This article provides a summary of key aspects concerning the future of Transdermal Drug Delivery Systems (TDDS) with respect to key market drivers for giving a drug transdermally, history of passive diffusion-controlled systems, and experiences and progress made with new physical enhancement techniques. Focus is given to technologies that have either led to marketed products or have reached the clinical development stage. Benefits and limitations of old and new techniques are discussed considering biological constraints and physicochemical requirements on formulations and active ingredients.
Rationale for Transdermal Drug Delivery (TDD)
Rationale for giving a drug transdermally has to be driven by an unmet medical need that can be met by this route, thus adding value to a drug therapy. For example, stable plasma level time profiles over extended time periods may reduce not only the dosing frequency, but possibly also side effects of the medication and daily doses that have to be administered by other routes.
As transdermal drug administration is an easy, painless, and convenient mode of application, patient compliance for this route is in general high, especially in elderly and young people and patients groups who have difficulties swallowing or who are suffering from nausea or emesis.
In addition, transdermal patches may improve competitiveness of a pharmaceutical company in a large market segment. Known examples are nitroglycerin patches in the cardiovascular field, which were successfully introduced in the nitrate market more than 30 years ago, and recent introduction of rivastigmine patches in the indication Alzheimer and dopamine agonist patches in the indications Parkinson’s disease (PD) and Restless Legs Syndrome (RLS) [1].
There is a drug-driven rationale in those cases where the active ingredient meets the requirements for transdermal candidates (see below) and where issues connected with the oral application can be solved by this route.
Finally, transdermal systems can support lifecycle management of approved drugs by strengthening the patent/IP situation and relationship to key customers, i.e., patients, physicians, health authorities, and caregivers, and offering a brand augmentation.
General Aspects to be Considered for TDD
Before the drug is absorbed by the vascular network and/or lymphatic system in the dermis, it has to overcome several hurdles [2,3]:
- The stratum corneum (SC), the main diffusion barrier of the skin
- Antigen presenting cells of viable epidermis reporting to the immune system like Langerhans cells and also cells filtering UV radiation or forming a barrier against chemicals
- Immune and inflammatory cells of the dermis which react on any mechanically or chemically induced irritation, like the mast cells. If the outermost skin layer has to be interrupted by microneedles or laser beams, location of nerve endings in the dermis has to be considered as well
In passive diffusion controlled systems the drug molecule can take different routes to cross the SC. The para- or intercellular tortuous route between the corneocytes is seen as the principal transport pathway for most lipohilic drugs. Following this route the drug has to diffuse through bilayers of ceramides, which are associated with free fatty acids (and their esters) and cholesterol. Structural properties of the paracellular lipid matrix fit the barrier needs of skin by being simultaneously robust and impermeable [4].
Human skin has on average about 100 to 200 sweat pores/cm2. Hair follicle density is in the same order of magnitude depending on age and region of the skin. Depending on physicochemical properties of the drug and formulation drug, uptake by this pathway may also not be negligible despite the small skin area fraction of about 0.1%.
The transcellular pathway requires repeated drug partition and diffusion across structured bilayers, and seems to be usually less important.
Requirements for Transdermal Drug Candidates
A transdermal drug candidate for passive diffusion controlled systems has to be potent, i.e., the daily dose must be in the lower mg range and must be well tolerated by the skin.
From a physicochemical point of view, a number of requirements have to be met:
- High lipophilicity (ideal log PO/W ≈ 2)
- Low molecular weight (ideally below 500 Dalton)
- Low melting point (ideally below 150 °C)
- Sufficient solubility in water at pH 6 to 7.4 (e.g., ≈ 0.05 to 1mg/ml if target delivery rate is in the mg range per day)
- Suitable pKa (determines solubility of the un-ionized form at physiological pH)
- Appropriate solubility parameter (measure of cohesion energy of the unionized form) (ideally about 18-22MPa0.5)
Requirements for Transdermal Formulations
All ingredients of the device have to be well tolerated by the skin and support continuous drug penetration through the skin at a reproducible rate over the intended application time period.
Accordingly, formulation ingredients must not close drug specific pathways. For example, it has been shown that shunt diffusion plays a major role in caffeine absorption, provided that pores are not closed by ingredients like waxes before drug application [5].
From a physicochemical point of view, the formulation of passive systems has to promote drug partitioning into and transport across the skin layers, to maintain drug activity gradient across the skin nearly constant over the intended application time and to assure a high drug depletion rate of the patch. Formulation factors influencing drug absorption rate are:
- Chemical potential of the drug
- Co-delivery of penetration enhancers
- Use of drug carrier systems (like micro- or nano-emulsions, liposomes, transferosomes, etc.)
- Drug particle size
- Eutectic mixtures
- Use of ion pairs
For transdermal patches an optimum balance between adhesion and cold flow properties of the adhesive formulation has to be adjusted to prevent detachment of the drug release surface from the skin surface during application or cohesion failure of the adhesive which might lead, for example, to drug containing adhesive residues on skin or clothes. Accordingly, state-of-the-art optimization of adhesion properties is an essential part of TDDS formulation development and an integral part of general regulatory requirements on quality, as summarized below [6].
Key Quality and Safety Relevant Objectives for TDD
- Deliver the required dose
- Minimize variability of drug absorption
- Minimize local skin reactions
- Maintain adequate physical stability and physical integrity of the TDDS during storage and application
- Minimize the excess amount of drug remaining in the TDDS after application
- Assure good adhesion and cohesion properties
- Minimize risk of detachment during application
- Minimize variability of skin adhesion and cold flow
Advantages and Constraints of Passive Diffusion Controlled Transdermal Systems
Basic assessment criteria for transdermal drug administration have to consider a number of benefits, and drawbacks, as listed below.
Key Advantages:
- Non-invasive administration
- High patient compliance
- Reduced daily dose
- Reduction of unwanted side effects
- Continuous drug delivery
- Stable plasma concentrations
- Visibility of drug administration
Key Constraints/Limitations:
- Skin tolerability
- Skin barrier properties
- Variability of application site conditions
Physical Enhancement Techniques Tested in Clinical Studies for TDD
Approaches to increase transepidermal drug transport rate may be subdivided in laser-, electrical-, structure-, and velocity-based techniques [7].
An example for enhancing drug delivery rate across human skin via application of an electric current is offered by iontophoresis. In these systems drug delivery rate across the skin barrier is mainly governed by electro-repulsion of ionized drug molecules from an electrode of similar charge. Accordingly, transepidermal transport rate is proportional to the applied constant current enabling enhancement of transdermal dose and control of drug delivery kinetics.
Another advanced electrical approach is microporation of the biological barrier via an alternating current applied to an array of microelectrodes or filaments which are brought in contact with the skin [8]. This treatment creates local heat leading to cell ablation and transient creation of microchannels or pores typically 50 to 100μm in diameter. Target penetration depth of local heating is less than 100μm and pore number is typically in the range of 100 to 200cm².
Microporation of the skin can be also achieved via application of short, solid microneedles or hollow cannulae, which penetrate the SC and epidermis up to the upper dermis, ideally without reaching pain-sensitive nerve endings in the dermis [9,10]. This structure-based technique causes a minimally invasive and painless disruption of the skin barrier. Different types of microneedles and modes of action are outlined in Figure 1.
 Figure 1. Types of Microneedles and Modes of Actions.
Figure 1. Types of Microneedles and Modes of Actions.Solid microneedles can be used to pierce the skin before the drug containing formulation is placed on the pretreated skin area (“poke and patch” approach), or the microneedles are coated with the drug before insertion and the drug remains in the skin on removal of the microneedle patch (“coat and poke“ approach).
If the microneedles consist of dissolvable sugars or biodegradable polymers which are loaded with drug, they remain in the skin together with the drug and only their carrier system is removed from the skin (“poke and release approach”).
Finally, drug solutions may be injected into the dermis via hollow microneedles (“poke and flow approach”).
Solid microneedles can be made of metal, silicon, or polymers; other materials like glass or ceramics have been proposed as well. Penetration depths of microneedles cover a wider range compared to electrically based microporation. However, the number and size of pores created by the described methods is similar or comparable in order of magnitude. Compared to a subcutaneous injection penetration depth of hollow microneedles is by a factor of 10 to 100 shorter.
Micropores of similar size can be also generated by using laser techniques, which do not require application of mechanical force to the skin and thus circumvent the effect of skin elasticity, which may lead to significant resistance against microneedle insertion [9]. Constraints to be considered with lasers are heat dissipation to surrounding skin tissue, which has to be minimized by very short laser pulses, and control of penetration depth, which has to be adjusted by the energy delivered by the laser beam per unit micropore area.
Advantages and Constraints of Enhancement Techniques
Described enhancement techniques offer a painless alternative to conventional injections similar to passive systems. In addition, they expand the range of transdermal drug candidates to salts and larger molecules like peptides, antibodies, proteins, and nucleotides. Furthermore, they enable bolus dosing and on demand delivery. Last but not least they can offer advantages in the field of vaccination by increasing the immune response via id application [11].
Again, skin tolerability is the most important prerequisite also for enhancement techniques. Skin disrupture may increase risk of immune and inflammatory reactions; recovery of disrupted skin regions , i.e., shelf life of micropores has to be carefully tested as well as any infection risk. Furthermore, application of microneedle patches must overcome the constraints caused by skin elasticity. The pressure which is needed to insert microneedles has to be controlled to minimize occurrence of unwanted skin reactions, e.g., by mast cell damage.
Finally, maturity of technologies in routine production must be demonstrated and costs of manufacturing have to be justified by therapeutic benefits.
Figures 2a and 2b give an overview of transdermal patches that were approved by FDA over the last decades. Not included are approvals of several patch-less systems and gels intended for treatment of sex hormone deficiencies and incontinence.
 Figure 2a. Approval History of TddS (US), 1979-2003.
Figure 2a. Approval History of TddS (US), 1979-2003. Figure 2b. Approval History of TddS (US), 2004-2013.
Figure 2b. Approval History of TddS (US), 2004-2013.The main indication fields for transdermal drug delivery systems introduced in the market between 1979 and 2003 were chronic pain, cardiovascular diseases, hormone replacement therapy, and local dermal analgesia.
While from 1979 to 2003 an iontophoretic patch with lidocaine/epinephrine was the only approved system that used a physical enhancement techniques [4]. Further “active” systems were approved by FDA in the following 10 years: Sonophoresis for lidocaine, iontophoresis for fentanyl in acute postoperative pain, or most recently iontophoresis for sumatriptane to treat migraine patients [12]. In addition, a heat-assisted system was approved that provided an enhanced passive diffusion of lidocaine by generating heat at the application site by a controlled chemical reaction following application.
Main indication fields for TDDS approved since 2004 were chronic pain, central nervous system (CNS) diseases, cancer, and dementia.
With passive systems a drug release of about 1mg/cm² is achievable meaning, i.e., with usual patch sizes of 10 to 40cm² daily dose up to 10 to 40mg may be applied across the skin.
Physical enhancement techniques are designed to deliver the drug through smaller skin areas. Nevertheless, they may allow a delivery of higher drug quantities even for large molecules. A rough estimate of dose limitations ranges between 20 and 100mg per treated total area, depending on the technology and the patch design.
Figure 3 gives an overview of selected projects based on microporation techniques which have reached the clinical development stage [9].
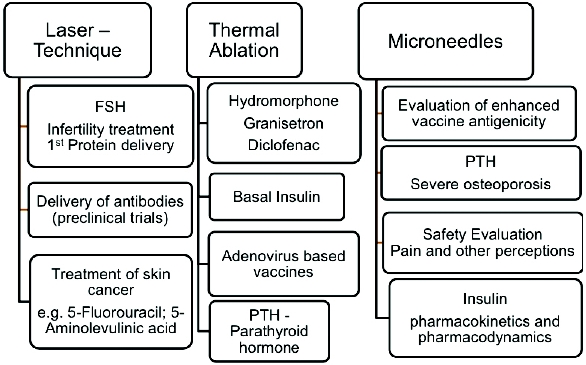 Figure 3. Clinical development Stage of Skin Microporation Techniques [9,10].
Figure 3. Clinical development Stage of Skin Microporation Techniques [9,10].In the microneedle area a certain emphasis is currently given to the delivery of vaccines, as intradermal application of a vaccine might improve immune response rates, especially in elderly patients. For example, a seasonal flu vaccine for id microinjection has been shown to be equivalent to a traditional IM vaccine plus adjuvant and has already been approved by FDA and EMA.
For decades another high priority project has been the painless delivery of insulin with a feedback control provided by varying glucose levels. Microneedle technologies intended for id delivery of insulin may be combined in the future with blood glucose sampling targeting for a feedback control of drug delivery.
Delivery of parathyroid hormone (PTH) in the treatment of severe osteoporosis via microneedles is in an advanced development stage. In placebo-controlled clinical studies, microneedle delivery has shown promising results at increasing total hip and lumbar spine bone mineral density [13]. Compared to a standard preparation that requires cool storage and has a shelf-life of only 28 days, solid PTH-coated microneedles do not require refrigeration and are stable at normal storage conditions for 2 years.
Considering today’s experiences and progress in the transdermal field, it can be concluded that the future of transdermal drug delivery depends on:
- Development of passive and active transdermal drug delivery systems which meet unmet medical, patient, and drug needs
- Further improvement of skin pretreatment methods
- Development of on demand systems which combine a suitable technique with a tailor-made drug reservoir or formulation
- Progress made with appropriate techniques and approaches to overcome constraints of passive diffusion without compromising skin integrity.
References
- B. Boroojerdi; H.M. Wolff ; M. Braun; and D.K.A. Scheller. Rotigotine transdermal patch for the treatment of Parkinson’s disease and restless leg syndrome. Drugs of Today 2010; 46: 483-505.
- The relationship between structure and barrier function of skin. In Roberts, M.S. and Walters, K.A. (Eds.). Dermal Absorption and Toxicity Assessment, Marcel Dekker, New York (1998), pp. 1-42.
- Morrow, D.I.J.; McCarron, P.A.; Woolfson, A.D.; and Donnelly, E.F. Innovative strategies for enhancing topical and transdermal drug delivery. The Open Drug Delivery Journal 2007; 1: 36-59.
- Iwai, I.; Han, H.M.; Hollander, L.; Svensson, S.; Öfverstedt, L.G.; Anwar, J.; Brewer, J.; Bloksgaard, M.; Laloeu, A.; Nosek, D.; Masich, S.; Bagatolli, L.A.; Skoglund, U.; and Norle, L. The human skin barrier is organized as stacked bilayers of fully extended ceramides with cholesterol molecules associated with the Ceramide Spinghoid moiety. J. Invest. Dermatology 2012; 132: 2215-2225.
- Otberg, N.; Patzelt, A.; Rasulev, U.; Hagemeister, T.; Linscheid, M.; Sinkgraven, R.; Sterry, W.; and Lademann, J. The role of hair follicles in the percutaneous absorption of caffeine. Br. J. Clin. Phamacol. 2007; 65: 488-492.
- Van Buskirk, G.A.; Arsulowicz, D.; Basu, P.; Block, L.; Cai, B.; Cleary, G.W.; Ghosh, T.; González, M.A.; Kanios. D.; Marques, M.; Noonan, P.J.K.; Ocheltree, T.; Schwarz, P.; Shah, V.; Spencer, T.S.; Tavares, L.; Ulman, K.; Uppoor, R.; and Yeoh, T. Passive Transdermal Systems Whitepaper Incorporating Current Chemistry, Manufacturing and Controls (CMC) Development Principles. AAPS PharmSciTech, published online Jan 2012.
- Khan, A.; Yasir, M.; Asif, M.; Chauhan, I.; Singh, A.P.; Sharma, R.; Singh, P.; and Rai, S. Iontophoretic drug delivery: history and applications. J. Appl. Pharm. Sci. 2011; 1: 11-24.
- Sintov, A.C.; Krymberk, I.; Daniel, D.; Hannan, T.; Sohn, Z.; and Levin, G. Radiofrequency driven skin microchanneling as a new way for electrically assisted transdermal delivery of hydrophilic drugs. J. Control. Release 2003; 89: 311-320.
- Gratieri, T.; Albert, I.; and Kalia, Y.N. Next generation intra-and transdermal therapeutic systems: using non-and minimally-invasive technologies to increase drug delivery into and across the skin. Eur. J. Pharm. Sci. 2013; 50: 609-22.
- Stevenson, C.L.; Santini, J.T.; and Langer, R. Reservoir-based drug delivery systems utilizing microtechnology. Advanced Drug Delivery Reviews 2012; 64: 1590–1602.
- Sullivan, S.P.; Koutsonanos, D.G.; Martin, M.D.P.; Lee, J.W.; Zarnitsyn, V.; Choi, S.-O.; Murthy, N.; Compans, R.W.; Skountzou, I.; and Prausnitz, M.R. Dissolving polymer microneedle patches for influenza vaccination. Nature Medicine 2010; 16: 914-920.
- Smith, T.R.; Goldstein, J.; Singer, R.; Pugach, N.; Silberstein, S.; Pierce, MW. Twelve month tolerability and efficacy study of NP101, the sumatriptan iontophoretic transdermal system. Headache 2012; 52: 612-624.
- Daddona, P.E.; Matriano, J.A.; Mandema, J.; Maa, and Y.-F. Parathyroid hormone (1-34)-coated microneedle patch system: clinical pharmacokinetics and pharmacodynamicsfor treatment of osteoporosis. Pharm. Res. 2011; 28: 159–165.
Author Biography
H. Michael Wolff , Ph.D., studied pharmacy and chemistry at the Philipps University in Marburg, Germany and gained his doctorate in Pharmaceutical Chemistry. In 1979, he joined Schwarz Pharma where he held different management positions and was responsible for the Pharmaceutical Development of Transdermal Systems. Dr. Wolff is currently director at UCB BIOSCIENCES in Monheim, Germany and Visiting Professor at the University of Sunderland.