powdered tablets with excipients. Model 1 (ciprofloxacin lactose dilution) was made by adding different aliquots of lactose to ciprofloxacin to give a range of 11 - 90% m/m ciprofoxacin. In addition, a 100% m/m sample (pure ciprofloxacin) was added to this model. Model 2 (Ciproxin lactose dilution) was made by adding different aliquots of lactose to Ciproxin powdered tablets to give a range of 33 - 67% m/m ciprofloxacin. Then partial least square regression (PLSR) was applied to the Raman spectra of these models obtained from the three instruments.
Results and Discussion
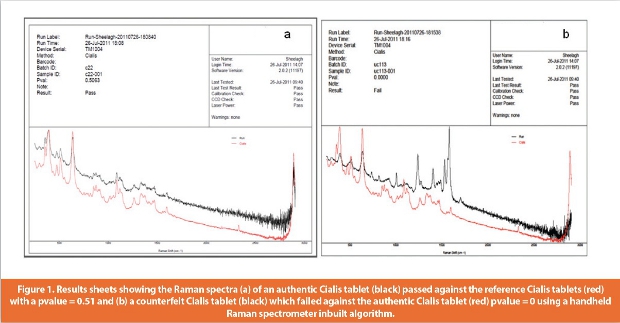
The handheld Raman instruments offered a simpler alternative approach compared to laboratory-based instruments. The simplicity of this approach was due to several factors. Handheld instruments offer mobility and usually have light weight (1 -2 kg) so they could be carried and used anywhere whether in pharmacies, hospitals and/or street markets. In addition, they can operate in different temperature conditions. Also, they offer a rapid and on the spot approach to the identification of medicines. Thus, a few seconds to minutes were enough to obtain a Raman spectrum depending on the Raman activity of the sample measured. Consequently, authentication of medicines could be established in minutes using the instrumental in-built algorithm. This could be carried out easily by non-skilled personnel. The algorithm worked using Bayes’ theorem by comparing the probability that the test sample spectrum (B) matched the library spectrum (A). In this respect, the test sample passes if the probability value (pvalue) of this sample spectrum against the library spectrum was above or equal to 0.05. Figure 1 shows the results sheet of authentic and counterfeit Cialis tablets which gave pvalue of 0.51 (passed) and 0 (failed) respectively when matched against an authentic Cialis tablet.
However, there were still some issues associated with the use of handheld instruments related to the accuracy of identification and quantification of APIs in medicines.
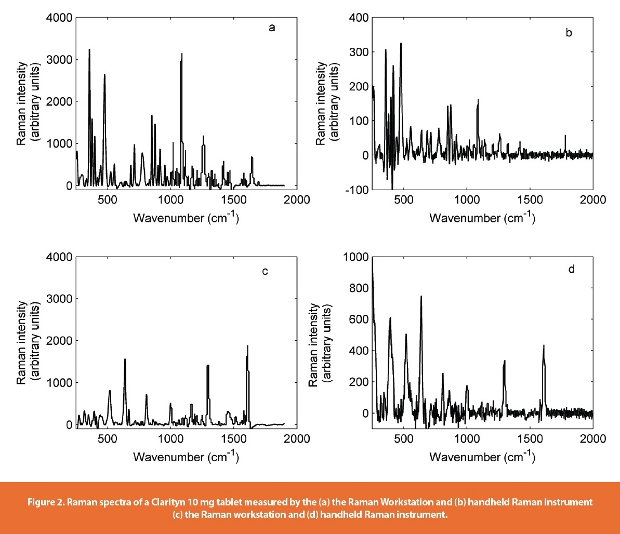
The laboratory-based instrument showed better spectral quality with regards to the larger number of peaks in the spectrum, low fluorescence and higher Raman scattering intensity. Though the Raman scattering intensity is arbitrary; yet this scattering intensity was up to 10 times higher in laboratory-based compared to handheld instruments. This was dependent on both the instrument and the samples. Thus, with the laboratory-based instrument the sample was exposed to higher laser power (600 mW) and larger spot size (6 mm). The medicines measured consisted of complex matrices of API and excipients in different concentrations. Whereas, APIs generally exhibit strong Raman activity, excipients’ Raman scattering is often masked by fluorescence [17]. Thus, samples with higher percentages of API had better spectral quality with both instruments. Figure 2 shows the Raman spectra of a Clarityn 10 mg tablet and a Diovan 80 mg tablet measured by both the laboratorybased and handheld instruments. The API in Clarityn 10 mg tablet, loratadine, was present in a low concentration of 10% m/m with three excipients: lactose monohydrate, maize starch and magnesium stearate. It showed 10 times more scattering intensity using the laboratory-based instrument than the handheld instrument and a signal to noise (S/N) ratio of 6.15 and 4.78 respectively. This was not the case with a Diovan 80 mg tablet which had only double the scattering intensity compared with the laboratory-based instrument. The Diovan tablet contained 50% m/m of API (valsartan) and 10 excipients: microcrystalline cellulose, crospovidone type A, colloidal anhydrous silica, magnesium stearate, hypromellose, titanium dioxide (E171), macrogol 8000, iron oxide red (E172), iron oxide yellow (E172) and iron oxide black (E172). Yet the S/N ratio was still higher for the laboratory-based instrument: 6.58 compared to 5.27 for the handheld instrument.
However, this did not affect the potential of identification of counterfeit medicines when offline analysis multivariate analysis methods were applied to the spectra obtained with the handheld instrument. Though the spectral noise contributed strongly to the correlation coefficient (r) value, CWS could still authenticate medicines provided they exhibited a high Raman scattering. In that case, an r value above 0.95 indicated that the test medicine passed against the reference medicine.
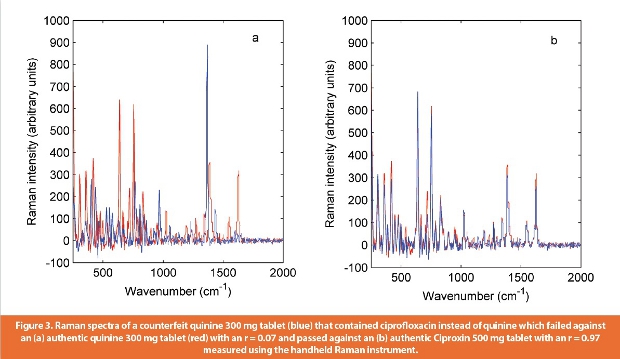
An example of the detection of counterfeit medicine using the handheld Raman instrument and the CWS method was a counterfeit quinine 300 mg tablet that contained ciprofloxacin API instead of quinine. The Raman spectrum of this tablet failed against an authentic quinine tablet spectrum (r = 0.07) and passed against a Ciproxin tablet spectrum (r = 0.97) (Figure 3). So the handheld Raman instrument was able to detect that the tablet was counterfeited by an antibiotic instead of anti-malarial. This was because both APIs were Raman active and present in high % m/m.
 However, fewer mismatches were obtained among pharmaceutical products with low % m/m of API and common excipients. In this case, A PCA method was shown to be more accurate as it classified spectra according to variances rather than comparing the whole spectrum and taking both peaks and noise into account. When PCA was applied to a known set of counterfeit Viagra tablets obtained worldwide, a clear classification was observed with the 95% equal frequency ellipses plotted around the authentic tablets (Figure 4).
However, fewer mismatches were obtained among pharmaceutical products with low % m/m of API and common excipients. In this case, A PCA method was shown to be more accurate as it classified spectra according to variances rather than comparing the whole spectrum and taking both peaks and noise into account. When PCA was applied to a known set of counterfeit Viagra tablets obtained worldwide, a clear classification was observed with the 95% equal frequency ellipses plotted around the authentic tablets (Figure 4).
For quantitative analysis, PLSR was applied to the Raman spectra of models 1 and 2 over the wavenumber range 250 - 1400 cm-1. The accuracy and precision of the models were evaluated using the regression correlation coefficient (r2) and relative standard error of calibration (RMSEC). Thus, higher r2 values and lower RMSEC values would show better models. For model 1, the handheld instrument showed more accurate results with r2 and RMSEC values of 0.986 and 3.75% m/m respectively (Table 1). 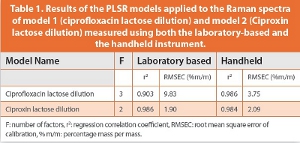 On the other hand, model 2 showed better agreement with the laboratory-based instrument; however, the results were still close to those obtained with the handheld instrument. Thus, the r2 values observed were 0.986 and 0.984 for the laboratory-based and handheld instruments respectively. The RMSEC values were also low in both cases and corresponded to 1.9% m/m and 2.09% m/m respectively. Consequently, the handheld instrument was more accurate than the laboratory-based instrument for quantitative analysis.
On the other hand, model 2 showed better agreement with the laboratory-based instrument; however, the results were still close to those obtained with the handheld instrument. Thus, the r2 values observed were 0.986 and 0.984 for the laboratory-based and handheld instruments respectively. The RMSEC values were also low in both cases and corresponded to 1.9% m/m and 2.09% m/m respectively. Consequently, the handheld instrument was more accurate than the laboratory-based instrument for quantitative analysis.
Conclusion
Handheld Raman instruments offered a more rapid, simpler and cost-effective alternative to laboratory-based instruments. The drawbacks associated with the use of these handheld instruments were related to spectral quality, fluorescence and Raman activity. However, these drawbacks did not affect the accuracy of identification and quantification of medicines.
References
1. WHO Factsheet N˚275, May 2012: http://www.who.int/mediacentre/factsheets/fs275/en/ accessed 23072012.
2. A. C. Moff at, S. Assi, and R. A. Watt, Identifying counterfeit medicines using near-infrared spectroscopy, JNIRS, 2010. 18: p. 1-15.
3. FDA, Counterfeit version of avastin in U.S. distribution, July 2012: http://www.fda.gov/ Drugs/DrugSafety/ucm291960.htm accessed 23072012.
4. MailOnline: http://www.dailymail.co.uk/news/article-2140702/South-Korea-customs-offi cialsthousands- pills-fi lled-powdered-human-baby-fl esh.html accesed 23072012.
5. S. Assi, R. A. Watt, and A.C. Moff at, Identifi cation of counterfeit medicines from The Internet and the world market using near-infrared spectroscopy. Anal. Methods, 2011. 3: p. 2231-2236.
6. D. Taylor, Trading in false hope, The School of Pharmacy, University of London, 2009.
7. D. E. Bugay and P. A. Martoglio Smith, Raman Spectroscopy in A. C. Moff at, M. D. Osselton and B. Widdop (Eds.), Clarke’s Analysis of Drugs and Poisons, 3rd edition, Pharmaceutical Press, London. 2004. p. 358-367.
8. Y. Ozaki and S. Sasic, Introduction to Raman Spectroscopy in S. Sasic (Ed.), Pharmaceutical Applications of Raman Spectroscopy, John Wiley and Sons Inc., Hoboken, New Jersey. 2008: p. 1-29.
9. C. Ricci, C. Eliasson, N.A. Macleod, P.N. Newton, P. Matousek, and S.G. Kazarian, Anal. and Bioanal. Chem., Characterisation of fake and genuine artesunate anti-malarial tablets using Fourier transform infrared imaging and spatially off set Raman spectroscopy through blister packs. 2007. 389: p. 1525-1532.
10. C. Ricci, L. Nyadong, F. Yang, F. M. Fernandez, C. D. Brown, P. N. Newton, and S. G. Kazarian, Assessment of handheld Raman instrumentation for in situ screening for potentially counterfeit artesunate antimalarial tablets by FT-Raman spectroscopy and direct ionization mass spectrometry, Anal. Chim. Acta, 2008. 623: p. 178-186.
11. M. de Veij, P. Vandenabeele, K.A. Hall, F.M. Fernandez, M.D. Green, N.J. White, A.M. Dondrop, P.N. Newton, and L. Moens, Fast detection and identification of counterfeit antimalarial tablets by Raman spectroscopy, J. Raman Spectrosc., 2007. 38: p. 181-187.
12. K.A. Hall, P.N. Newton, M.D. Green, M. de Veij, P. Vandenabeele, D. Pizzanelli, M. Mayxay, A. Dondorp, and F.M. Fernandez, Characterisation of counterfeit artesunate antimalarial tablets from Southeast Asia, Am. J. Trop. Med. Hyg., 2006. 75: p. 804-811.
13. S. Trefi , C. Routaboul, S. Hamieh, V. Gilard, M. Malet-Martino, and R. Martino, Analysis of illegally manufactured formulations of tadalafi l (Cialis) by 1H NMR, 2D DOSY 1H NMR and Raman spectroscopy, J. Pharm. Biomed. Anal., 2008. 12: p. 103-113.
14. P.Y. Sacre, E. Deconinck, T. De Beer, P. Courselle, R. Vancauwenberghe, P. Chiap, J. Crommen, and J.O. De Beer. Comparison and combination of spectroscopic techniques for the detection of counterfeit medicines, J. Pharm.
Biomed. Anal., 2010. 53: p. 445-453.
15. M.G. Orkoula and C.G. Kontoyannis, Non-destructive analysis of risperidone in fi lm-coated tablets, J. Pharm. Biomed. Anal., 2008. 47: p. 631-635.
16. S. Assi, R.A. Watt, and A.C. Moff at, Authentication of medicines using Raman spectroscopy, EPR, 2011. 1: p. 49-55.
17. S. Assi, R.A. Watt and A.C. Moff at, Comparison of laboratory and handheld instruments for the identifi cation of counterfeit medicines, Spectroscopy, 2011. June: p. 36-47.
18. P. Matousek, F. Thorley, P. Chen, M. Hargreaves, C. Tombling, P. Loeff en, M. Bloomfi eld, and D. Andrews, Emerging Raman techniques for rapid non-invasive characterization of pharmaceutical samples and containers, Spectroscopy, 2011. March: p.44-51.
19. Sulaf Assi, Robert A. Watt, and Anthony C. Moff at, On the quantifi cation of ciprofl oxacin in proprietary Ciproxin tablets and generic ciprofloxacin tablets using handheld Raman spectroscopy, J. Raman Spectrosc., 2011. doi: 10.1002/jrs.3125.
Author Biography
Dr. Sulaf Assi is a postdoctoral research fellow in Drug Misuse and Abuse at the University of Hertfordshire. She finished her Ph.D. on the identification of counterfeit medicines from the School of Pharmacy, University of London. Her active research is focused on the identification of novel psychoactive substances and counterfeit medicines using different analytical techniques and chemometrics.