Introduction
Rapid and consistent in-vivo drug dissolution is critical for drug absorption. In-vitro dissolution tests are used to predict in-vivo disintegration and dissolution properties of drug products. The in-vitro disintegration and dissolution times of tablets and capsules can vary significantly based on their composition and processing. Though small differences in-vitro dissolution are not expected to result in significant in-vivo performance differences, the slight in-vitro dissolution delay observed by over-encapsulation for double blind clinical trials, as well as switching from gelatin to HPMC capsules often raises concerns on the potential impact on in-vivo bioavailability. While it is accepted that the in-vitro dissolution delay of about 5 minutes caused by overencapsulation with gelatin capsules of immediate release (IR) tablets or powder formulation does not lead to non-bioequivalence, no data on bioequivalence exist for over-encapsulation with an HPMC capsule having a dissolution lag time of around 10 minutes. To assess the potential impact, a comparative investigation was performed using invitro dissolution, PK simulation and human bioequivalence comparing an IR fixed dose combination compressed caplet containing three different rapidly-absorbed drugs over-encapsulated with gelatin capsules and the same caplet over-encapsulated with HPMC capsules made by a thermo-gelation process.
Two piece hard gelatin capsules (HGC) have been used to deliver medicines and nutritional supplements for over 80 years (Colton, 1931). These types of HGCs are well-described in pharmacopoeial monographs and in the literature and their in-vitro and in-vivo behavior has been extensively characterized. Due to their reliable IR performance, HGCs are widely used for a variety of formulations and delivery applications [Stegemann 2011, Cole et al, 2008, Deepthi & Murthy, 2015].

The plant-derived polymer hydroxypropyl methyl cellulose (HPMC) has been used in pharmaceutical and nutritional products for many years as an excipient for drug product formulation and coating applications. HPMC capsules are an alternative to HGCs, and were originally manufactured by addition of a gelling system using a gelling agent (e.g. carrageenan, gellan gum) and gelling promoter (e.g. potassium acetate, potassium chloride) to form the capsule shell. HPMC capsules produced by newly-developed thermo-gelation processes without the addition of gelling systems were introduced later and have been commercially available for some time (Al-Tabakha, 2015, Cade & He 2010). The physical and chemical properties of HPMC address some limitations of gelatin, enabling the application of capsule technology to a broader range of drug products and formulations. Specifically, HPMC allows incorporation into capsules ingredients that are chemically incompatible with gelatin, hygroscopic or sensitive to moisture. Studies have demonstrated differing in-vitro dissolution profiles for HGCS and different types of HPMC capsules (Gabacza et al. 2014, Honkanen et al, 2001; Vardakou et al 2011). The dissolution profiles of HPMC capsules depend on the capsule formulation and manufacturing process. HPMC capsules using either carrageenan or gellan gum as a gelling agent show a pH and ionic strength dependent dissolution behavior which was not the case for HPMC capsules made by a thermo-gelation process [Ku et al 2011]. It has been shown that the bioavailability is comparable between gelatin, HPMC capsules containing gelling agents and HPMC capsules made by thermogelation for IR products [Ku et al. 2010; Cole et al 2004].
Study Design
Two dosage forms were prepared: 1) Excedrin® Extra Strength (Novartis Consumer Health) caplets each containing Acetaminophen/ Acetylsalicylic acid/ Caffeine 250/250/65 mg were over-encapsulated in a standard size 00 hard gelatin capsule (Capsugel, France ) and 2) the same Excedrin caplets were over-encapsulated in HPMC capsules manufactured by a thermo-gelation process without secondary gelling agents (Vcaps® Plus, Capsugel, France). The in-vitro dissolution of the over-encapsulated caplets were performed according to the USP-29 monograph for “acetaminophen, aspirin and caffeine tablets” using a USP dissolution apparatus 2 at 100 rpm and 900 ml water at 37° C ± 0.5° C. Samples were taken after 10, 20, 30, 45 and 60 min., and analyzed by HPLC for acetaminophen, acetylsalicylic acid and caffeine.
PK simulations of all three compounds were performed using GastroPlus software version 9.0. We report here only the results for acetaminophen as its predicted PK was the most sensitive to the input release profile. Clearance, volume of distribution, and number of compartments were fit to the measured mean plasma concentration versus time data for the two over-encapsulated dosage forms, and the physicochemical properties of acetaminophen were calculated using Simulations Plus ADMET predictor version 7.1. Dissolution kinetics were fit to in vitro dissolution data using a Weibull model equation
where R is the percent of drug released, Rmax is the maximum percentage of drug released, t is the time in hours, T is the lag time, b is a shape factor, and A is a kinetic or time scale parameter.
The bioequivalence study was a single-center, open label, single dose, randomized 2-way crossover in 24 male healthy subjects aged 18 – 45 years under overnight fasted conditions characterized in Table 1.
Table 1. Physical characteristics of the 24 males enrolled in the in vivo bioequivalence study

samples for the determination of acetaminophen, acetylsalicylic acid, total salicylate, and caffeine, were collected before receiving the over-encapsulated caplets in either gelatin or HPMC capsules with 240 mL water and 20 and 40 minutes and 1, 1.5, 2, 3, 4, 6, 8, 10, and 12 hours post dose.
Plasma Cmax, AUC0-t and AUC0-∞ of acetaminophen, acetylsalicylic acid, total salicylates and caffeine were considered as the primary pharmacokinetic parameters to establish bioequivalence between the two over-encapsulated products. According to the regulatory requirement for bioequivalence, an acceptance range of 80.00 to 125.00% was defined.
Results
In-vitro dissolution
The dissolution data for Excedrin® Extra Strength caplets and the two types of over-encapsulated caplets in gelatin and HPMC capsules are provided in Figure 1.
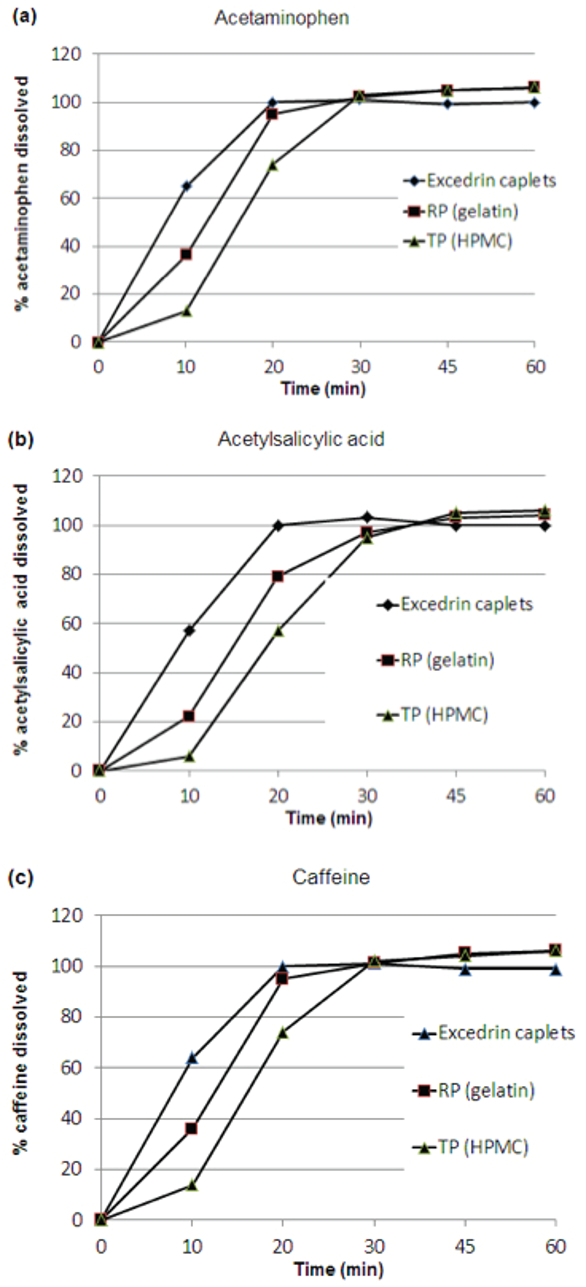 Figure 1. In-vitro dissolution profiles of acetaminophen (a), acetylsalicylic acid (b) and caffeine (c) from two Excedrin® Extra Strength caplets, RP (over-encapsulated in gelatin capsules) or TP (over-encapsulated in HPMC capsules) in USP apparatus 2 in water 37° C ± 0.5° C at 100 rpm
Figure 1. In-vitro dissolution profiles of acetaminophen (a), acetylsalicylic acid (b) and caffeine (c) from two Excedrin® Extra Strength caplets, RP (over-encapsulated in gelatin capsules) or TP (over-encapsulated in HPMC capsules) in USP apparatus 2 in water 37° C ± 0.5° C at 100 rpmThe results show that the APIs had slower release from the overencapsulated product than from the unencapsulated caplets. Release from the HGC over-encapsulated dosage form was delayed by about 5 minutes and release from the HPMC over-encapsulated dosage form was delayed by about 10 minutes relative to that of the unencapsulated caplet. After 30 minutes, 95% of acetylsalicylic acid, acetaminophen and caffeine were released for all 3 dosage forms.
PK simulations
PK simulations were used to predict the impact of the slightly delayed release of active caused by over-encapsulation with the two types of capsules on the average plasma concentrations of each active. The in-vitro dissolution profiles shown in Figure 1 were fit to a Weibull equation. The dissolution lag time, which is representative of the capsule rupture time, was varied in the simulations. Results are shown only for acetaminophen as its predicted PK profile is most sensitive to the input release rate due to its fast absorption and clearance. Simulation results are overlaid with average measured plasma concentrations and presented in Figure 2. The simulations predicted nearly identical plasma concentration versus time profiles for the two over-encapsulated dosage forms, resulting in no significance difference in Cmax, Tmax or AUC.
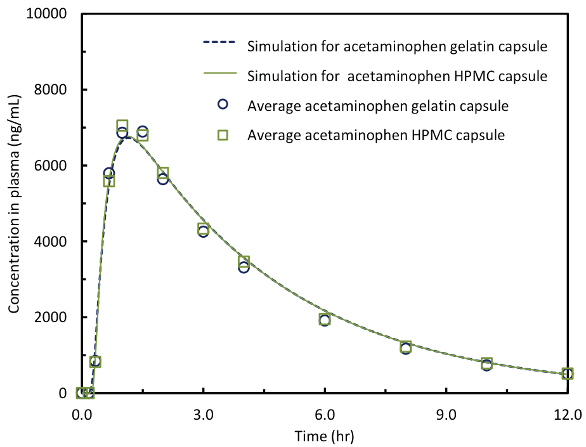 Figure 2. In-vivo and simulation concentration versus time comparisons for acetaminophen in HPMC and gelatin capsules.
Figure 2. In-vivo and simulation concentration versus time comparisons for acetaminophen in HPMC and gelatin capsules.Figure 3 shows the predicted sensitivity of three PK parameters, Cmax, Tmax and AUC, on the input dissolution lag time. These simulations compared the predicted PK profiles to the PK profile of the reference acetaminophen formulation. These simulations predict, as expected, that Tmax increases linearly with increasing dissolution lag time but almost no difference in Cmax and AUC for lag times up to 120 minutes. Thus, it is expected that small differences in dissolution time lag of the magnitude measured for over-encapsulation – on the order of only 5 to 10 minutes – should have negligible impact on PK.
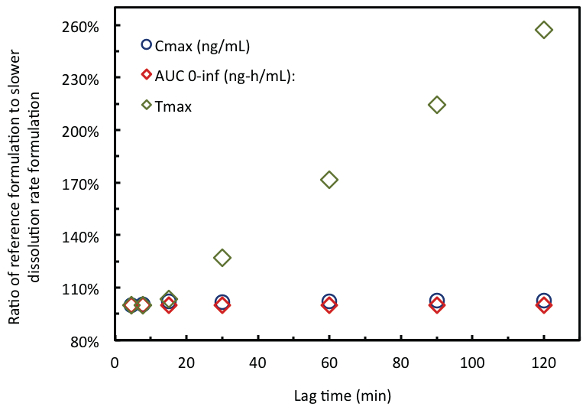 Figure 3. PK simulation results for acetaminophen with increasing dissolution rate lag time.
Figure 3. PK simulation results for acetaminophen with increasing dissolution rate lag time.In-vivo pharmacokinetic data and bioequivalence analysis
Cmax, AUC0-t and AUC0-∞ for acetaminophen, acetylsalicylic acid, total salicylates and caffeine of the over-encapsulated caplets in HGC and HPMC capsules are shown in Figures 4a-d and Table 2. The rate and extent of absorption of all three model drugs dosed as the two different dosage forms is essentially identical, with no statistical difference for all of the pharmacokinetic parameters investigated.
 Figure 4a. Mean in vivo acetaminophen plasma concentration released over 12 hours.
Figure 4a. Mean in vivo acetaminophen plasma concentration released over 12 hours.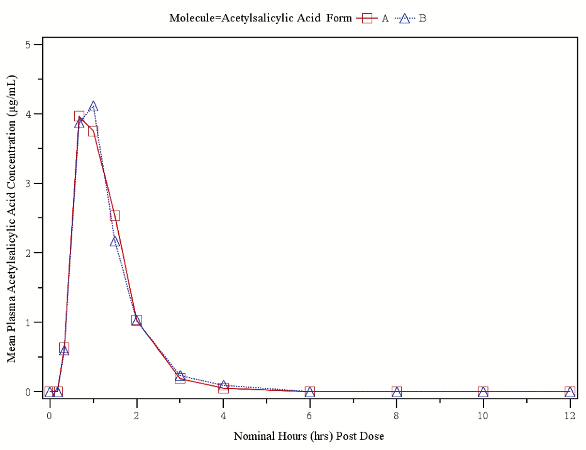 Figure 4b. Mean in-vivo acetylsalicylic acid plasma concentration released over 12 hours.
Figure 4b. Mean in-vivo acetylsalicylic acid plasma concentration released over 12 hours.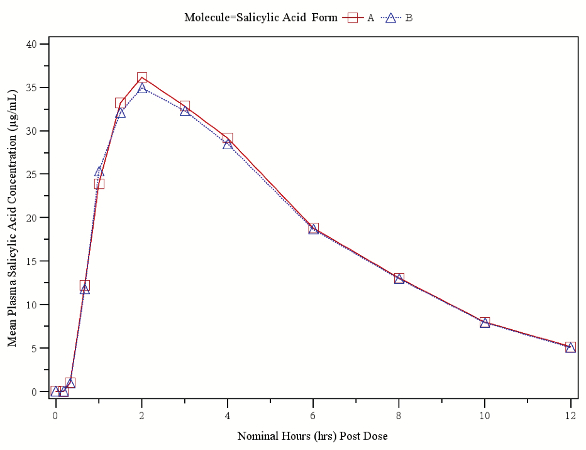 Figure 4c. Mean in-vivo total salicylates plasma concentration released over 12 hours.
Figure 4c. Mean in-vivo total salicylates plasma concentration released over 12 hours.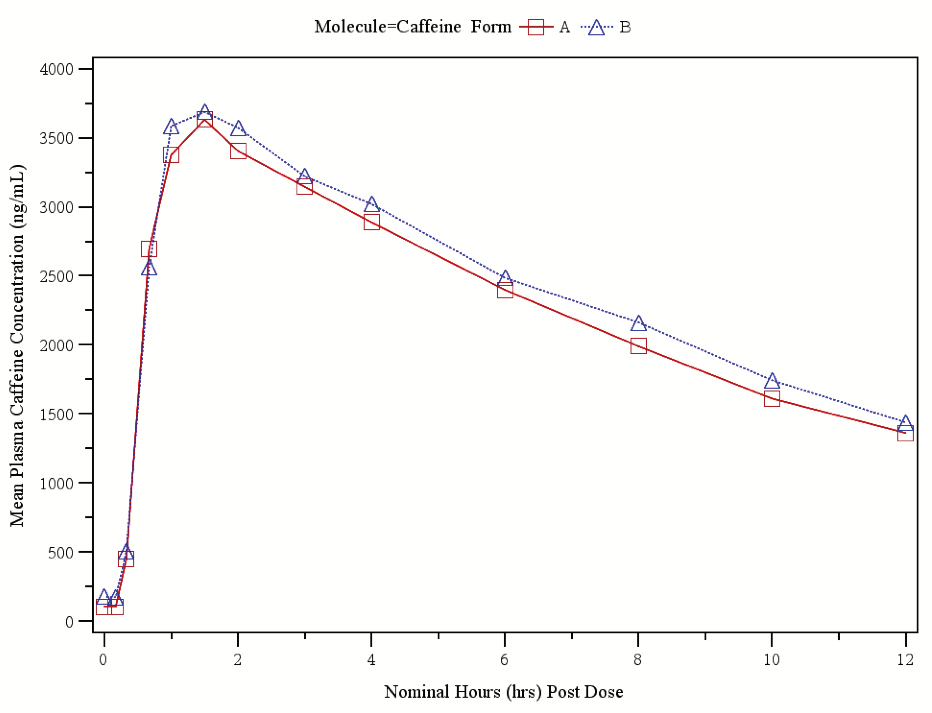 Figure 4d. Mean in-vivo caffeine plasma concentration released over 12 hours.
Figure 4d. Mean in-vivo caffeine plasma concentration released over 12 hours.Table 2. Mean pharmacokinetic parameters including standard deviations of acetaminophen, acetylsalicylic acid, total salicylate and caffeine (N=24) released from gelatin and HPMC capsules. The 90% CI for Cmax, AUC0-t and AUC0-∞ were within 80.00-125.00% range.

Statistical analysis confirmed that the 90% CI the 90% CI for Cmax, AUC0-t and AUC0-∞ are well within the range of 80 -125.00% acetaminophen, aspirin (acetylsalicylic acid, total salicylates) and caffeine for comparison of the gelatin over-encapsulated caplet and the HPMC capsule over-encapsulated caplet (Tables 3a-d).
Table 3a. Statistical analysis results for the assessment of bioequivalence of acetaminophen (N=24)

Table 3b. Statistical analysis results for the assessment of bioequivalence of acetylsalicylic acid (N=24)
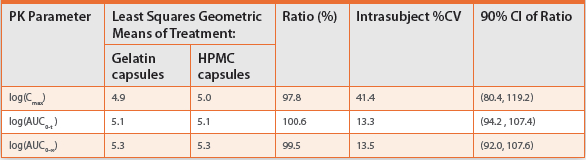
Table 3c. Statistical analysis results for the assessment of bioequivalence of total salicylates (N=24)
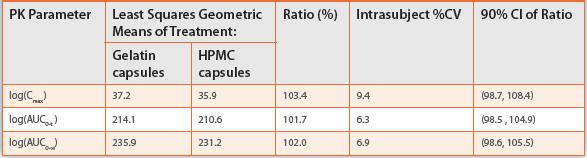
Table 3d. Statistical analysis results for the assessment of bioequivalence of caffeine (N=24)

Further analysis from the mixed model analysis (Table 4), demonstrated that there were no sequence effects on Cmax and AUC of acetaminophen, aspirin (acetylsalicylic acid, total salicylates) and caffeine, as no statistical difference was found at the 10% level of significance. This data suggests that drug release and absorption from HGC and HPMC capsules for the three model compounds are comparable and meet the PK criteria for bioequivalence.
Table 4. Statistical analysis results from mixed model analysis of acetaminophen, acetylsalicylic acid, total salicylates and caffeine (N=24)

Discussion
There are various types of commercial two-piece HPMC capsules having different formulations and manufacturing processes, providing distinct in-vitro and in-vivo characteristics. HPMC capsules manufactured by the traditional dipping process include a gelling system composed of gelling agent or polymer (carrageenan or gellan gum) and a gelling promoter (potassium chloride or potassium acetate) [Cole et al 2004]. The dissolution performance of these HPMC capsules depends on the pH and ionic strength of the media [Cole et al 2014; Honkanen et al 2001; Ku et al 2011]. The potential impact of these dissolution differences on the in-vivo performance in patient populations is still unclear. However, it has been suggested to avoid administration of drug products in such capsules with carbonated drinks like Coca Cola [Chiwele et al 2000].
In contrast, HPMC capsules manufactured from pure HPMC (no gelling agent added) using a thermo-gelation process have dissolution profiles independent of pH and ionic strength of the dissolution media [Groshens et al 2009; Kilic et al 2009; He et al 2012].
For double blind clinical trials, overencapsulation of IR products with HGCs is used for blinding purposes. The short lag-time generated by the encapsulation of the tablets – on the order of 5 minutes - is seen in the invitro dissolution profiles of over-encapsulated tablets [Esseku et al 2010]. in-vivo studies using gamma-scintigraphy to determine capsule initial and complete disintegration and bioequivalence and pharmacodynamic endpoints between an encapsulated and non-encapsulated IR tablets have shown that IR tablets can be used as sensitive markers for the evaluation of the impact of capsules on the in-vivo performance [Goates et al 2000; Sikes et a 2003; Wilding et al 2005].
Acetaminophen, acetylsalicylic acid and caffeine have good aqueous solubility and high permeability and therefore are Class 1 drugs according to the BDDCS classification. [Benet et al 2011]. The three compounds are known to have short Tmax values between 0.5 and 2.0 h and the Excedrin® Extra Strength caplets release more than 90% of the three actives within 5 minutes, and 100% within
15 minutes, according to the FDA product review [FDA 1998]. To evaluate the impact of the two different capsules on in-vivo performance, the Excedrin® Extra Strength caplets were selected for the study, as the release of the caplets from the capsule is the critical parameter for in-vivo dissolution and absorption of all three drugs.
The in-vitro dissolution profiles of acetaminophen, acetylsalicylic acid and caffeine were performed in purified water according to the FDA monograph for ‘acetaminophen, acetylsalicylic acid and caffeine’ fixed dose combination tablets [USP 29] and applied for the Excedrin® Extra Strength caplets filing in 1997 [FDA 1998]. The in-vitro dissolution profiles of the Excedrin® Extra Strength caplets in this study were slower than the data reported in the registration for the caplet version, but comparable to the dissolution data reported for the Geltab version [FDA 1998].
The in-vitro dissolution of the three APIs demonstrated a delay in dissolution of about 5 minutes for the HGC over-encapsulated caplet and a delay of about 10 minutes for the HPMC capsule over-encapsulated caplet compared to the non-encapsulated caplet. However, greater than 95% of the active was released for all 3 dosage forms after 30 minutes, in agreement with the previously reported dissolution data, and attributable to the slightly longer rupture time for HGC (2-3 minutes) and HPMC capsules (8 minutes) [Ku et al 2011].
The AUC0-t, AUC0-∞, AUC0-t/ AUC0-∞, Cmax and Tmax of acetaminophen, acetylsalicylic acid, total salicylate and caffeine in gelatin and HPMC capsules in the healthy volunteers were all comparable. The statistical analysis of the acetaminophen, acetylsalicylic acid, total salicylate and caffeine values, and mixed model analysis between these compounds did not reveal any significant difference between HGC over-encapsulated caplets and HPMC capsule over-encapsulated caplets using a 90% confidence interval of the ratio. The results met the criteria for bioequivalence between the reference product and test product.
These results were consistent with the acetaminophen PK simulations, shown in Figure 2. These simulations were used to assess the impact of dissolution profile on the predicted plasma concentration versus time profiles. The simulations predicted there should be no significant difference in AUC, Cmax, or Tmax due to the small difference in release and dissolution. A series of simulations was conducted using dissolution profiles with longer lag times. As shown in Figure 3, lag times as long as 120 minutes were predicted to have essentially no impact on AUC and Cmax. This is expected as acetaminophen is highly permeable and its rate and extent of absorption is not expected to be sensitive to position in the small intestine. However, as expected, Tmax was predicted to linearly increase with the dissolution lag time input for dissolution lag times longer than about 15 minutes, the average gastric emptying time for a human in the fasted state [Dressman et al 1986]. Specifically, the simulation predicts that the release lag time – and presumably capsule rupture time - would have to be longer than 25 minutes before a 20% change in Tmax would be expected to be observed.
The findings agree with recent clinical data showing that in-vivo in the fasted state, HPMC and gelatin capsule formulations of afuresertib are bioequivalent [Lickliter et al. 2014]. That study indicated that food can increase the in-vivo bioavailability of afuresertib in HPMC capsules and this is an area for future research, where dissolution testing could be used to explore the potential for achieving increased bioavailability.
For certain applications, one might expect differences in in-vivo performance between the same active and formulation dosed in HGC versus HPMC capsules. Examples include:
- applications where acid soluble drugs (e.g. weak bases) may show a difference in extent of absorption due to differences in gastric exposure due to differing capsule shell dissolution rates;
- applications where there is potential for API conversion to a low energy form during gastric exposure;
- formulations which may be particularly prone to gelation during capsule shell dissolution, which can result in slow API dissolution from the gel; and
- applications involving low solubility weakly basic APIs, where the HPMC from the capsule shell may act beneficially as a crystallization inhibitor. (Ouellet, et al. 2013).
Conclusions
The comparative in-vivo study between 1) an IR compressed caplet over-encapsulated with a standard gelatin and 2) the same IR compressed caplet over-encapsulated with an HPMC capsule manufactured by a thermo-gelation process (without the use of secondary gelling agents) has demonstrated equivalent performance for all three BDDCS class 1 drugs contained in the caplet.
Bioequivalence was achieved for acetaminophen, acetylsalicylic acid, total salicylate and caffeine on the PK parameters of AUC, Cmax and Tmax in the plasma sampled from 24 fasted human subjects for the reference product (Excedrin® Extra Strength caplets over-encapsulated in gelatin capsules) and test product (Excedrin® Extra Strength caplets overencapsulated in HPMC capsules made by a thermo-gelation process).
These findings provide evidence that HGC and HPMC capsules containing IR formulations of water soluble, rapidly absorbed drugs perform similarly in-vivo in young, healthy, fasted subjects yielding essentially identical pharmacokinetic parameters. The bioequivalence according to the FDA Guidelines established for the Excedrin® Extra Strength caplets over-encapsulated in either HGC of HPMC capsules made by the thermo-gelation process confirmed that the pharmacokinetics for these two capsules is essentially identical for acetaminophen, acetylsalicylate, and caffeine. The 5 minutes longer lag time in the in-vitro dissolution observed for the HPMC capsule over-encapsulated dosage form relative to the HGC overencapsulated dosage form did not lead to a significant difference in in-vivo pharmacokinetics.
References
Al-Tabakha M.M., Arida A. L.., Fahelelbom K.M., Sadek, B., Saeed, D.A., Abu, Jarad, R.A., Jawadi, J. 2015. Influence of capsule shell composition on the performance indicators of hypromellose capsule in comparison to hard gelatin capsules. Drug Dev. Ind. Pharm. 14, 1-12.
Benet, L.Z., Broccatelli, F., Oprea, T.I. (2011) BDDCS applied to over 900 drugs. AAPS J 13(4) 519-547
Cade, D., He, X., 2010. Hydroxypropyl Methyl Cellulose Hard Capsules and Process of Manufacture US Patent 20100168410 A1.
El-Malah, Y., Nazzal, S., Bottom, C.B. (2007) Hard gelatin and hypromellose (HPMC) capsules: estimation of rupture time by real-time dissolution spectroscopy. Drug Dev. Ind. Pharm. 33, 27–34.
Esseku, F., Lesher, M., Bijlani, V., Lai, S., Cole, E., Adeyeye, M. (2010) The effect of overencapsulatrion on disintegration and dissolution. Pharm Technol 104-111
Cole, E.T., Scott, R.A., Connor, A.L., Wilding, I.R., Petereit, H.U., Schminke, C., Beckert, T., Cadé, D. 2002. Enteric coated HPMC capsules designed to achieve intestinal targeting. Int. J. Pharm. 1, 231, (1), 83-95.
Cole, E.T., Scott, R.A., Cade, D., Connor, A.L., Wilding, I.R., 2004. in-vitro and in-vivo pharmacoscintigraphic evaluation of ibuprofen hypromellose and gelatin capsules. Pharm Res. 21, (5), 793-8.
Cole E.T., Cadé, D., Benameur, H., 2008. Challenges and opportunities in the encapsulation of liquid and semi-solid formulations into capsules for oral administration. Adv. Drug Deliv. Rev. 17; 60, (6), 747-56.
Colton, A. (1931). Capsule machine U.S. Patent 1 787 777 and British Patent 360 427.
Deepthi, Y., Murthy, T.E., 2015. Design and development and evaluation of candesartan cilexetil liquid filling formulations. Int. J. Pharm. Investig. 5, (2), 81-6.
Digenis, G.A., Sandefer, E.P., Page, R.C., Doll, W.J., Gold, T.B., Darwazeh, N.B. 2000. Bioequivalence study of stressed and nonstressed hard gelatin capsules using amoxicillin as a drug marker and gamma scintigraphy to confirm time and GI location of in vivo capsule rupture. Pharm Res. 17, (5), 572-82.
Dressman, J. (1986). Comparison of Canine and Human Gastrointestinal Physiology. Pharmaceutical Research, 3(3), 123-131.
FDA Drug approval package (1998). Excedrin® Migraine (Acetaminophen, Aspirin & Caffeine) Tablets, Caplets & Geltabs. http://www.accessdata.fda.gov/drugsatfda_docs/nda/98/020802_s000_ExcedrinTOC.cfm
FDA Guidance for Industry Dissolution Testing of Immediate Release Solid Oral Dosage Forms http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm070237.pdf
Garbacza, G. Cadé, D., Benameur, H, Weitschies, W., 2014. Bio-relevant dissolution testing of hard capsules prepared from different shell materials using the dynamic open flow through test apparatus. European Journal of Pharmaceutical Sciences 57, 264–272.
Goadsby, P. J., Ferrari, M. D.,; Olesen, J., Stovner, L. J., Senard, J. M., Jackson, N. C., Poole , P. H. C. (2000) Eletriptan in acute migraine:: A double-blind, placebo-controlled comparison to sumatriptan. Neurology 54(1): 156 – 163
Groshens, E., He, X., Cade, D. (2009) Hypromellose Hard Capsules – Reproducibility of theIn Vitro Dissolution Performance in USP SGF Media. Poster AAPS Annual Meeting 2009
He, X., Groshens, E., Remondiere, I., Cade, D. (2012) Hypromellose capsules dissolution. Poster AAPS Annual Meeting 2012
Honkanen, O., Laaksonen, P., Marvola, J., Eerikäinen, S., Tuominen, R., Marvola, M., 2002. Bioavailability and in vitro oesophageal sticking tendency of hydroxypropyl methylcellulose capsule formulations and corresponding gelatin capsule formulations. Eur. J. Pharm. Sci. 15 (5):479-88.
Honkanen, O., Seppä, H., Eerikäinen, S., Tuominen, R., Marvola, M. (2001) Bioavailability of ibuprofen from orally and rectally administered hydroxypropyl methyl cellulose capsules compared to corresponding gelatin capsules. S.T.P. Pharm Sci 11(2): 181 - 185
Jones, B.E., Basit, A.W., Tuleu C., 2012. The disintegration behaviour of capsules in fed subjects: A comparison of hypromellose (carrageenan) capsules and standard gelatin capsules. International Journal of Pharmaceutics, 424 (1–2), 40–43.
Kilic, M., Jantratid, E.,, Cade, D.,, Benameur, H., Dressman, J.B. (2009) in-vitro dissolution performance of a new hypromellose capsules – Vcaps Plus in biorelevant media. Poster AAPS Annual Meeting 2009
Ku, M.S, Li, W., Dulin, W., Donahue, F., Cade, D., Benameur, H., Hutchison, K. 2010.
Performance qualification of a new hypromellose capsule: part I. Comparative evaluation of physical, mechanical and processability quality attributes of Vcaps Plus, Quali-V and gelatin capsules. Int. J. Pharm. 15, 386, (1-2), 30-41.
Ku, MS, Lu, Q., Li, W., Chen, Y. (2011) Performance qualification of a new hypromellose capsule: Part II. Disintegration and dissolution comparison between two types of hypromellose capsules. Int J Pharm 416: 16 - 24
Liebowitz, S.M., Vadino, W.A., Ambrosio, T.J., 1990. Determination of hard gelatin capsule brittleness using a motorized compression test stand. Drug Dev. Ind. Pharm. 16, 995–1010.
Lickliter, J. Noble, R., Smith D., Russ, S., Morris, S., Cooper, M. 2014. Pharmacokinetics and food effect of formulations of afuresertib. Clinical Pharmacology in Drug Development. 3, (S1), 8 1-14-1971589.
Ogura, T., Furuya, Y., Matuura, S., 1998. HPMC capsules: an alternative to gelatin. Pharm. Tech. Europe. 10 (11), 32-42.
Oullet, D, et al. Effects of Partricle Size, Food, and Capsule Shell Composition on the Otral Bioavailability of Dabrafenib, a BRAF inhibitor, in Patients with BRAF Mutation-Positive Tumors, J. Pharm Sci. 102(9) 2013
Sikes, C., Alderman, J., Emir, B., Wilding, I. (2003) Encapsulation of sumatriptan tablets does not alter their bioavailability or dissolution characteristics. Headache 43 : 581 – 582
Stegemann, S., Klebovich, I., Antal, I., Blume, H.H., Magyar, K., Németh, G., Paál, T.L., Stumptner, W., Thaler, G., Van de Putte, A., Shah, V.P. 2011. Improved therapeutic entities derived from known generics as an unexplored source of innovative drug products. Eur. J. Pharm. Sci. 20, 44, (4), 447-54.
USP 29<Acetaminophen, Aspirin and Caffeine Tablets>
Vardakou, M., Mercuri, A., Naylor, T.A., Rizzo, D., Butler, J.M., Connolly, P.C., Wickham, K.S.J., Faulks, R.M. (2011) Predicting the human in-vivo performance of different oral capsule shell types using a novel in-vitro dynamic gastric model. Int J Pharm 419: 192-199
Wilding, I.R., Clark, D., Wray, H., Alderman, J., Muirhead, N., Sikes, C.R. 2005. In vivo disintegration profiles of encapsulated and nonencapsulated sumatriptan: gamma scintigraphy in healthy volunteers. J Clin. Pharmacol. 45, (1), 101-5.