Introduction
According to the popularly cited study from Tufts Center for the Study of Drug Development, it costs $2.6 billion to receive a drug approval.1 Despite the increased investments and revolutionary therapies brought to market, return on investment from drug launches is near historical lows.2 Luckily, issues such as challenging physicochemical properties and unfavorable absorption characteristics can be addressed early in the development process. Screening formulation options in the pre-clinical setting has the potential to reduce both costs and risk of attrition.3
The routine use of high throughput screening and more targeted drugs have contributed to nearly 70% of pipeline drug candidates falling into Class II (poor solubility and good permeability) of the Biopharmaceutics Classification System (BCS). These compounds tend to have poor bioavailability, variable pharmacokinetics, and are subject to food effects. Therapies from non-optimized drug products developed with these compounds can range from sub-therapeutic pharmacotherapy, to cases where patients can be exposed to toxic levels of the drug. Butler and Dressman have proposed a newer Developability Classification System (DCS), which divides BCS Class II into two parts: drugs whose absorption is dissolution rate-limited (IIa); and for those whose absorption is solubility-limited (IIb).4 Whereas the BCS was proposed primarily for use as a regulatory tool, the DCS was created as a developability tool to evaluate and address drug development issues at early development stages through the rational selection of appropriate formulation technologies for these challenging compounds.
This trend for drug candidates to have similar characteristics has driven the increased use of bioavailability enhancement technologies. The most successful approaches have been lipid formulations, solid amorphous dispersions, and particle size reduction.5 Certain API properties often favor one technology over another. Numerous groups have developed in silico prediction tools to choose an optimal formulation technology. However, this a priori approach should be taken more as guidance rather than a steadfast rule. A parallel screening approach at early clinical or pre-clinical stages, instead of a “fit-for-purpose” approach in Phase II, can accelerate development and potentially address efficacy and safety concerns sooner in development
Lipid-Based Drug Delivery System (LBDDS)
Of the above-mentioned bioavailability enhancement technologies, lipid-based formulations are perhaps the most studied and have the longest history of clinical and commercial success. This technology is, in many cases, a favorable option for DCS Class IIa, and preferably for IIb active pharmaceutical ingredients because the drug is both formulated to be in solution when delivered and maintained in solution in the gastrointestinal tract. Pouton et al. first proposed classification of lipid-based formulations into four different categories based on types and ratios of excipients.6 This was later expanded by Porter et al. to include a fifth category of LBDDS.7 The dynamic nature of lipid-based formulations in-vivo requires specialized formulation expertise to perform pre-formulation screening and assessment in the development of lipid-based formulations. The mechanism by which lipid-based formulations enhance bioavailability has been thoroughly reviewed in literature.8-9 Application of a parallel screening approach during development is used to accelerate and choose the best types and combinations of excipients. The expert formulator can begin to incorporate Quality-by-Design (QbD) principles at the pre-formulation stages. Some of the critical parameters of interest would include: screening for solubility in excipients, biorelevant media, and lipid digestion products; excipient compatibility; risk of precipitation upon dispersion and digestion; and API degradation. A key consideration for delivering a LBDDS is that most formulations are liquids or semi-solids having low melting points.
Soft Capsules Are Excellent Delivery Vehicles For Lipid-Based Formulations
There are many papers and articles that not only discuss the scientific merits of the LBDDS, but also their positive outcomes during development, formulation, manufacturing, and clinical phases of development. The clinical and commercial success of a LBDDS is in large part due to the use of soft capsules for their delivery. Soft capsules are excellent delivery vehicles because of the compatibility and versatility they offer. Soft capsules are compatible with a wide range of lipid excipients ranging from highly lipophilic to amphiphilic to hydrophilic properties. The soft capsule shell can be tailored to meet both the needs of the API and fill containing the API (liquid and semi-solid). For example, during encapsulation of soft capsules, the lipid-formulation is filled into the capsule shell with no headspace and hermetically sealed, which protects oxygen sensitive APIs. Importantly, soft capsules do not compromise or alter the performance properties of the lipid fill material in-vivo. Properly formulated soft capsule shells rapidly rupture and dissolve upon administration thus allowing the LBDDS to perform as designed. For a faster onset of action, improved absorption, or reduced variability in absorption, lipid-based formulations in soft capsules are often designed to spontaneously disperse forming very fine, thermodynamically stable emulsions for Immediate Release (IR) of the API. Lipid semi-solids filled into softgels can also be used for IR application as a means of increasing drug loading (i.e., solid solutions/ dispersions) as well as improving stability of unstable APIs (i.e., APIs prone to hydrolysis) by reducing potential for migration of the API or excipients between the fill and the shell. More recently, the use of semisolid fills in soft capsules to achieve Controlled Release (CR) of APIs has been demonstrated.10 By using plant polysaccharide-based soft capsule shells, higher melting point semisolid fills and highly viscous liquids can now be encapsulated at elevated temperatures expanding the range of lipid-based fills available to the formulator. In addition to CR applications, Delayed Release (DR) can be achieved using film coated soft capsule shells. Because soft capsules do not compromise a LBDDS’s performance, whether it is for IR, CR or DR applications, the formulator has the confidence that extrapolation of pre-formulation and formulation study results will apply in the fully developed soft capsule dosage form for commercial marketing.
Another important advantage of using soft capsules for LBDDS is that quantities are readily increased to commercial scale numbers, given that the process parameters obtained during lab-scale and pilot-scale are translatable to larger scale manufacturing. The time for critical process parameter assessment can be much shorter for soft capsules compared to other formulation approaches. This is particularly true for highly potent compounds where doses can be less than 100 mcg and dose uniformity is extremely challenging. By starting with an API in solution, the manufacturing process for soft capsules ensures a highly accurate and reproducible API filling solution during encapsulation. In addition, the history of New Drug Approvals (NDAs) with soft capsule products and lipid-based formulations provides an excellent precedent for US FDA and foreign regulatory agencies’ approval.
Patient acceptance is critical to any commercially successful technology. Soft capsules incorporate many patient-centric factors such as easier swallowability when compared to tablets, they are fast acting, and can incorporate odor and taste masking. There are numerous clinical examples that illustrate how soft gelatin capsules have enabled the commercially viable development of APIs that could not be developed as conventional dose forms. One well known example is the use of purified omega-3 fatty acid esters for the treatment of patients with high triglyceride levels. These are challenging molecules because of their liquid state at ambient temperatures, oxygen instability, and strong odor and taste. It would be very difficult to formulate an API with these characteristics into an acceptable dosage form other than soft capsules.
The case of abiraterone acetate and enzalutamide helps illustrate certain benefits of using a LBDDS compared to traditional formulation techniques. Both drugs are approved for the treatment of metastatic castration-resistant prostate cancer.11-12 Abiraterone acetate inhibits the synthesis of ligands that bind to androgen receptors, while enzalutamide inhibits androgen receptors directly. Both agents appear to be equally effective for patients pre- and post-chemotherapy and are well tolerated.13 Abiraterone acetate and enzalutamide are administered orally, once daily. Because of their similarities, a clinician is likely to choose one agent over the other based on patient factors. Since enzalutamide is known to induce several drug metabolism enzymes (Table 1), patients taking multiple medications may have a higher likelihood of drug-drug interactions. Although abiraterone acetate has relatively minimal drug-drug interaction concerns, it displays pharmacokinetic challenges. It is possible to address these challenges using bioavailability enhancing technologies such as lipidbased formulation.
Table 1. Profile comparison of abiraterone acetate and enzalutamide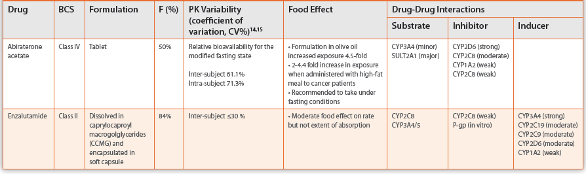
Abiraterone acetate is a BCS Class IV compound (low solubility, low permeability). It has poor absorption, high pharmacokinetic variability, and significant food effect. The combination of these characteristics may raise safety concerns for patients. Abiraterone acetate is commercially available as a conventional tablet formulation. Studies have shown that high-fat meals and formulation in olive oil can increase exposure.11 It is possible that a lipid formulation of abiraterone acetate could improve bioavailability and consequently decrease inter- and intra-subject variability. Enzalutamide is a BCS Class II compound. As mentioned before, lipid-based formulations are favorable options for this class. The lipid formulation of enzalutamide has a high bioavailability, low inter-subject variability, linear dose response, and no food effect. Therefore, the pharmacokinetic profile is likely to be more predictable.
Current Market Landscape For Lipid Based Drug Delivery Systems
Lipid formulations have the longest commercial success track record among enabling technologies measured by the number of NDAs. There are numerous benefits for using a LBDDS for poorly soluble drugs, and the use of soft capsules has enabled their commercial success. A high quality, reputable industry partner is highly desirable for the successful, efficient development, scale-up and commercial manufacturing of soft capsules. It is particularly important to choose a partner that has experience and knowledge to help design an optimal lipid formulation based on the specific physicochemical properties of the API during the pre-clinical stages. An added advantage would be using the same partner for scale-up and commercial manufacturing because the process tends to be more straightforward within the same partner entity or network.
Conclusions
The trend for an increasing percentage of pipeline drugs to fall into BCS Class II requires the use of bioavailability enhancement technologies. Lipid-based formulations have many advantages for lipophilic drugs, and they are also the most studied and have the longest history of commercial success. The commercial and clinical success of lipid formulations is due in a large part to the use of soft capsules as their delivery vehicles. Soft capsules do not impact the performance properties of an LBDDS, can be designed for the specific API requirements, and can be readily scaled to commercial batch sizes. There are several expert companies in the development and commercial soft capsule market. However, considerations such as history of commercial launches, innovation, and scientific knowledge are all important factors when choosing the right partner for successful soft capsule product development and reliable manufacturing supply.
References
- DiMasi JA, Grabowski HG, Hansen RA. Innovation in the pharmaceutical industry: new estimates of R&D costs. Journal of Health Economics 2016;47:20-33.
- Smietana K, Ekstrom L, Jeffery B, Moller M. Improving R&D productivity. Nature Reviews Drug Discovery 2015;14:455-456.
- Basavaraj S, Betageri GV. Can formulation and drug delivery reduce attrition during drug discovery and development- review of feasibility, benefits and challenges. Acta Pharmaceutica Sinica B. 2014;4:3-17.
- Butler JM, Dressman JB. The developability classification system: application of biopharmaceutics concepts to formulation development. J Pharm Sci 2010;99:4940-4954.
- Crew, M. (2014, March 5). Bioavailability enhancement- analysis of the historical use of solubilization technologies. Retrieved April 29, 2016, from http://www.drug-dev.com/ Main/Back-Issues/BIOAVAILABILITY-ENHANCEMENT-Analysis-of-the-Histor-657.aspx
- Pouton CW. Formulation of poorly water-soluble drugs for oral administration: Physicochemical and physiological issues and the lipid formulation classification system. Eur J Pharm Sci. 2006; 29: 278-287.
- Porter CJH, Trevaskis NL, Charman WN. Lipids and lipid-based formulations: optimizing the oral delivery of lipophilic drugs. Nat Rev Drug Discov. 2007; 6: 231-248
- Williams HD, Sassene P, Kleberg K, et al. Toward the establishment of standardized in vitro tests for lipid-based formulations, part 1: Method parameterization and comparison of in vitro digestion profiles across a range of representative formulations. J Pharm Sci. 2012; 101: 3360-3380.
- Williams HD, Sassene P, Kleberg K, et al. Toward the Establishment of Standardized In Vitro Tests for Lipid-Based Formulations, Part 3: Understanding Supersaturation Versus Precipitation Potential During the In Vitro Digestion of Type I, II, IIIA, IIIB and IV Lipid-Based Formulations. Pharm Res. 2013; 30: 3059-3076.
- Bishop CW, Tabash SP, Agudoawu SA, White JA, Crawford KH, Messner EJ, Petkovich PM, inventors; Opko IP Holdings II, assignee. Methods for controlled release oral dosage of a vitamin D compound. United States patent US 8,778, 373. 2014 Jul 15.
- Zytiga® [package insert]. Horsham, PA: Janssen Biotech, Inc; 2012.
- Xtandi® [package insert]. Northbrook, IL: Astellas Pharma US, Inc; 2015.
- Benoist GE, Hendriks RJ, Mulders PFA, et al. Pharmacokinetic aspects of the two novel oral drugs used for metastatic castration-resistant prostate cancer: abiraterone acetate and enzalutamide. Clin Pharmacokinet. 2016 Apr 22. [Epub ahead of print].
- Gibbons JA, Ouatas T, Krauwinkel W, et al. Clinical pharmacokinetic studies of enzalutamide. Clin Pharmacokinet. 2015; 54: 1043-1055.
- Stuyckens K, Saad F, Xu XS, et al. Population pharmacokinetic analysis of abiraterone in chemotherapy-naïve and docetaxel-treated patients with metastatic castration-resistant prostate cancer. Clin Pharmacokinet. 2014; 53: 1149-1160.