Introduction
Drug abuse, which is defined as the repeated or sporadic non-medical use of a drug for the positive psychoactive effects it produces, is widespread in the United States. According to the 2011 Vital Signs report from the Centers for Disease Control, the legal sale of opioid painkillers has increased by 300% over a decade. This has been accompanied by an increase in the milligram-per-person use of prescription opioids, an increase in opioid overdose deaths (~14,000 death/year), and the rise of concern for their misuse, diversion and abuse.1 Besides marijuana, opioid medications have exceeded other drugs of abuse (e.g. cocaine and heroin) in prevalence of use.
Mitigating the risk for accidental overdose and abuse of opioids requires a multi-disciplinary approach involving physicians, pharmacists, and regulators.2,3 Any effort that does not incorporate all involved stakeholders will be unlikely to achieve its full potential of public health benefits. One effort undertaken by the medical community was the submission of a Citizens Petition requesting changes to opioid analgesic labels to the Food and Drug Administration (FDA) by the Physicians for Responsible Opioid Prescribing (PROP).4 This petition proposed the following: addition of a maximum daily dose of 100 mg morphine-equivalent for non-cancer pain, a three-month limit of continuous treatment duration for non-cancer pain, and removal of the term “moderate” in the indication. However, the American Academy of Pain Medicine and Professionals for Rational Opioid Monitoring and Pharmacotherapy have opposed the PROP petition, arguing that it lacks the scientific evidence to support the removal of moderate pain from indications and that it is based on arbitrary interpretation of dosing and duration limits.5,6 A systematic review of guideline recommendations related to mitigating the risk for accidental overdose and misuse, which was published in 2013, identified agreements among various guidelines on several opioid mitigation strategies.7 These strategies include caution with higher doses, caution when titrating doses, and dose reduction when switching between opioids. Despite apparent consensus on some recommendations, there is little evidence that any of these approaches decreases the risk for accidental overdose and misuse/abuse of opioids.
Regulatory agencies and the pharmaceutical industry have also attempted to address this risk. In response to a request from the FDA, a pharmaceutical industry working group was formed to prepare the extended release/long acting (ER/LA) opioids risk evaluation and mitigation strategy (REMS) proposal as class-wide, single shared REMS for FDA approval. There are many legislative initiatives, such as the REMS for ER/LA opioids, opioid labeling updates with boxed warnings, and prescription drug monitoring programs to educate, certify, and track prescribing habits of physicians. The ultimate goal is to ensure safe use of these drugs by striking the right balance between the pain management needs of patients and mitigation of the risks posed by opioids and other analgesics. As part of the response to the prescription drug abuse crisis, Congress instructed the FDA to promulgate guidance on the development of abuse deterrent products under the FDA Safety and Innovation Act.3,8,9 Hence, the FDA strongly encourages sponsors to follow their guidance to develop abuse-deterrent formulations (ADFs) for opioid drug products as an additional risk mitigation approach to curb a troubling rise in opioid painkiller abuse. The development and regulatory considerations of abuse-deterrent formulations (i.e. introduction of limits or impediments to abuse in a drug formulation) is the main focus of this article.
Though there is a growing interest in ADFs, they are not a new concept. There are a variety of ADF approaches that are either currently inuse or in development (Table 1). These technologies are categorized according to the Guidance for Industry: Abuse-Deterrent Opioids- Evaluation and Labeling and Assessment of Abuse Potential of Drugs (8, 9). A number of FDA-approved products utilize these approaches (Table 2).
Table 1. Abuse Deterrent Technologies Used in Pharmaceutical Products or Under Development
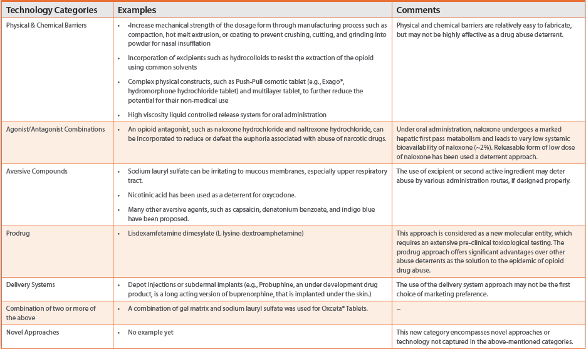
Table 2. Example of FDA-Approved Abuse-Deterrent Drug Products

One of the earliest approaches was the agonist/antagonist combination. Talwin NX®, a reformulated Talwin® (pentazocine) with naloxone (an opioid antagonist), received approval in 1982. Under oral administration of Talwin NX®, naloxone undergoes a marked hepatic first-pass metabolism leading to very low systemic bioavailability (~2%). When Talwin NX is manipulated for abuse via injection or insufflation, naloxone will block the euphoric feeling for abusers. In the two years following the introduction of Talwin NX®, the rates of both emergency room and medical examiner mentions per million prescriptions decreased by 70%, indicating that the incorporation of naloxone into the pentazocine formulation successfully reduced abuse.10 Higher doses of naloxone (i.e. 5, 10, and 20 mg) have also been formulated with oxycodone as a non-releasable abuse deterrent, while allowing the opioid to alleviate pain when administered appropriately (i.e., Targiniq ER®). Naltrexone, another opioid antagonist, has also been utilized for ADFs. Following oral administration, naltrexone undergoes complete absorption (approximately 96% of the dose absorbed combining naltrexone, active metabolite 6- β-naltrexol and other metabolites) from the gastrointestinal tract. Using naltrexone as an abuse deterrent requires it to be embedded as a non-releasable component, such as in Embeta®, so that there is no absorption when administered orally. However, the potential for abuse with this approach remains, particularly via oral administration.
Both releasable and non-releasable formulations offer different benefits. The use of a releasable antagonist (e.g. Talwin NX®) creates a much higher hurdle for abusers to separate the drug from the abuse deterrent agent(s) because they are homogenously mixed together. Use of a non-releasable antagonist (e.g., Embeta) can prevent the risk of side effects from systemic exposure to the antagonist as long as the integrity of the dosage form is maintained. A third, intriguing possibility for ADFs is the direct delivery of an antagonist to the large intestine, achieved through an enteric coating, to locally block opioid action and reduce associated constipation.11
The abuse deterrent formulations for oral administration may consist of either single-unit dosage form (e.g. tablets and capsules) or multiple-unit dosage form (e.g. beads or pellets in capsules or in sachets). In general, it is difficult to fabricate a single-unit dosage form because it is technically challenging to sequester and coat the powder-sized abuse deterrent(s), while avoiding damage during the compacting process. For multiple-unit dosage forms, technologies such as extrusion spheronization, drug layer processing, and fluid bed coating are versatile techniques of fabricating constructs with abuse deterrent properties. Furthermore, advanced capsule filling machines are capable of filling up to four different beads into a capsule shell. Other than multiple-layered single bead approaches, the use of multiple types of beads for abuse deterrent formulations is also feasible, provided that there is no discernible difference in bead appearance in terms of size, shape, or color.
Use of aversive compounds is another approach. Inclusion of these ingredients is designed to cause uncomfortable effects if the drug is either manipulated prior to ingestion or taken at a higher dose than recommended. There are many aversive compounds available for use. Sodium lauryl sulfate is a known irritant of mucous membranes, especially in the upper respiratory tract, and has been used in Oxeta to prevent intranasal abuse of crushed tablets. Additionally, anionic surface-active agents, such as sodium lauryl sulfate and sodium dioctyl sulfosuccinate, are used to interact with positively-charged amine drugs to form poorly water-soluble complexes, which can result in decreased absorption. For example, Wells et al. investigated the effect of anionic surfactants on the release of chlorpheniramine maleate from an inert, heterogeneous matrix and found that the formation of a poorly water-soluble complex between chlorpheniramine maleate and the anionic surfactant greatly slowed release at low concentrations of surfactant.12 Furthermore, Rao et al. observed that as the concentration of sodium lauryl sulfate increased to 15% w/w, the release rate correspondingly decreased, which was attributed to the formation of a poorly soluble complex.13 Furthermore, Matschiner et al. characterized ion pair formation between erythromycin and sodium lauryl sulfate, and they confirmed the assumption of a complex formation of poorly water-soluble estolate salt in a 1:1 molar ratio.14 Because of the solubilization effect of surface active agents, the concentration of these surfactants in the ADF is important to optimize the formation of poorly watersoluble complexes while avoiding solubilization of the ion-pair in the micellar phase. Another surface-active agent, sodium dioctyl sulfosuccinate, is commonly used as a stool softener and may provide the added benefit of alleviation of constipation, in addition to its use as an abuse deterrent. Similarly, an ion-exchange resin, such as sodium polystyrene sulfonate to complex with and inactivate opioids may be another possible ADF approach.
The use of nicotinic acid as a deterrent (i.e. Acurox® Tablets) has been previously used in oxycodone formulations. Nicotinic acid causes a flushing effect when taken in larger quantities than recommended. There are many concerns, however, regarding the use of nicotinic acid as a deterrent. One concern is that the flushing effects may not be noxious enough to limit oral abuse of the drug. Since nicotinic acid in the treatment of hypercholesterolemia is still of major importance, the number of users of nicotinic acid with un-tolerable flushing side effects may be not significantly high. The variable tolerance of nicotinic acid in patients without a clear threshold dosage calls into question nicotinic acid’s effectiveness as a deterrent. Physicians commonly recommend fatty foods and non-steroidal anti-inflammatory drugs to greatly blunt flushing when taking nicotinic acid for reducing hypercholesterolemia; this is a potential avenue of avoiding abuse deterrent strategy.15
The incorporation of many other aversive agents into opioid drug products have been proposed. These include:
- A bittering agent to impart an intensely bitter taste, such as sugar octaacetate, denatonium benzoate, or denatonium saccharide
- An agonist of pain receptors as a strong irritant, such as capsaicin
- An emetic to trigger vomiting, such as ipecac or zinc sulfate
- A diuretic to induce urgency and frequency of micturition, such as hydrochlorothiazide
- A bright colorant tracer as a psychological deterrent to resist adulteration or identify abusers, such as indigo blue
- A malodorous compound as a deterrent for nasal insufflation, such as skatole or indole 3-carbinol
Aversive compounds as abuse deterrents may be designed with either a releasable or non-releasable approach in mind. These proposed deterrents may not be highly toxic, but they have issues for this proposed use. Every deterrent agent has a different pharmacological or irritating effect, and each may have unwanted chemical interactions with the opioids. For that reason, there is a constant debate about the use of deterrents in terms of which deterrent to select, the amount to use, and mechanism of delivery. The problem of unintentional harm from aversive compounds may be more common than many researchers suspect, as there may be complicated use situations and actual use in healthcare may not mirror the approved usage. Limited numbers of drug products with abuse deterrent formulations are currently approved, and there has not been enough data to assess their risks and benefits. Years may pass before research indicates whether these formulations reduce the abuse and misuse potential of opioids and whether they cause harmful side effects.
Physical and chemical barriers can be utilized to produce sustained release formulations, which may reduce opioid abuse by simply slowing down the release rate. With this approach, however, comes the concern that the higher quantities of opioids in sustained release dosages may attract drug abusers. Sustained release properties provide a barrier to drug extraction for abuse. One example of physical barrier lies in hydrophilic matrix tablets. When immersed in water or hydroalcoholic solvents, the hydrophilic matrix forms a viscous gel layer. Subsequently, drug diffusion through and erosion of the gel layer imparts sustained release properties to the matrix tablets. There are various gel forming agents and viscosity modifiers, including: sodium alginate, hydroxyethyl cellulose, hydroxypropyl cellulose, methyl cellulose, hydroxyl methyl cellulose, polyacrylic acids, polyethylene oxide, karaya gum, acacia, tragacanth gum, locust bean gum, and guar gum. Also, hot melt technology has been applied to ADFs by using polyethylene oxide (a low melting point polymer) to increase the crushing strength.16 Other complex physical constructs, such as push-pull osmotic pump tablets, also have been claimed to possess a better physical barrier and resistance to drug abuse, compared to simple hydrophilic matrix tablet. It is not clear, however, to what extent the dosage form’s resistance to crushing and chewing contributes to deterrence of abuse. High viscosity gels based on sucrose acetate and cellulose acetate butyrate have also been proposed for use in opioid abuse deterrence. These high viscosity liquid-controlled release systems require the use of soft gel capsules.17-20
The use of a prodrug formulation is another common approach to deterring abuse. Lisdexamfetamine dimesylate (Vyvase®) is an example of a prodrug approach to delivering amphetamine, while minimizing abuse potential compared to the parent compound. This sustained release effect is due to the gradual hydrolysis of lysine-conjugated amphetamine (prodrug) in blood to its parent drug, even with rapid gastrointestinal absorption of the prodrug. Similarly, the prodrug approach has been applied to opioids.21,22 If the prodrug is designed to be activated by a gastrointestinal enzyme, the abuse potential for non-oral administration routes (e.g., nasal, inhalation, and injection) is significantly attenuated because the prodrug is not activated during absorption through these routes. Because of its sustained release properties via chemical modifications and the requirement for activation of the prodrug, the prodrug approach effectively resists chewing and crushing tactics of drug abuse. If the specific enzyme required for activation of a prodrug is saturable, euphoric effects experienced by the patients may be limited by the enzyme kinetics involved in the activation of the prodrug. In this aspect, the chemical modification approach may provide abuse deterrent features for various abuse routes, such as snorting, inhalation, injection, and even ingestion. These features (i.e. abuse-deterrent and drug release properties) are inherent to the designed prodrug. Hence, the formulation strategy of a prodrug may be relatively simple when compared to other ADF approaches.
It should also be noted that combinations of different approaches may be used to further reduce abuse potential. For example, the agonist/antagonist approach may be combined with the use of an aversive compound. The addition of an aversive compound could be titrated such that the proper dosage unit only results in a tolerable effect when administered. If used in greater dosage than recommended, the total ingested aversive compound accumulates and triggers the undesired effects. This combination has the potential to discourage abuse of drugs by taking excess doses, as well as the potential to decrease abuse through non-oral routes of administration.
Testing and Regulatory Considerations for Abuse Deterrent Formulations
As outlined in 21 CFR 300.50 (a), two or more drugs may be combined in a single dosage form when each component makes a contribution to the claimed effect. An abuse deterrent formulation can be regarded as a special case of this rule because a deterrent component is incorporated to minimize the potential for abuse of the principal component (e.g. opioids). Abuse deterrent formulations may be applied to a variety of opioid drug products. In addition to many immediate-release opioids, the extended release/long acting (ER/LA) opioid analgesics include: Avinza®, Butrans®, Dolophine®, Duragesic®, Embeda®, Exalgo®, Kadian®, MS Contin®, Nucynta ER®, Opana ER®, Oxycontin ER®, Palladone®, Zohydro ER® and generic versions of any of these brands. There are six approved products (Oxecta®, Embeta®, Oxycontin®, Opana ER®, Vyvanse®, and Targiniq ER®) which contain abuse deterrent properties described in their package inserts. These approved ADFs are far from perfect. Each may mitigate abuse to some extent for one or more administration routes, but none are designed to mitigate drug abuse derived from taking multiple unaltered pills orally. This abuse tactic is a major concern, as the abuse of opioids frequently begins in this way, often escalating over time to more involved measures, including: crushing the dosage form, altering the administration route, or extracting the active ingredient to satisfy the abuser’s progressive addiction needs. Thus, methods of deterring ingestion of larger than recommended doses are critical to avoid escalation of drug abuse. Significant work has gone into developing abuse deterrent strategies against drug ingestion by alternate administration routes and opioid extraction from formulations. It is understandable that the former approach is much more difficult to accomplish than the latter and researchers attempted to tackle the easier one first. One product (Acurox® [oxycodone hydrochloride and niacin] tablets) has attempted to mitigate the three most common abuse methods:15 oral (when taken at doses higher than recommended), intranasal (nasally snorting crushed tablets) and intravenous (IV injection of dissolved tablets). Despite the fact that this product did not receive approval, this case, along with other successful cases (see Table 2), build a foundation for other ADF development companies to improve upon.
The FDA has released final guidance documents for ADF development, which should be the basis for the design and conduct of studies of ADFs. The FDA recommended collecting data from each of the following studies categories to obtain a full understanding of the ADF’s abuse potential:
- Laboratory-based in vitro manipulation and extraction studies (Category 1),
- Pharmacokinetic studies (Category 2),
- Clinical abuse potential studies (Category 3).
These studies categories are recommended to be conducted sequentially and the data obtained from category 1 may affect the designs and need of the other two categories and the results of category 2 may affect the design and need for category 3 studies. For physical and chemical barrier approaches, the following properties must be evaluated for an ADF and a comparator: crushability, extractability, dissolution, syringeability, and vaporization. Sponsors must demonstrate that the manipulation of the ADF is more difficult compared to the manipulation of a comparator through in vitro manipulation, extraction and dissolution studies. Currently, there are no standardized tests to evaluate ADFs, and analysis methods comparing the ADF and comparator may be selected at the sponsor’s discretion. However, tests should be as extensive and objective as possible, and the sponsor should standardize test methods to generate reliable physicochemical testing results when possible.
For crushability, sponsors must evaluate the mechanical strength of the ADF against common crushing devices, such as pill cutters with grinding capability, pepper grinders, coffee grinders, and high speed choppers. For extractability, sponsors should assess the intact and crushed ADF’s resistance to solvent extraction by readily available solvents, such as isopropyl alcohol and ethyl alcohol. . The resistance to dissolution change also must be demonstrated for the intact and crushed ADF, measured with dissolution methods specified by the FDA. In addition, hydroalcoholic media (e.g. 10%, 20% and 40% ethanol) should be used to evaluate the resistance of dissolution change for the ADF. Pharmacokinetic testing of controlled release ADF vs. the comparator to determine if ADF’s controlled release property is resistant to mechanical crushing is also required. For syringeability, evaluation of drawing and injecting the reconstituted reduced particle matters from the ADF through different needle gauges is performed to show the difficulty to draw up and inject the liquid, compared to the comparator. Sponsors also need to demonstrate the ineffectiveness of the ADF to be smoked (e.g. drug decomposes before its melting).
In addition to efficacy/safety studies, additional clinical studies may be required (e.g. pharmacokinetic studies, deterrent dose response studies, and abuse liability studies) to demonstrate several important parameters. These parameters include the efficacy of the principal component, the safety of the deterrent formulation, and the efficacy of the deterrent component in minimizing abuse of the principal component.
The major challenge in ADF design is the selection of an appropriate strategy and amount of deterrent to discourage excessive oral consumption of opioid drugs in an unaltered form. It is critical that ADFs have 1) an effective, well-tolerated combination of an opioid and deterrent within recommended guidelines and 2) statistically significant and clinically meaningful results in drug dislike/like scores at doses designed to be aversive (e.g. four times the recommended dose in Acurox® case), when compared to opioid alone. Special attention must be given to the amount of effort required to bypass the abuse deterrence mechanism in ADFs. Marketing an ADF with an easily-compromised abuse deterrent mechanism is costly and counterproductive. Drug like/dislike scores are subjective measures evaluated from patients, based on drug rating questionnaires containing visual analog scales or bipolar visual analog scales. Additional subjective drug ratings may be useful measures in evaluating ADFs, and options include: the Addiction Research Center Inventory’s morphinebenzedrine group scale (euphoria), LSD specific scale (dysphoria), and pentobarbital-chlorpromazine-alcohol group scale (sedation).23,24 If the dislike effect is transient and not noxious enough, the ADF will be easily tolerated by patients and ineffective for its role. On the other hand, if the dislike effect is long-lasting and highly unpleasant, the ADF will likely be effective, but also result in a negative effect on the safety profile compared to non-abuse deterrent formulations. It is difficult to balance the risk of causing adverse effects in opioid-using patients and the risk of opioid misuse and abuse. Simply put, the cost of potentially punishing the many legitimate opioid users because of the minority of abusers is questionable, which needs to be answered and justified by better and safer opioids while reducing the risk for abuse and misuse.
Conclusion
Prescription drug abuse and misuse is a particularly complex issue. While healthcare system abuse interventions are clearly important, these may be inadequate in addressing all of the intricacies of this problem. Due to their powerful abuse deterrent capabilities, ADFs should be considered an integral tool in preventing opioid misuse, abuse, and overdoses. More development efforts are necessary to identify robust abuse-deterrent properties, refine abuse-deterrent formulations to increase their efficacy in opioid products, and create new paradigms for addressing this critical problem.
References
- Center for Disease Control and Prevention, CDC vital signs: Prescription Painkiller overdoses in the U.S., www.cdc.gov/Vitalsigns/PainkillerOverdoses/. Updated November 1, 2011.
- Woodcock, J, “A Difficult Balance- Pain Management, Drug Safety, and the FDA”, N. Engl. J. Med., 2009, 361(22), 2105-7.
- Food and Drug Administration Safety and Innovation Act, Pub. L. No. 112-144, 126 Stat. 993, § 1122© (2012).
- http://www.citizen.org/documents/2048.pdf
- http://www.painedu.org/spotlight.asp?spotlight Number=159
- http://www.bpihealth.com/news/the-great-opioid-debate.aspx
- Nuckols, T, et al., Ann. Intern. Med., 2013 Nov. 12 [doi:10.7326/0003-4819-160-1-201401070-00732].
- Guidance for Industry, Abuse-Deterrent Opioids – Evaluation and Labeling, January 2013 (Draft Guidance) and 2015 (Final Guidance).
- Guidance for Industry, Assessment of Abuse Potential of Drugs, January 2012.
- Baum, C, Hsu, JP, Nelson RC, “The Impact of the Addition of Naloxone on the Use and Abuse of Pentazocine”, Public Health Report, 1987, 102(4), 426-429.
- Meissner, W, Schmidt U, Hartmann M, Kath R, Reinhart K, “Oral Naloxone Reverses Opioid- Associated Constipation”, Pain, 2000, 84(1), 105-109.
- Wells, M, Parrott, E, “Effect of Anionic Surfactants on the Release on Chlorpheniramine Maleate from an Inert, Heterogeneous Matrix”, Drug Dev. Ind. Pharm., 1992, 18(2), 175-186.
- Rao, “Effect of sodium lauryl sulfate on the release of rifampicin from guar gum matrix”, Indian Journal of Pharmaceutical Sciences, 200, September-October, 62(5), 404-406.
- Matschiner, S, Neubert, R, Wohlrab, W, “Optimization of Topical Erythromycin Formulations by Ion-Pairing”, Skin Pharmacology, 1995, 8(6), 319-326.
- Advisory Committee Briefing Package for NDA 22451 Acurox® (oxycodone hydrochloride and niacin) tablets, www.fda.gov/downloads/adviso...rugsAdvisoryCommittee/ UCM209143.pdf.
- Arkenau-Maric, E., Bartholomaus, J., Kugelmann, H., “Dosage form that is safeguarded from abuse”, European Patent 1658054B1 and U.S. Patent Application 20070183980A1.
- Yum, S.I., Schoenhard, G., Tipton, A.J., Gilson, J.W., Middleton, J.C., “Oral Drug Delivery System”, U.S. Patent 8,420,120; 8.133.507; 8,153,152;8,354,124; 8,168,217; 8,147,870.
- Tipton, A.J., Holl, R.J., “High Viscosity Liquid Controlled Delivery System”, U.S. Patent 5,747,058 (1998).
- Tipton, A.J., “High Viscosityy Liquid Controlled Delivery System as a Device”, U.S. Patent 5,968,542 (1999).
- Gibson, J.W., Sullivan, S.A., Middleton, J.C., Tipton, A.J., “High Viscosity Liquid Controlled Delivery System and Medical or Surgical Device”, U.S. Patent 6,413,536 (2002).
- Jenkins, T.F., Husfeld, C.O., “Compositions Comprising Enzyme-Clevable Oxycodone Prodrug”, U.S. Patent 8,568,228 and 8,497,237 (2013).
- Shafer, J.A., Telyatnikov, V.V. and Guo, Z., “Compounds and Methods for Lowering the Abuse Potential and Extending the Duration of Action of a Drug”, U.S. Patent 7,230,005 (2007).
- Hill, H.E., Haertzen, C.A., Wolbach, A.B. and Miner, E.J., “The Addiction Research Center Inventory: Standardization of Scales which Evaluate Subjective Effects of Morphine, Amphetamine, Pentobarbital, Alcohol, LSD-25, Pyrahexyl and Chlorpromazine”, Psychopharmacologia, 1963, 4, 167-183.
- Haertzen, C.A., Hill, H.E., and Belleville, R.E., “Development of the Addiction Research Center Inventory (ARCI): Selection of items that are sensitive to the effects of various drugs”, Psychopharmacologia, 1963, 4, 155-166.
The opinions expressed in this review by the authors do not necessarily reflect the view or policies of the Food and Drug Administration (FDA).