With the increase of molecules in development classified by the Developability Classification System (DCS) as Class II (compounds having good permeability but poor solubility) and Class IV (both poorly soluble and poorly permeable), simple formulation approaches like tablets, or powder in a capsule, can lead to suboptimal patient outcomes due to poor oral bioavailability and high pharmacokinetic variabilities. Lipid-based drug delivery systems (LBDDS) are the most well studied and well established formulation approaches for addressing solubility and permeability issues.1
Even though LBDDS are well documented in literature, the pharmaceutical industry has had difficulties moving forward with this technology. There are limited options to deliver these formulations (softgel capsules, liquid filled hard shell capsules, and liquid in bottle), and few pharmaceutical companies or contract development and manufacturing organizations can develop and manufacture lipid formulations in optimal dosage forms.
LBDDS were introduced to the pharmaceutical industry over 80 years ago, and many scientists’ beliefs about its advantages, disadvantages, and limitations have been passed down through generations of developers. However, LBDDS themselves have evolved, and continue to evolve with new excipients, dosage forms, and tests to study their behavior. Many of those pre-conceived beliefs are not completely accurate considering this wealth of additional information. This article will identify scientists’ foremost beliefs about LBDDS, and discuss whether they remain true today.
“The Mechanism of LBDDS is not well-known or can’t be predicted” - MYTH
The in vivo behavior of a LBDDS can be predicted with in vitro tests. There are many in vitro tests to characterize LBDDS, including the assessment of digestion in the gastrointestinal tract (GIT), which presents a simple way to understand the kinetic effect of in situ solubilization of the API, in solution or suspension. This assessment makes it easier to get a whole picture of a LBDDS’ behavior in humans, and the robustness of the formulation.2-4
The introduction of Neoral® in 1995 is a widely cited example illustrating how a self-emulsifying LBDDS can address clinical concerns and result in a product providing a better treatment for patients. This increased pharmaceutical companies’ interest in this technology. The principle behind the lipid-based approach is an increased solubility of an API in lipids compared to its solubility in water.5 When a LBDDS is used to formulate poorly water-soluble drugs, these generally consist of a drug substance and excipients that exist in a solubilized form in gastrointestinal (GI) fluids. This means the formulation initially resists dispersion in GI fluids by maintaining the drug in solution. Afterwards, the lipid components of the formulation can be processed by the lipase and undergo de-esterification. Upon digestion, the API remains in solution. Therefore, lipid systems have the advantage that they can present the drug as a stable liquid solution.
Although a liquid solution is generally preferred, a triglyceride suspension should be considered if a molecule is soluble in digestion but a liquid solution formulation is not achievable for the selected dose.
“LBDDS are only good for solubility enhancement”- MYTH
While the main advantage of LBDDS have been recognized as increasing GI solubility of poorly soluble molecules, it is also increasingly clear that LBDDS may provide other key advantages such as decreasing food effect, increasing permeability and, under some circumstances, avoiding first-pass metabolism, and with some possibilities to influence absorption pathways. For some high LogP drugs, such as testosterone undecanoate (Andriol®), it was seen to limit first-pass metabolism by lymphatic transport.
Some drugs, such as isotretinoin, are required to be taken with food, especially fatty food, because of the high food impact on bioavailability of the drug when taken with fat. Lipid formulation can be used to lessen food effect, resulting in a safer product for patients. Since the API is already well solubilized in lipids, the addition of other fat from food will not have a recognizable impact on the drug absorption and, as a result, the amount of API absorbed will vary less from dose-to-dose.
“LBDDS are only for highly lipophilic molecules” - MYTH
Based on the name, many drug developers think that only lipophilic compounds fit in LBDDS. The term LBDDS refers to a large group of formulations which share some common features. There are 25 commonly used excipients (lipids, surfactants (both of high and low Hydrophile-Lipophile Balance (HLB) values), solvents, co-surfactants and plasticizers) used in LBDDS. These excipients have a wide variety of physicochemical properties and can be combined at different ratios. Depending on the choice and ratio of excipients, LBDDS can be classified and characterized using the Lipid Formulation Classification System (LFCS), as seen in Table 1.8
Table 1. 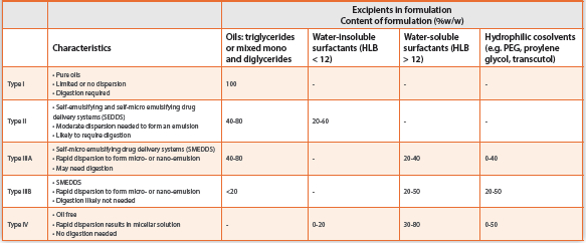
LBDDS is a versatile platform to formulate APIs with a wide range of physicochemical properties,1 from highly lipophilic to highly hydrophilic, and anywhere in between. Hydrophilic compounds can be solubilized in high HLB surfactant or hydrophilic solvent. Moreover, it is also possible to have a formulation with 100 percent surfactant.9 Examples of marketed drugs using such approaches are shown in Table 2.
Table 2. Some examples of marketed products containing hydrophilic fills.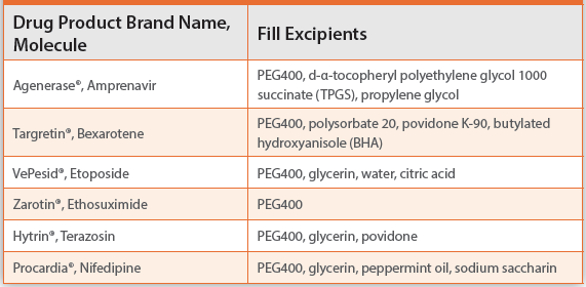
“High drug load, necessarily means large dosage size”- MYTH
For lipid-based formulations, there are several types of development strategies that keep an API solubilized in formulation and during its journey through the gastrointestinal tract (GIT), so that it is able to solubilize the API in situ in the GIT. No matter which strategy is selected, the goal is always to increase bioavailability by levering the API’s solubility in the GIT. In addition, LBDDS also offers more possibilities when the drug load needs to be high. Typically, there is a dose limit of approximately 200 mg per dose form for a lipid-based formulation but when a suspension or, as demonstrated in a recently commercialized formulation, a semisolid formulation can be applied, the drug load could be even higher. Progesterone (Prometrium®) 100 mg and 200 mg soft capsules is micronized as a suspension in peanut oil. However, solubility capacity of intestinal colloidal phases is higher upon digestion of the triglycerides in peanut oil.
Keep in mind that LBDDS are designed to increase bioavailability, which can facilitate a reduction to the drug load whilst still meeting the theoretical drug absorption levels needed. One of the downstream benefits of increased bioavailability, and therefore using lower drug loads is a reduced cost of drug substance manufacture.
“Slow development and high costs” - MYTH
An important advantage of using soft capsules for LBDDS is that quantities may be readily increased to commercial scale, given that the process parameters obtained during lab-scale and pilot-scale are readily translatable to larger scale manufacturing. The time for critical process parameter assessment can be much shorter for soft capsules when compared with other formulation approaches. This is particularly true for highly potent compounds where doses can be less than 100 mcg and where dose uniformity is extremely challenging. By starting with an API in solution, the manufacturing process for soft capsules ensures highly accurate and reproducible API filling during encapsulation. Calcitrol (Rocaltrol®), which is available in 0.25 µg to 0.5 µg softgel capsules, exemplifies this attribute. In addition, the history of New Drug Approvals (NDAs) employing soft capsules and lipid-based formulations provides an excellent precedent for the FDA and other regulatory agencies’ approval. Some people think that it is more complex to develop a LBDDS than other formulations, but overlook that it is often easier and faster to move from lab scale to commercial scale. Moreover, the development incorporates a Quality by Design (QbD)10 approach that requires an increasingly robust characterization of the formulation to de-risk formulation development.
During the pre-formulation stage, solubility and compatibility tests are powerful predictive tools of an API’s physicochemical properties when exposed to different excipients. In early formulation development, QbD can establish relationships between the APIs intrinsic static properties and external variables (e.g., physiologic conditions) that could impact target product quality. Static properties include solidstate properties (e.g., particle size) and physicochemical properties (e.g., solubility). In formulation development, the application of QbD can provide valuable information on critical parameters that affect in vivo behavior of an API, which is essential to provide the optimal formulation strategy, and can save a lot of time by helping in the selection of the best option(s), faster.
A good example is that LBDDS and softgels have been used as the introductory dosage form for many drugs, including lifesaving drugs such as those for anticancer treatments (such as enzalutamide), and protease inhibitors (such as rotinavir and saquinavir).
“LBDDS can provide an optimal release profile” - TRUTH
Immediate release softgel formulations can provide faster onset which, when compared with tablets, is especially valuable for OTC drugs such as allergy and analgesics medications. Since the API is already solubilized in the dose, the absorption process is accelerated as it is unnecessary for the solid dose to first be dissolved in the patient’s body. Extended release can be facilitated by semisolid formulation, and/or extended release coating, to reduce dosing frequency and drug spikes in the blood stream for fewer side effects. A recently launched semisolid softgel product enabled an extended released of calcifediol, a highly potent compound, for the optimal treatment to patients.
“For LBDDS, we should consider liquid filled hard shell (LFHS) capsules first because it is easy, faster and more cost effective” - MYTH
Excipients for LFHS are more limited when compared with softgel capsules and therefore there are fewer options capable of solubilizing challenging molecules. Different commercial instruments are needed for scale up in later phases too, which may cause delays and cost more for the development overall. The ”head-space” (the air gap inside the capsule) needed for two-piece hard shell capsules makes high drug load formulation challenging, which leads to bigger overall capsule sizes and also the possibility that the drug substance is exposed to oxygen inside the capsule. In addition, LFHS are prone to cracking of the hard shell, which impacts both product quality and shelf life.
“LBDDS is only for small molecules” - MYTH
Together, softgels and lipid formulations have helped bring more than 60 NDAs to market, most of which are small molecules. With continued innovation, formulators are incorporating permeation enhancers, surfactants and chelating reagents into lipid formulation in enteric coated softgels, showing very promising progress toward oral administration of biotherapies that would have traditionally been administered to patients by injection. In early trials, proteins and peptides, such as insulin, human growth hormone, calcitonin and recombinant parathyroid hormone display enhanced absorption when delivered in a lipophilic vehicle. Permeation enhancers open tight junctions and increase paracellular passage while various surfactants encourage transcellular transport by disrupting the lipid bilayer. Chelating reagents open tight junctions by chelating to calcium ions present between intestinal epithelial cells. Cyclosporine is already successfully formulated with LBDDS and based on the progress made to date, more protein or peptide drugs in lipids for oral administration are expected in the near future.
“Protection from generics”- TRUTH
A lot of academic research has been conducted on the topic of LBDDS, but there are still only a few pharmaceutical companies that can be considered experts in developing LBDDS formulations and making marketable dose forms (in either soft gelatin capsules or liquid filled hard shells). Although more specialized to develop, LBDDS in softgels may provide better protection from massive generic competition. In addition, applying LBDDS can also be an effective approach for lifecycle management or to expand shelf space with more dose forms available.
Conclusions
As we have discussed, LBDDS is clearly a proven solution to handle molecules with bioavailability issues. We hope to have demystified some of the myths that surround this form of delivery and that may make drug developers consider LBDDS not only as a last chance approach, when in truth it should be evaluated in parallel to other formulation approaches. We hope drug developers can use this important formulation approach to expedite development, and bring more molecules to patients in a patient-preferred dose form.
References
- Savla R, Browne J, Plassat V, Wasan KM, Wasan EK. Review and analysis of FDA approved drugs using lipid-based formulations. Drug Dev Ind Pharm. 2017;43(11):1743-58.
- Bakala-N’Goma JC, Williams HD, Sassene PJ, Kleberg K, Calderone M, Jannin V, et al. Toward the establishment of standardized in vitro tests for lipid-based formulations. 5. Lipolysis of representative formulations by gastric lipase. Pharm Res. 2015;32(4):1279-87.
- Williams HD, Sassene P, Kleberg K, Bakala-N’Goma JC, Calderone M, Jannin V, et al. Toward the establishment of standardized in vitro tests for lipid-based formulations, part 1: method parameterization and comparison of in vitro digestion profiles across a range of representative formulations. J Pharm Sci. 2012;101(9):3360-80.
- Williams HD, Sassene P, Kleberg K, Calderone M, Igonin A, Jule E, et al. Toward the establishment of standardized in vitro tests for lipid-based formulations, part 3: understanding supersaturation versus precipitation potential during the in vitro digestion of type I, II, IIIA, IIIB and IV lipid-based formulations. Pharm Res. 2013;30(12):3059-76.
- Feeney OM, Crum MF, McEvoy CL, Trevaskis NL, Williams HD, Pouton CW, et al. 50 years of oral lipid-based formulations: Provenance, progress and future perspectives. Adv Drug Deliv Rev. 2016;101:167-94.
- Shackleford DM, Faassen WA, Houwing N, Lass H, Edwards GA, Porter CJ, et al. Contribution of lymphatically transported testosterone undecanoate to the systemic exposure of testosterone after oral administration of two andriol formulations in conscious lymph duct-cannulated dogs. J Pharmacol Exp Ther. 2003;306(3):925-33.
- Trevaskis NL, Kaminskas LM, Porter CJ. From sewer to saviour - targeting the lymphatic system to promote drug exposure and activity. Nat Rev Drug Discov. 2015;14(11):781-803.
- Pouton CW. Formulation of poorly water-soluble drugs for oral administration: physicochemical and physiological issues and the lipid formulation classification system. Eur J Pharm Sci. 2006;29(3-4):278-87.
- Gullapalli RP. Soft gelatin capsules (softgels). J Pharm Sci. 2010;99(10):4107-48.
- ICH Harmonized Tripartite Guideline. International committee of harmonization of technical requirements for registration of pharmaceuticals for human use. Q8: Pharmaceutical Development. 2003.
Neoral® is the registered trademark of Sandoz AG
Andriol® is the registered trademark of Merck
Agenerase® is the registered trademark of GlaxoSmithKline
Targretin® is the registered trademark of Eisai
VePesid® is the registered trademark of Bristol-Myers Squibb
Zarotin® is the registered trademark of Pfizer
Hytrin® is the registered trademark of Abbott Laboratories
Procardia® is the registered trademark of Pfizer
Prometrium® is the registered trademark of Abbvie