Introduction
Innovation focused on addressing unmet medical need and improving outcomes for patients is one of the central and overarching goals of the life sciences sector, with significant contributions from large biopharmaceutical companies, biotech and specialty pharma companies, drug delivery companies, and academia. For decades the creation of new medicines has increased quality and quantity of life for patients around the globe. Just looking at the past decade reveals great progress on various fronts, including a 40% reduction of cardiovascular deaths in the US, a significant increase of life expectancy of HIV patients, and the advent of cancer medicine–diagnostic combinations, among others [1]. Scientific breakthroughs leading to novel and valuable medicines are benefiting both patients and their caregivers, and ultimately, society.
However, the resources it takes to develop novel treatments have been steadily increasing over time. Recent estimates vary and range to $1.8bn (capitalized) for the full development of a novel medicine [2], which includes the significant cost stemming from the attrition of developmental drugs from the innovator pipeline. Only one out of approximately 8000 new chemical entities makes it to the market, and the related overall R&D process takes on average approximately 13.5 years [3]. In this context, it has been postulated that the R&D model of the biopharmaceutical industry is broken.
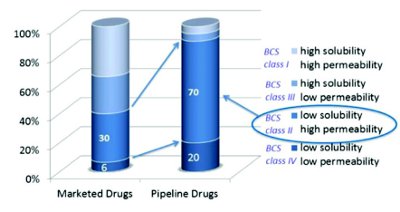
Figure 1. Marketed vs. pipeline drugs: trend toward low solubility
Yet, there is evidence that the pipelines of developmental drugs are getting richer due to the scientific advances of the past decade, and that significant opportunity to create novel treatments that address unmet medical need lies ahead of us. However, one enormous challenge to overcome is the trend toward low solubility drug candidates, which often translates into their low intrinsic bioavailability and can ultimately lead to the attrition of the respective candidates.
This article discusses the solubility-driven bioavailability challenge of innovator pipeline drug candidates and highlights the opportunities that present themselves upon utilization of advanced oral drug delivery technologies.
The innovator pipeline predominantly contains low solubility drugs
Most drugs in use today are applied via the oral route of administration, which is the preferred route for most patients and many indications. Looking at the portfolio of developmental drugs slated for oral administration in comparison to marketed drugs, it becomes evident that there is a strong trend towards drug candidates with low aqueous solubility (Figure 1).
Figure 2 shows that approximately 90% of pipeline drugs fall into the two low solubility categories of the Biopharmaceutical Classification System (BCS), i.e. classes II & IV [4] (volume of water to dissolve a single dose exceeds 250 mL). This is a significant increase when compared to the less than 36% of marketed drugs falling into these two classes. Low solubility of drug candidates can translate into poor (and varying) bioavailability, it can slow down the overall development process, can lead to the development of a suboptimal drug for the patient, or even to its attrition from the pipeline, thus contributing to the increasing cost of drug development cited above.
The effect of low aqueous solubility of a drug on its bioavailbility

Figure 2. Fate of water soluble drugs during passage of the GI tract
Most water soluble drugs, as long as their permeability and metabolic inertness is sufficient, can penetrate biological membranes during the passage of the GI tract and ultimately become bioavailable (Figure 2).
Insoluble drugs generally will not become bioavailable after oral ingestion (Figure 3), and low solubility drugs, like those belonging to BCS class II, will typically show poor and in cases varying bioavailability.
Advanced oral drug delivery technologies
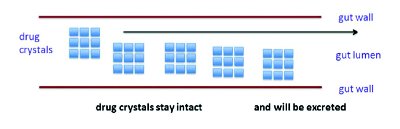
Figure 3. Fate of insoluble drugs during passage of the GI tract
One of the main questions for the drug delivery scientist applying advanced formulation design to a specific BCS class II drug candidate is how to effectively decouple the low intrinsic solubility of the active in the GI tract from the often resulting poor bioavailability. At a conceptual level, the remedy to address this challenge seems to be simple. The crystal lattice of the drug substance needs to be disrupted at the formulation stage. However, reducing this concept to practice and in parallel designing a patient-centered as well as sufficiently stable product is not easy at all, and the formulation scientist needs to work with high sophistication toward this goal. Advanced experimentation approaches tailored to the characteristics of the specific drug substance to be formulated need to be employed, and success is not guaranteed.
Several technologies to disrupt the crystal lattice of drug candidates have been described [5,6], and Figure 4 shows the use of four different routes in principle.
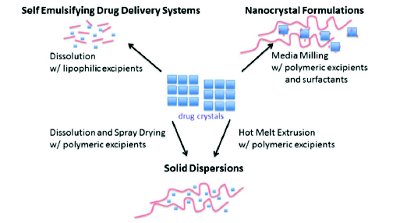
Figure 4 . Technologies to disrupt the crystal lattice of drug substances leading to various drug product intermediates
Formation of Self Emulsifying Drug Delivery Systems (SEDDS) by dissolving the drug substance in lipophilic and/or amphiphilic excipients/excipient mixtures typically is done with concurrent application of heat [7]. The resulting SEDDS intermediate can then be filled into soft or hard gelatin capsules to yield the fi nal dosage form. Creation of nanocrystals via media milling results in a significant increase of the surface area of the drug substance, and in turn, often leads to a profoundly increased dissolution rate of the drug in the GI tract. In order to reduce the risk for agglomeration of the crystals and to improve wetting, suitable excipients will be added to form the nanocrystal formulation intermediate.
Creation of solid dispersions via Hot Melt Extrusion (HME) is done in a continuous manufacturing process utilizing extrusion equipment where physical mixtures of drug substance and polymeric excipients like povidone will be subjected to heat and high shear forces resulting, upon cooling, in the solid dispersion intermediate.
Formation of solid dispersions via spray drying starts with the preparation of a solution of the drug substance together with suitable polymeric excipients like hypromellose acetate succinate in solvents/ solvent mixtures. These solutions are subsequently subjected to a spray drying process, which yields the solid dispersion intermediate.
It is important to note that the aforementioned intermediates still need to be converted to fi nal dosage forms – e.g. tablets, capsules, etc. – to be acceptable for use by the patient. Figure 5 shows the integrated three-step process for the creation of a tablet via a spraydried solid dispersion intermediate. It is important to note that the patient will be able to apply what looks and can be handled like a conventional tablet with all the advantages that come with this well-established dosage form, and will additionally benefi t from the drug’s reliable bioavailability due to application of advanced oral drug delivery technology.
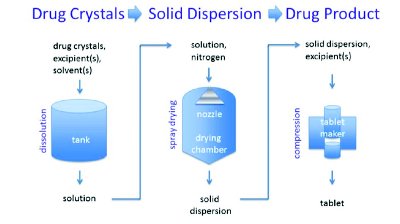
Figure 5. Integrated three step manufacturing process of solid dispersion based tablets
Disrupting the crystal lattice of the drug substance is necessary but not sufficient to design a product of acceptable quality, stability, and in vivo performance to meet the needs of the patient. Manufacturability considerations play a significant role in that physico-chemical attributes of the drug substance, particularly melting point and solubility (process solvents) can limit the use of certain technologies. The application of HME can be difficult for drugs with a melting point of over 200 °C.
Furthermore, amorphous drug substances or solid dispersions obtained from either HME or spray drying must be stabilized against crystallization during shelf life of the fi nal drug product, which typically should be at least two years at 25 °C. Sophisticated formulations based on suitable excipients/excipient combinations need to be developed to guarantee storage stability of the drug product and thus usability by the patient.
Table 1 . Examples of advanced oral drug delivery products

Even if manufacturability, shelf life/stability, and high initial drug solubility in the GI tract can be achieved, sufficiently high and reliable bioavailability is still not guaranteed in case precipitation of the drug substance in the GI tract occurs. In order to avoid this phenomenon, a new approach – named “spring and parachute approach” [8] – has been discussed more recently.
Product examples
Table 1 provides product examples related to the four different aforementioned manufacturing technologies.
A closer look at sophisticated formulations for saquinavir [9] and aprepitant [10] shows that the enhancement of their relative bioavailability lies in the range of approximately 3 to 4 fold (Figure 6). For aprepitant, utilization of nanocrystal technology enabled the drug, in other words, application of advanced oral drug delivery saved the drug from attrition, and ultimately made it available to the patient. In the case of saquinavir, the SEDDS formulation provided an improvement over the previously marketed standard formulation in the sense of a life cycle management geared towards patient benefits.
Novel excipients – need and opportunity
While oral drug delivery systems on the market today typically are built on the usage of well accepted excipients, research has shown that there is a need for a new generation of excipients to enable novel medicines, excipients that combine drug product manufacturability with various in vivo performance characteristics. However, the development of any new excipient, the recent development of a polyethylene glycol-vinylcaprolactam-vinylacetat co-polymer [11], takes significant resources and up to seven years [12]. The very need for novel excipients also presents itself as an opportunity for collaboration between excipient manufacturers, regulators, and pharmaceutical companies to create, control, and apply the use of these important materials.

Figure 6. Advanced oral drug delivery leading to increased bioavailability of poorly soluble drugs
Future excipients will strengthen the toolkit of the advanced oral drug delivery scientist and help to save more of the promising drug candidates in the innovator pipeline from attrition, for the ultimate benefi t of the patient.
Conclusion
There has been a significant trend in the innovator pipeline towards low solubility drug candidates with an inherent risk for poor bioavailbility, and a heightened risk for attrition from the innovator pipeline. Sophisticated application of advanced oral drug delivery technologies supported by versatile excipients is enabling many of these drug candidates. This results in tangible patient benefi ts and contributes to the overall value creation by the innovator.
Author biography
Ralph Lipp, Ph.D., is President and CEO of Lipp Life Sciences LLC. Before founding Lipp Life Sciences LLC, Ralph served as Vice President Pharmaceutical Sciences, R&D, at Eli Lilly and Company and as Head of Pharmaceutical Development at Schering AG. Ralph holds a degree in Pharmacy from Johannes Gutenberg University in Mainz, Germany, and obtained a Ph.D. in Medicinal Chemistry as well as a Habilitation for Pharmaceutical Technology from Free University Berlin, Germany. His scientific contributions comprise over 120 publications, including more than 20 patents, covering 5 marketed medicines.
References
- L.Cox, P.Peck. The top ten medical advances of the decade. MedPage Today, December (2009).
- S.Morgan, P.Grootendorst, J.Lexchin, C.Cunningham, D.Greyson. The cost of drug development: a systematic review. Health Policy 100(1), 4-17 (2011).
- S.M. Paul, D.S. Mytelka, C.T. Dunwiddie, C.C. Persinger, B.H. Munos, S.R. Lindborg, A.L. Schacht. How to improve R&D productivity: the pharmaceutical industry’s grand challenge. Nature Reviews Drug Discovery 9, 203-214 (2010).
- L. Benet. EDAN. Leuven, Belgium. March 18-20, 2007.
- C.Timpe. Drug solubilization strategies applying nanoparticulate formulation and solid dispersion approaches in drug development. Am. Pharm. Review, January (2010).
- K.T. Savjani, A.K. Gajjar, J.K. Savjani. Drug solubility: importance and enhancement techniques. ISRN Pharmaceutics, Article ID 195727 (2012).
- C.Brüsewitz, A.Schendler, A.Funke, T.Wagner, R.Lipp. Novel poloxamer-based nanoemulsions to enhance the intestinal absorption of active compounds. Int. J. Pharm. 329(1-2), 173-81 (2007).
- P.Augustijns, M.E.Brewster. Supersaturating drug delivery systems: fast is not necessarily good enough. J. Pharm. Sci. 101(1), 7-9 (2012).
- www.dailymed.nlm.nih.gov
- Y.Wu, A.Loper, E.Landis, L.Hettrick, L.Novak, K.Lynn, C.Chen, K.Thompson, R.Higgins, U.Batra, S.Shelukar, G.Kwei, D.Storey. The role of biopharmaceutics in the development of a clinical nanoparticle formulation of MK-0869: a Beagle dog model predicts improved bioavailability and diminished food effect on absorption in human. Int. J. Pharm. 285(1-2):135-46 (2004).
- N.Langley. The role of polymeric excipients in bioavailability enhancement. DCAT Week ’13. New York, NY. March 14, 2013.
- K.Kolter. Novel excipients: A rare species. Pharm. Technol. Eur. 23 (10) (2011).