Introduction
Practically, delivering a therapeutic agent via few breaths to the lungs is more convenient and less invasive than injections making it the ideal way for drug delivery in certain cases. Asthmatics may know best that a puff of their asthma reliever (e.g. salbutamol sulphate, a β2- agonist bronchodilator) is the fastest and most efficient way to get them to breathe normally within a few moments. Targeting the lungs for the treatment of respiratory illnesses like pneumonia, cystic fibrosis and tuberculosis may be the most effective way to deliver the right amount of the active pharmaceutical to the right organ while sparing the whole body the unnecessary exposure to unwanted side effects. Furthermore, the therapeutic dose may be lower when compared to oral or parenteral doses, which is extremely advantageous in cases like antibiotics, in order to minimize drug resistance. On the other hand, when formulated for the lower respiratory tract, systemic absorption is promoted, and the potential for delivery of systemic agents becomes possible [1]. With advances in biotechnology and genomics, an explosion in the potent and specific therapeutics is demanding new delivery technologies as well as devices. The pulmonary route may be the most attractive way to deliver these fragile macromolecular drugs offering a large surface area and a rich capillary network for drug bioavailability. Avoiding the first pass hepatic metabolism and the relatively lower enzymatic activity are advantageous when compared to the oral route [2].
Controlled Release Inhalation Therapy
Promises
Current advancements in inhalation delivery technologies as well as device design seem parallel to the growing need for treatment of increasing respiratory diseases. Despite the increasing number of inhalation products for the treatment of respiratory illnesses, most prominent examples may include bronchodilators and steroids, no controlled release inhalation system exists to-date. The short duration of action and the need to deliver drugs at least 3-4 times daily is a significant drawback of current inhalation therapies [3]. Tailoring the drug release rate to the needs of specific disease conditions can be achieved by a controlled release formulation. For example, a controlled release formulation of active pharmaceuticals like antibacterials, cytotoxic agents or immunosuppressants can keep the medicament concentration relatively constant within the lung tissue for prolonged periods of time and, consequently, boost the effect of those drugs. While keeping a constant blood concentration for systemically acting molecules like insulin is another example of why a controlled release formulation may be beneficial in effectively controlling the blood sugar level. Furthermore, protecting the active therapeutic from the environment in the respiratory tract (e.g. mucociliary clearance and macrophage phagocytosis) is another huge virtue for a successful controlled delivery system. Maybe most importantly from the patient’s prospective would be simplifying the complexity of the treatment regimen and improving his/her compliance which is ultimately reflected by better disease management and health outcomes [4].
Concerns
Unfortunately, it is not a simple process to design, engineer, formulate and produce a precise controlled release formulation for pulmonary inhalation. The critical size range for respiratory particles in general, which needs to be 2.5 - 6 microns for local drug delivery and less than 2.5 microns for potential systemic delivery (Figure 1), makes the residence of these particles in the lungs subject to different factors [5]. Small particles production is usually associated with an increase of surface area-to-mass ratio, which makes the physicochemical properties of these particles including their ability to be efficiently aerosolized in the desired area in the lungs rather complicated. This is in addition to the natural defensive mechanisms of the respiratory system, which actively act on the removal of particles by the mucociliary escalator, or phagocytosis by the alveolar macrophages depending on where the particles have landed. This, in turn, depends on the size, shape and surface characteristics of the particles [5, 6]. Furthermore, upon inhalation, drug particles will deposit onto an epithelial surface which average cell diameter is equivalent to that of the particle (<10 μm) and on a fluid layer that has an equivalent thickness (~0.1-10 μm) [7]. Furthermore, the lung epithelia structure varies from one region to another where the surface barrier liquid thickness and composition vary accordingly [8]. 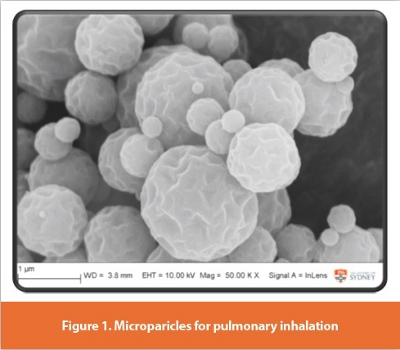 While the relationship between the physico-chemical properties of particles within the respiratory size range and their aerosolization efficiency is still not fully understood, the fate of deposited particles is yet to be accurately predicted and requires detailed investigation prior to use in humans. The effective delivery of drugs both locally or systemically via the lungs is dependent upon the solubilization and release of the active pharmaceutical and subsequent diffusion and/or active transport across the epithelia. Mucin and phospholipids are the main components on the surface and, depending upon the regional deposition and disease state of the patient, the drug particle may encounter a thicker mucus layer or a sub-micron phospholipid fi lm [7].The increased blood flow of the lungs and its permeability, which are also relevant to the disease state, can be huge advantages for products intended for systemic absorption as the actives get absorbed faster. Obviously, on the other hand, they can be drawbacks for medications intended to act locally in the respiratory tract (e.g. antibiotics and corticosteroids) where undesired systemic exposure is inevitable. In the case of a formulation intended for controlling the release of the active material it carries, rich blood flow, high permeability as well as clearance mechanisms pose significant hurdles for such formulations to act the way they are designed to act.
While the relationship between the physico-chemical properties of particles within the respiratory size range and their aerosolization efficiency is still not fully understood, the fate of deposited particles is yet to be accurately predicted and requires detailed investigation prior to use in humans. The effective delivery of drugs both locally or systemically via the lungs is dependent upon the solubilization and release of the active pharmaceutical and subsequent diffusion and/or active transport across the epithelia. Mucin and phospholipids are the main components on the surface and, depending upon the regional deposition and disease state of the patient, the drug particle may encounter a thicker mucus layer or a sub-micron phospholipid fi lm [7].The increased blood flow of the lungs and its permeability, which are also relevant to the disease state, can be huge advantages for products intended for systemic absorption as the actives get absorbed faster. Obviously, on the other hand, they can be drawbacks for medications intended to act locally in the respiratory tract (e.g. antibiotics and corticosteroids) where undesired systemic exposure is inevitable. In the case of a formulation intended for controlling the release of the active material it carries, rich blood flow, high permeability as well as clearance mechanisms pose significant hurdles for such formulations to act the way they are designed to act.
Production
Many conventional approaches have been explored to form controlled release inhalation medications including: natural/synthetic polymer encapsulation, liposomal based particles, solid lipid microparticles, and viscous semisolids vehicles. An up-to-date review on the recent advances in this field was published in 2009 by Salama et al. [4]. For example, when insulin was encapsulated in liposomes, its absorption from the lungs was enhanced and prolonged [9]. In addition, by using calcium phosphate–PEG particles, the bioavailability and duration of action of insulin were enhanced when administered to the lungs of rats compared to conventional subcutaneous delivery [10]. Similarly, iota- and kappa-carrageenan have been shown to be potential release-modifying polysaccharide gels. A modified absorption rate of theophylline and flutecasone propionate was observed when the polymers were utilized in solutions <5% w/v, with no evident damaging or inflammatory effect on lung tissue [11].
It is also of utmost importance to consider the safety of using release-modifying agents. The local toxicity to the lung tissue could be due to the adverse local effect of the drug, metabolite, carrier or excipient on the cells. Generally, liposomes are more tolerable [12] since they are made of phospholipids similar to the lungs own surfactants’ phospholipids. Liposomes have also the advantage of the ability to controlling the release rate by manipulating their size, number of bilayers and charge. But unfortunately, their high production cost and relative instability makes them disadvantageous [13]. Polymeric biocompatible materials are able to produce less expensive and more stable nano/ micro inhalation particles. Yet their potential pulmonary toxicity like inflammation or hemorage, polymer accumulation effects [14, 15] and the common use of organic solvents for their production [16-18] may also question their safety as approved excipients. Nevertheless, some of those systems may be more tolerable than others. A study of the most popular release modifying polymers (including hydroxypropyl cellulose, gelatin, chitosan, alginate, hyaluronic acid, and poly(lactide-coglycolide, PLGA) on a Calu-3 lung epithelial model suggested relatively good tolerance; although PLGA, showed a decrease in cell membrane integrity and increased inflammatory mediator concentrations [19]. Glyceryl behenate [20] and polyvinyl alcohol [21] have been used to incorporate drug molecules, preliminary studies showed no indication of in vivo or in vitro A549 cell toxicity, respectively. Although these particulate systems are biodegradable in nature, future studies should also consider long-term toxicity effects and clearance mechanisms.
Evaluation
The release and subsequent availability of the active materials in the lung from the controlled release formulation will be influenced by drug solubility, lipophilicity, chemical structure and size. Furthermore, the site where the particles/droplets settle also determines the fate of the encapsulated active pharmaceutical. Active and passive mechanisms are known to exist in the lung and because of the diverse nature of molecules used to treat respiratory diseases and the associated excipients, it seems a very complicated process that has not been fully investigated to date [22].
An increasing number of literatures have dealt with controlled release formulations intended for pulmonary inhalation mainly from the production and in vitro characterization points of view. For example, extended release profiles, ranging from hours to days, have been demonstrated using different in vitro release approaches [17, 23-26]. However, a very important issue that we need to have in mind while evaluating this type of emerging research is that there is no standard method to evaluate these proposed controlled release formulations. It is also worth mentioning that very few of these studies had in vivo data to support claims of controlled release [18, 27, 28]. These in vitro techniques vary between the conventional USP Apparatus 1 [29], 2 and 4 [30], paddle over disc methods [31], modified twin stage impinger [26] and diffusion cells [30, 32].
In an attempt to narrow this gap, Salama et al. [30] have compared different in vitro methods in use to evaluate the release profiles of controlled release dry powders for inhalation and the capability of the techniques used for in vitro characterization to differentiate between a series of model controlled release formulations. In vivo release profiles of two of these formulations were subsequently evaluated using an ovine model (Figure 2) [33]. The findings have clearly shown that there is a significant difference between the tested formulations using a diffusion model while there was no significant difference when using the modifications of conventional apparatus under the same conditions, which may not be an appropriate approach for the assessment of drug dissolution. It was clearly envisaged that small differences in the in vitro drug release were translated to have significant implications when tested in vivo.
 Without a standardized method of assessing and testing controlled release formulations for inhalation, it becomes quite difficult to accurately compare methods of production of potential controlled release formulations and their effectiveness. Therefore, it is difficult to assess whether the in vitro approaches described the formulations accurately or under/over-estimated in vivo release characteristics. This may end up to the conclusion that development/modification of conventional in vitro models may prove irrelevant in testing these formulations. It is also of specific importance to consider the biology at the epithelial interface. This includes the presence of influx and efflux transporters as well as active clearance mechanisms (cilia motion and macrophage phagocytosis) which may be dominating factors to consider when delivering novel inhalation medicines [34].
Without a standardized method of assessing and testing controlled release formulations for inhalation, it becomes quite difficult to accurately compare methods of production of potential controlled release formulations and their effectiveness. Therefore, it is difficult to assess whether the in vitro approaches described the formulations accurately or under/over-estimated in vivo release characteristics. This may end up to the conclusion that development/modification of conventional in vitro models may prove irrelevant in testing these formulations. It is also of specific importance to consider the biology at the epithelial interface. This includes the presence of influx and efflux transporters as well as active clearance mechanisms (cilia motion and macrophage phagocytosis) which may be dominating factors to consider when delivering novel inhalation medicines [34].
An in vitro/in vivo correlation would be particularly important to carry out standardized in vitro release testing during controlled release formulation and screening stages. Furthermore, cell lines and/or animal studies are needed to accurately investigate the exact pattern by which these particles are deposited in the lungs, the mechanism by which the drug is released from the particles, cellular uptake and absorption, as well as the clearance from the lung. Alveolar macrophages phagocytosis of this type of modified release formulations is of particular interest and needs to be further explored. Other potential polymeric materials especially with muco-adhesive properties need to be investigated in the search for formulating critical therapeutics with reduced cilia clearance rates.
Conclusion
In conclusion, the controlled release formulations have complex challenges, which add to the requirements of formulating a conventional inhalation therapy. Not only should the particles be small enough to be inhalable, but also a release-modifying excipient is needed to control the release of the drug after delivery. Both of these steps are challenging: the production of micron-sized particles is difficult, since with a reduction in size there is a significant increase in surface areato- mass ratio; subsequently, it becomes more difficult to produce a controlled release profile and incorporate effective release agents. The use of a release agent also has its own concerns; rate of release, degradation, clearance and safety issues. However, it is important that we understand the dissolution behavior of existing formulations before we can hope to understand what happens with controlled release formulations. In addition, further animal studies with larger population are needed to establish an in vitro/in vivo correlation. Ultimately, the area of controlled release formulation and the study of the mechanism of deposition and clearance are far from understood and although many challenges exist, controlled release formulations to the lung have not yet reached their full potential and are still underappreciated.
References
1. Jain, K.K., Drug Delivery systems - An Overview, in Drug Delivery Systems, K.K. Jain, Editor 2008, Humana Press: Totowa. NJ. p. 1-50.
2. Smyth, H.D.C. and A.J. Hickey, Controlled Pulmonary Drug Delivery 2011: Controlled Release Society.
3. Byron, P.R., Prediction of drug residence times in regions of the human respiratory tract following aerosol inhalation. Journal of Pharmaceutical Sciences, 1986. 75(5): p. 433-438.
4. Salama, R., et al., Recent Advances in Controlled Release pulmonary Therapy. Current Drug Delivery, 2009. 6: p. 404-414.
5. Pritchard, J.N., The influence of lung deposition on clinical response. Journal of Aerosol Medicine- Deposition Clearance and Effects in the Lung, 2001. 14: p. S19-S26.
6. Martonen, T.B., Mathematical model for the selective deposition of inhaled pharmaceuticals. Journal of Pharmaceutical Sciences, 1993. 82(12): p. 1191-1199.
7. Patton, J.S., et al., The particle has landed - characterizing the fate of inhaled pharmaceuticals. Journal of Aerosol Medicine and Pulmonary Delivery, 2010. 23 ((Supp 1)): p. S71-S87.
8. Patton, J.S. and B.R. Byron, Inhaling medicines: Delivering drugs to the body through the lungs. Natures Reviews Drug Discovery, 2007. 6: p. 67-74.
9. Zeng, X.M., G.P. Martin, and C. Marriott, The Controlled Delivery of Drugs to the Lung. International Journal of Pharmaceutics, 1995. 124(2): p. 149-164.
10. Garcia-Contreras, L., et al., Evaluation of Novel Particles as Pulmonary Delivery Systems for Insulin in Rats. AAPS PharmSci 2003. 5 (2): p. Article 9.
11. Yamada, K., et al., Carrageenans can regulate the pulmonary absorption of antiasthmatic drugs and their retention in the rat lung tissues without any membrane damage. International Journal of Pharmaceutics, 2005. 293(1-2): p. 63-72.
12. Myers, M.A., et al., Pulmonary effects of chronic exposure to liposome aerosols in mice. Experimental Lung Reserach, 1993. 19: p. 1-19.
13. Karathanasis, E., et al., Preparation of in vivo cleavable agglomerated liposomes suitable for modulated pulmonary drug delivery. Journal of Controlled Release, 2005. 103(1): p. 159-175.
14. Armstrong, D.J., et al., Poly-(D,L-lactic acid) microspheres incorporating histological dyes for intra-pulmonary histopathological investigations. The Journal of Pharmacy and Pharmacology, 1996 48(3): p. 258-262.
15. Müller, R.H., et al., Cytotoxicity of magnetite-loaded polylactide, polylactide/glycolide particles and solid lipid nanoparticles. International Journal of Pharmaceutics, 1996. 138(1): p. 85-94.
16. Alhusban, F.A. and P.C. Seville, Carbomer-modified spray-dried respirable powders for pulmonary delivery of salbutamol sulphate. Journal of Microencapsulation, 2009. 26(5): p. 444-455.
17. Learoyd, T.P., et al., Sustained delivery of salbutamol and beclometasone from spray-dried double emulsions. Journal of Microencapsulation, 2010. 27(2): p. 162-170.
18. Rytting, E., et al., In vitro and in vivo performance of biocompatible negatively-charged salbutamol-loaded nanoparticles. Journal of Controlled Release, 2010. 141: p. 101-107.
19. Sivadas, N., et al., A comparative study of a range of polymeric microspheres as potential carriers for the inhalation of proteins. International Journal of Pharmaceutics, 2008. 358(1- 2): p. 159-167.
20. Sanna, V., et al., Preparation and In Vivo Toxicity Study of Solid Lipid Microparticles as Carrier for Pulmonary Administration. AAPS PharmSciTech 2004. 5(2): p. Article 27.
21. Salama, R.O., et al., Preparation and evaluation of controlled release microparticles for respiratory protein therapy. Journal of Pharmaceutical Sciences, 2009. (In Press, Accepted 3 November 2008): p. DOI:10.1002/jps.21653
22. Young, P.M., D. Traini, and R. Salama, In Vitro Techniques Equipped to Study Clinically Relevant Controlled Release Products. Respiratory Drug Delivery Europe, 2011.
23. Asada, M., et al., Theophylline particle design using chitosan by the spray drying. International Journal of Pharmaceutics, 2004. 270(1-2): p. 167-174.
24. Huang, Y.-C., et al., The characteristics of betamethasone-loaded chitosan microparticles by spray-drying method. Journal of Microencapsulation, 2003. 20(4): p. 459-472.
25. Learoyd, T.P., et al., Chitosan-based spray-dried respirable powders for sustained delivery of terbutaline sulfate. European Journal of Pharmaceutics and Biopharmaceutics, 2008. 68(2): p. 224-234.
26. McConville, J.T., et al., Use of a novel modified TSI for the evaluation of controlled-release aerosol formulations. I. Drug Development and Industrial Pharmacy, 2000. 26(11): p. 1191-1198.
27. Ungaro, F., et al., Insulin-loaded PLGA/cyclodextrin large porous particles with improved aerosolization properties: In vivo deposition and hypoglycaemic activity after delivery to rat lungs. Journal of Controlled Release, 2009. 135(1): p. 25-34.
28. Yamamoto, A., et al., Control of pulmonary absorption of water-soluble compounds by various viscous vehicles. International Journal of Pharmaceutics, 2004. 282(1-2): p. 141-149.
29. Learoyd, T.P., et al., Modified release of beclometasone dipropionate from chitosan-based spraydried respirable powders. Powder Technology, 2008. 187(3): p. 231-238.
30. Salama, R.O., et al., Preparation and characterisation of controlled release co-spray dried drugpolymer microparticles for inhalation 2: Evaluation of in vitro release profiling methodologies for controlled release respiratory aerosols. European Journal of Pharmaceutics and Biopharmaceutics, 2008. 70(1): p. 145-152.
31. Copley, M., Y.-J. Son, and J. McConville, Dissolution testing for inhaled drugs. Pharmaceutical Technology Europe, 2010. 22(11): p. http://pharmtech.findpharma.com/pharmtech/ Drug+Delivery/Dissolution-Testing-For-Inhaled-drugs/ArticleStandard/article/detail/692804 visited on 01/03/2011.
32. Cook, R.O., R.K. Pannu, and I.W. Kellaway, Novel sustained release microspheres for pulmonary drug delivery Journal of Controlled Release, 2005. 104(1): p. 79-90.
33. Salama, R., et al., Development of an In Vivo Ovine Dry Powder Inhalation Model for the Evaluation of Conventional and Controlled Release Microparticles. AAPS Journal, 2009. 11(3): p. 465-468.
34. Haghi, M., et al., Modification of Disodium Cromoglycate Passage Across Lung Epithelium In Vitro Via Incorporation into Polymeric Microparticles. The AAPS Journal, 2012. 14(1): p. 79-86.
Author Biography
Dr. Rania Salama’s research expertise is in inhalation medicine, with a specific interest in controlled release formulations, chronic respiratory illnesses management and regimens simplification, in vitro/in vivo methodologies and correlations. Specifically, Rania’s recent research has focused on studying formulation and in vitro characterization of controlled release dry powder inhalers using synthetic and natural polymeric materials and their in vivo testing in a recently developed large animal model. In addition, she has experience in development and implementation of comparative bioavailability and bioequivalence studies (in human volunteers). Currently, she is a Postdoctoral Research Associate with the Advanced Drug Delivery Group at the Faculty of Pharmacy, University of Sydney, NSW, Australia. She has extensive expertise in undergraduate and postgraduate education as well as supervising postgraduate research students.