Introduction
The oral route of administration is central for the delivery of a large number of important drugs in various therapeutic areas, and many patients prefer standard oral dosage forms as well as advanced oral drug delivery systems over other dosage forms. This preference stems from various factors including the non-invasiveness, ease-of-use, and reliability of oral dosage forms. The importance of oral drug delivery also manifests itself in that it comprises – at 38% in 2012 [1] – the largest fraction of all of drug delivery and the oral drug delivery market is growing at a compounded annual growth rate of 10.3% from 2010 to 2017 [2].
Scientists have been pushing the boundaries of oral drug delivery for many decades, and in addition to all the early advances in this area, progress in several domains of oral drug delivery has come to fruition over the past 15 years. Many medicines built on this progress are already enabling improved outcomes for patients today. This article will highlight several milestones relative to oral drug delivery reached over the past 15 years in the domains of:
- absorption process understanding
- developability of new chemical entities (NCEs)
- formulation/drug delivery system design, and
- patient-centered drug design.
Future opportunities will also be discussed.
Absorption Process Understanding
One principal goal of oral drug administration is to ensure high and reliable bioavailability of the drug. Upon ingestion and disintegration of the dosage form in the GI tract, there are several factors determining the absolute bioavailability of a drug, including its resistance to presystemic intestinal degradation (enzymatic and non-enzymatic) and to hepatic first pass metabolism, as well as its solubility in GI fluids and its permeability (via passive and active transport) of biologic membranes.
Signifi cant progress has been made over the past two decades to model, predict, and test all of the aforementioned factors. In particular, the introduction and the later widespread use of the Caco-2 cell line for permeability testing as well as the increased sophistication in dissolution testing, has helped improve the precision of predicting the absorption of drugs [3].
Another important milestone has been the introduction of the Biopharmaceutics Classification System (BCS) in 1995 [4] and its widespread use among scientists – including formulation/ drug delivery scientists, pharmacokineticists, pharmacologists, and medicinal chemists, among others – in the process of drug development, thereafter. Today, the BCS concept is also applied to predict the impact of the physiological state of the GI tract and food intake on the bioavailability of drugs [5]. In addition to the BCS, other sophisticated in vitro as well as in silico tools have become available to scientists in the recent past, helping evaluate the suitability of drug candidates, formulations, and delivery systems for oral administration. Building on as well as going beyond pharmacopeial dissolution testing, these modern tools include software packages for the simulation of absorption processes and complex experimental dissolution set-ups like the artificial stomach. Combined uses of dissolution testing in an artificial stomach setup and computing the data in silico have also been applied more recently [6]. Novel approaches include various important factors, e.g. the prediction of supersaturation and precipitation in the GItract, which can be of high relevance. Furthermore, the development of an integrated tool for the prediction of the in vivo performance of oral dosage forms, the “OrBiTo” (Oral Biopharmaceuticals Tool) focused at addressing current gaps in scientists’ toolbox, has been proposed very recently [7].
Today’s increased understanding of absorption processes is the basis for modern development of oral medicines, whether it is applied at early stages of R&D at the pipeline level (portfolio of developmental drugs), the single molecule level (e.g. for the enablement of an specifi c drug), or at the formulation level (e.g. for line-extensions).
Developability of NCEs
Drug discovery today, designing novel drugs for tomorrow, is an important and exciting fi eld. Once a pharmacological target has been identifi ed, early activities comprise the screening of numerous compounds – e.g. from a compound library – in order to determine which ones interact with the target. This process typically results in the identifi cation of so-called hits as one of the fi rst steps in the modern drug discovery process. Subsequent structural optimization of these hits via the hit to lead to candidate to drug sequence takes into account various strategies to increase effi cacy, selectivity, metabolic stability, and, importantly, oral bioavailability of the compounds. Typically it takes about 8-12 years from the initial testing stage via preclinical and clinical development until the new medicine will be available to the patient, and in the process the number of approximately 8,000 compounds will be narrowed down to one marketed drug.
 Figure 1. Drug discovery and developability information (modifi ed from [8])
Figure 1. Drug discovery and developability information (modifi ed from [8])How to select leads and candidates – and thereby ultimately the novel drug – has been heavily infl uenced by insights from the domain of developability of NCEs [8] in the recent past.
The task at hand – in addition to optimizing the compound’s pharmacological activity – is to increase the probability of successfully moving that very compound from in vitro testing to the bedside. This task can be achieved by carefully designing the physico-chemical and biopharmaceutical properties of the NCE, thereby enhancing its developability. In recent years, a number of models and multi-parametric principles have been established to support exactly that activity. An earlier milestone in that domain has been the publication of Lipinski’s rule-of-fi ve (RO5) in 1997 [9] and its direct or modifi ed application thereafter. Its increasing importance in the late 90s and its rapid uptake is proven by the fact that in the year 2004 alone, the citations in CAS SciFinder to the original RO5 publication exceeded 1,000 [10]. The original RO5 defi nes four physico-chemical parameters found in a set of orally active drugs which made it into phase II clinical trials:
- molecular weight ≤500
- logP ≤5
- H-bond donors ≤5
- H-bond acceptors ≤10, and
Over the past 15 years, the knowledge relative to predictors for oral activity of drug candidates has significantly grown, and various changes to the RO5 have been suggested, including the introduction of a rule-of-three for the application in fragmentbased drug design [11].
Today, it is widely accepted that a sequential approach of focusing on effi cacy and selectivity, e.g. designing a high affi nity ligand, in a fi rst step and to deal with its drug-like properties only later on, is an inferior strategy to a more holistic approach which includes taking properties like solubility and permeability into account already early on. Furthermore, enzymatic as well as chemical stability are of interest as one looks at the overall developability of compounds.
In practical terms, there are various opportunities at the molecular level to infl uence the developability parameter of solubility, including the reduction of crystallinity of the compound or the introduction of hydrophilic/ionizable groups. A good example of the latter is the protease inhibitor Crixivan® (indinavir) [12]. Here the introduction of an ionizable moiety (a substituted piperazin) signifi cantly increased the aqueous solubility and thereby contributed to an increase from low bioavailability for some analogs to substantial human bioavailability for the drug itself. Despite all the progress made related to the prediction of solubility, oral bioavailability, and overall developability of drug candidates over the last 15 years, an undeniable and signifi cant trend towards a higher fraction of poorly soluble (BCS class II and IV) compounds became evident in the innovator pipeline of developmental drugs recently [13]. It has been discussed that three main factors contributed to that trend [7]:
- addition of lipophilic residues to achieve an increased ligand-receptor affi nity
- general broadening of the chemical space driven by the use of combinatorial chemistry, and
- introduction and use of high-throughput screening.
This very trend towards candidates with potentially poor oral bioavailability might be further exacerbated by the current interest in the area of polypharmacology and the related use of framework combination methods, which are being applied towards the design of NCEs which hit multiple pharmacological targets simultaneously [14].
While one may look at the continued trend towards more lipophilic drug candidates as both counterintuitive and discouraging, one can also look at it from a diff erent perspective. The breadth of today’s pharmacological targets drives the portfolios of developmental NCEs to rather high heterogeneity. While this comes with certain challenges for the further development of the corresponding drug candidates, the opportunities for the patient likely outweigh the initial drawback. In order to fully exploit these opportunities, the application of developability methods in discovery must be complemented by additional sophisticated methods including salt or co-crystal formation (for recent reviews see [15,16]) and/ or formulation design approaches (see below) in development to minimize overall portfolio attrition and bring more valuable medicines to the patient.
Formulation/Drug Delivery system Design
In case a novel drug substance has favorable physico-chemical and biopharmaceutical properties, e.g. stability, solubility in aqueous media, permeability of biological membranes, suffi cient biological half-life for once-a-day dosing, and a broad therapeutic window, formulation scientists have a substantial array of techniques to choose from and typically focus their development activities on immediate release (IR) dosage forms, such as standard fi lm-coated tablets or hard gelatin capsules.
Controlled Release Dosage Forms
In case the drug at hand has a short biological half-life and/or a narrow therapeutic window, controlled release (CR) dosage forms typically will be at the center of interest of the development team, in order to allow for a reduced dosing frequency and constant plasma concentrations, which can ultimately translate into better patient adherence to the drug regimen and thus contribute to improved patient outcomes.
Since the mid-1960s, various types of CR dosage forms have already been established, including matrix-systems, microspheres, pellets, micro capsules and micro tablets, and (more recently) bio-adhesive drug delivery systems, among others [17]. The aforementioned technologies have been optimized over the years and Ambien® CR (zolpidem tartrate) is one example of several for the application of matrix CR technology. CR systems based on osmotic pressure, like single-chamber osmotic pumps, multi-chamber osmotic pumps and additional types have been established more recently [18]. Glucotrol® XL (glipizide) is an example for an osmotic pump-based system.
Orodisperible Drug Products
The need for rapid drug delivery together with the need for easy-to- swallow oral drugs in certain patient populations (including pediatric and geriatric patients) has triggered an important trend towards orodispersible tablets and films. Significant progress has been made over the past 15 years in this area and the term ‘orodispersible’ meanwhile has been introduced both into the United States Pharmacopeia and into the European Pharmacopeia [19]. Orodispersible tablets are typically un- coated and supposed to disperse in the oral cavity before swallowing within a timeframe of three minutes or less. A multitude of formulation and processing technologies can be applied to produce orodispersible tablets [17] as displayed in Figure 2.
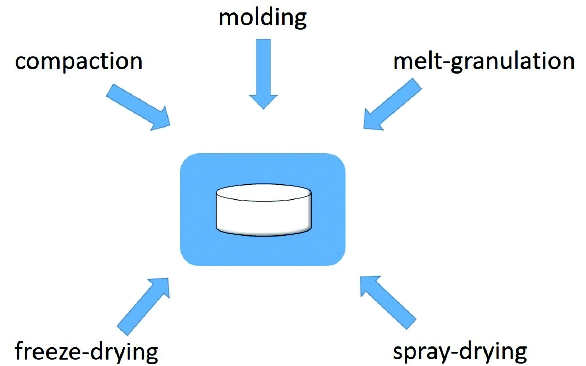 Figure 2. Manufacturing of orodispersible tablets
Figure 2. Manufacturing of orodispersible tabletsOver 25 different orodispersible drugs have been introduced to the market including the tablet product Zyprexa® Zydis (olanzapine) and Zuplenz® (odansentron), the first prescription drug based on an orodispersible film, which was approved by the FDA in 2010 [20].
Formulations for Enhanced Solubility and Bioavailability
Given the increasing percentage of drug candidates with poor aqueous solubility, with up to 90% of NCE candidates belonging to either BCS category II or IV [13], one significant focus of formulation scientists over the past 15 years has been to develop formulations which enable the delivery of the resulting drugs at a reasonable reasonalble rate and extent of oral bioavailability. This has led to the successful market introduction of a notable number of drugs based on various advanced drug delivery technologies, including: formation of solid dispersions (via hot melt extrusion or spay drying), nanocrystal formation via media milling, and the creation of self-emulsifying drug delivery systems (SEDDS). Examples of the successful application of these technologies towards novel medicines include drugs like Kaletra® (ritonavir, lopinavir), Sporanox® (itraconazole), Emend® (aprepipant), and Fortovase® (saquinavir) [21].
Patient-centered Drug Design
Over the past decade, there has been a clear trend to create a better understanding of patient needs and to use the resulting knowledge in the process of designing and developing novel drugs, with the overarching goal of creating improved outcomes for patients.
Furthermore, regulatory expectations, such as the “The Guidance for Industry Q8(R2) Pharmaceutical Development”, request: “In all cases, the product should be designed to meet patients’ needs and the intended product performance” [22]. The specific needs of pediatric and geriatric patient groups have been defined more clearly in the recent past. Correspondingly, regulatory expectations for pediatric drug development have been introduced both in the US [23] and Europe [24].
Beyond the needs of these two patient groups, the specific needs of other groups have been researched as well, including dexterity-impaired patients (e.g. rheumatoid arthritis patients), patients with swallowing problems, patients suffering from visual decline, and patients with inadequate health literacy [25].
Today, scientists take a variety of parameters including patient need into consideration, as they design and develop novel dosage forms [26], see Figure 3.
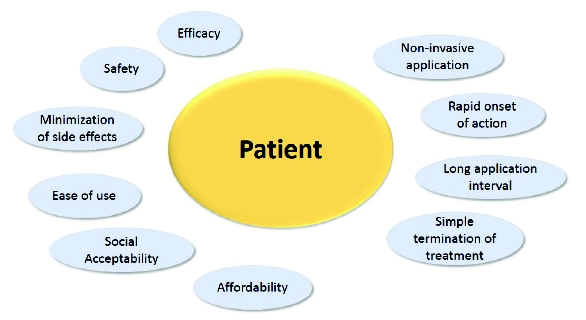 Figure 3. Patient Need Examples
Figure 3. Patient Need ExamplesBasic drug design is typically founded on quality parameters like dose accuracy, purity, and stability as well as on patient needs for safety and efficacy. For specific patient groups, additional needs have to be taken into consideration in order to design for the best achievable outcome. It is crucial to understand these factors well at the outset of the drug development activity. In order to meet some very specifi c patient needs, design elements going beyond drug substance and drug product might need to be optimized, including packaging confi guration, devices, and handling process/instructions.
Examples of newer drugs addressing specifi c patient needs include easy-to-swallow products for patients with swallowing issues, such as the previously mentioned orodispersable fi lm strip Zuplenz® and the orodispersable tablet Zyprexa® Zydis.
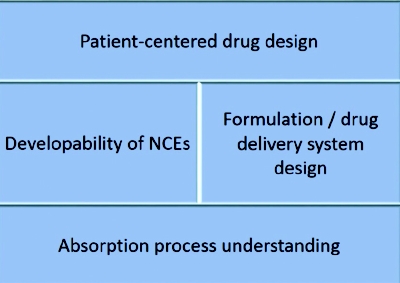
Figure 4. Integrated design of oral medications
Future opportunities
Building on the signifi cant progress achieved in the four aforementioned domains, (absorption process understanding, developability of NCEs, formulation/drug delivery system design, and patient-centered drug design), there is still opportunity for additional advancement of the broader area of oral drug delivery, which can be achieved in particular by more seamlessly integrating development activities across the four domains (Figure 4).
In order to achieve this state, two main principles need to be applied. First, scientists from all domains involved will constantly have to evaluate how their activities infl uence the R&D space of their collaborators in adjacent domains. Second, everyone involved in the development process needs to direct his activities towards maximization of meeting the needs of his patients.
To achieve this, the overall development approach, which in the past was likened to a relay race where the team members pass on the baton, needs to be transformed to a collective approach, comparable to that of a rowing team where all the team members sit in one boat and pull jointly towards the common direction: improved patient outcomes.
Summary
Signifi cant progress has been made over the past 15 years in various domains vital to oral drug delivery including: absorption process understanding, developability of NCEs, formulation/drug delivery system design, and patient-centered drug design. Patients have benefi tted from that progress via the availability of several novel and important medicines. Future innovations can be derived from a more overarching approach in drug development with signifi cant touch points between the aforementioned broader domains and gain better patient outcomes.
Author Biography
Ralph Lipp, Ph.D., is President and CEO of Lipp Life Sciences LLC. Before founding Lipp Life Sciences LLC, Ralph served as Vice President Pharmaceutical Sciences R&D at Eli Lilly and Company and Head Pharmaceutical Development at Schering AG. Ralph holds a degree in Pharmacy from Johannes Gutenberg University in Mainz, Germany, and obtained a Ph.D. in Medicinal Chemistry as well as a Habilitation for Pharmaceutical Technology from Free University Berlin, Germany. His scientifi c contributions comprise over 120 publications, including more than 20 patents, covering 5 marketed medicines.
References
- MarketsandMarkets. North American Drug Delivery Technologies Market 2017. www.beforeitsnews.com.
- GBI Research. Oral Drug Delivery Market Report. Contract Pharma, June 2012.
- R.T.Borchardt. Hidalgo, I. J., Raub, T. J., and Borchardt, R. T.: Characterization of the human colon carcinoma cell line (Caco-2) as a model system for intestinal epithelial permeability. Gastroenterology, 96, 736–749, 1989—The Backstory. AAPS Journal 13(3), 323-327 (2011).
- G.L.Amidon, H.Lennernas, V.P.Shah, J.R.Crison. A theoretical basis for a biopharmaceutic drug classifi cation: the correlation of in vitro drug product dissolution and in vivo bioavailability. Pharm. Res. 12, 413-420 (1995).
- M.N.Martinez, G.L.Amidon. A mechanistic approach to understanding the factors aff ection drug absorption: a review of fundamentals. J. Clin. Pharmacol. 42, 620-643 (2002).
- S.N.Bhattachar, E.J.Perkins, J.S.Tan, L.J.Burns. Effect of gastric pH on the pharmacokinetics of a bcs class II compound in dogs: Utilization of an artificial stomach and duodenum dissolution model and gastroplus,™ simulations to predict absorption. J. Pharm. Sci. 100, 4756–4765 (2011).
- E.S.Kostewicz, B.Abrahamsson, M.Brewster, J.Brouwers, J.Butler, S.Carlert, P.A.Dickinson, J.Dressman, R.Holm, S.Klein, J.Mann, M.McAllister, M.Minekus, U.Muenster, A.Müllertz, M.Verwei, M.Vertzoni, W.Weitschies, P.Augustijns. In vitro models for the prediction of in vivo performance of oral dosage forms. Eur. J. Pharmaceut. Sci. in press (2013).
- R.Borchardt. Drug Design with ADME in mind: recent paradigm shifts in discovery. In C.G.Kruse, H.Timmerman (eds.). Towards Drugs of the Future. IOS Press, 53-74 (2008).
- C.A.Lipinski, F.Lombardo, B.W.Dominy, P.J.Feeney. Experimental and computational approaches to estimate solubility and permeability in drug discovery and development settings. Adv. Drug Deliv. Rev. 23(1-3), 3-25 (1997).
- C.A.Lipinski. Lead- and drug-like compounds: the rule-of-five revolution. Drug Discovery Today: Technologies 1(4), 337-341 (2004).
- J.Baell, M.Congreve, P.Leeson, C.Abad-Zapatero. Ask the Experts: Past, present and future of the rule of five. Future Med. Chem. 5(7), 745-752 (2013).
- R.Panchagnula, N.S.Thomas. Biopharmaceutics and pharmacokinetics in drug research. Int. J. Pharmaceutics 201, 131-150 (2000).
- L.Benet. EDAN. Leuven, Belgium. March 18-20, 2007.
- R.Morphy. Selective multitargeted drugs. In: Polypharmacology in Drug Discovery. J.-U.Peters (ed.) Wiley and Sons, 47-262 (2012).
- A.T.M.Serajuddin. Salt formation to improve drug solubility. Adv. Drug Deliv. Rev., 59(7), 603- 616 (2007).
- B.S.Sekhon, Pharmaceutical co-crystals – a review. Ars Pharmaceut. 50(3) 99-117 (2009).G.M.Khan. Controlled release oral dosage forms: some recent advances in matrix type drug delivery systems. The Sciences 1(5), 350-354 (2001).
- M.Kushal, M.Monali, M.Durgavati, P.Mittal, S.Umesh, S.Pragna. Oral controlled release drug delivery system: an overview. Int. Res. J. Pharmacy, 4(3), 70-76 (2013).
- P.Dey, S.Maiti. Orodispersible tablets: A new trend in drug delivery. J. Nat. Sci. Biol. Med. 1(1), 2–5 (2010).
- M.L.Buck. Alternative forms of oral drug delivery for pediatric patients. Pediatr. Pharm. 19(3), (2013).
- R.Lipp. The innovator pipeline: bioavailability challenges and advanced oral drug delivery opportunities. Am. Pharm. Rev. 16(3), 10-16 (2013).
- www.fda.gov. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER). Center for Biologics Evaluation and Research (CBER), Nov. 2009.
- G.P.Giacoia, P.Taylor-Zapata, A.Zajicek. Eunice Kennedy Shriver National Institute of Child Health and Human Development Pediatrics Formulation Initiative: proceedings from the second workshop on pediatric formulations. Clin. Ther. 34(Suppl.), S1–S10 (2012).
- J.Walsh, S.Mills. Formulating better medicines for children: 4th European Paediatric Formulation Initiative Conference. Ther. Deliv. 4, 21–25 (2013).
- S.Stegemann. Patient centric drug delivery – a changing paradigm in healthcare provision. Health insight 3 – The future of the pharma industry. Apr. 24, 2013, Beirut, Lebanon.
- R.Lipp. Patient-centered design of drug delivery systems. BIT’s 1st annual symposium of drug delivery systems. Nov. 3-5, 2011, Shenzhen, China.