- Independent CMC Consultants
Introduction
Excipients are essential ingredients in medicinal products, facilitating manufacture, stability, absorption, administration and, in some cases, drug targeting. They can also, enhance aesthetic appearance, facilitate product differentiation and improve compliance. They are no longer generally considered to be pharmacologically inert.1 Indeed, antimicrobial preservatives by their very definition need to show antimicrobial activity to facilitate meaningful product shelf-lives. Their presence is specifically mandated for multidose semi-solid and liquid products.2,3 Additionally, these requirements also apply to devices for transdermal delivery where the delivery system is aqueous-based and enhanced by application of a mild electric current, i.e. electrophoretic. Performance standards for antimicrobial efficacy are defined within the various pharmacopoeias4,5,6 and involve challenging the formulation with a range of different microbial species, i.e. bacteria (three types), a yeast (Candida) and a mold (Aspergillus). Viruses are not included. Test organisms are common to all product types,4,5,6 but individual requirements can vary with product type.7,8,9 This diversity of microbial test organisms sets high standards for preservative performance. Furthermore, a number of traditional preservatives are no longer in current use due to concerns regarding their safety. The list of available preservatives may be further constrained by emerging concerns and associated regulatory constraints. No new preservatives have become available to replace those that are no longer sanctioned for use. This review is the first part of an updated7 three -part review and discusses such developments and offers perspectives on the management of such constraints.
Preservative Availability
Biocidal Agents
The ideal biocidal or preservative system meets the following requirements;
- antimicrobial activity against the microbes listed in pharmacopeial test methods, also possibly against product or facility-specific microbes that may pose a risk to product quality,
- antimicrobial activity spans the pH range associated with the product or device,e.g. iontophoretic system,
- free from irritancy, bitterness and other sensory effects at the inclusion level in the product,
- does not adversely interact with the drug, or other components in the formulation, package or delivery device,
- maintains preservative efficacy throughout products shelf life and in use period.
It can be difficult to meet all such requirements with a single agent. It is common practice therefore to use combinations of preservatives in order to meet the performance standards. The preservatives that are commonly used at this time are listed in Table 1, along with their Chemical Classes. Chemical structure can influence, not only their modes of action but also, physico-chemical properties and interaction propensity with other components in a product. Such possibilities need to be considered in dosage form design.
Table 1. Common Preservatives for Pharmaceutical Products

A number of medications that deliver drugs transdermally have become available in recent years. While these can be considered as “single-dose” products, the possibility exists that their (necessarily) prolonged contact with skin could lead to microbial growth in the area of application. Most are formulated in non-aqueous bases so they do not require preservation. In a few cases, however, drug delivery is driven by iontophoresis, and such systems are aqueous-based. To the authors’ knowledge there are no regulatory guidelines in place, nor any performance standards with respect to preservation. However, the above-mentioned precedents suggest that it is prudent to consider including a preservative when developing such a product. Historically, preservatives have been widely used in cosmetic and food products but much more limited number have been used in medicinal products, if monographs in the major pharmacopoeias (USP, Ph. Eur., JP) or in Product-related information in Regulatory Agency databases are any yardstick. The preservatives listed in Table 1 reflect the limited choices currently available to the pharmaceutical formulator, particularly when availability for specific product types or routes of administration is further constrained by the nature of the agents and the performance requirements listed in Table 2. Relevant microbiology textbooks provide more extensive background.2,3
Table 2. Performance Requirements for Preservatives
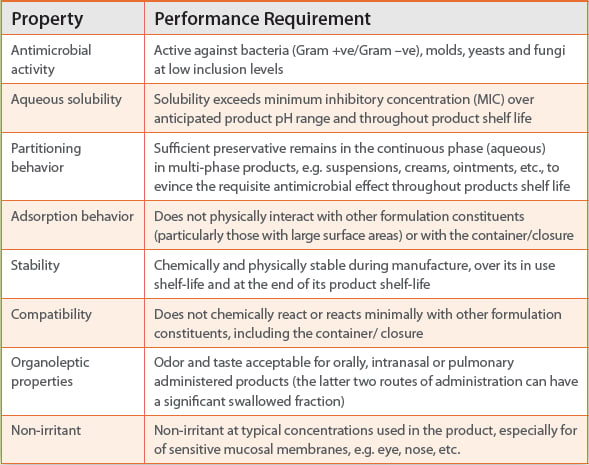
Furthermore, there are no preservatives available that possess sufficient efficacy, safety and non-irritancy to allow inclusion in products instilled into ocular or intrathecal tissue.3 Such products must be preservative-free. There is also mounting pressure to develop preservative free parenteral products, this being reflected in the increasing prevalence of single use presentations, e.g. blow fill seal (BFS) products. However, multi-dose parenteral products still require preservation.13 In addition, there is an increasingly negative view of some of the more commonly used preservatives, particularly in Europe, driven in large by a more conservative assessment of their intrinsic safety and labelling considerations.15 This has led to a concerted effort to replace supposedly “offending” preservatives particularly for pediatric, multi-dose oral products containing parabens”.16
Other biocidal agents, which are commonly used as preservatives, are still found in mature products.2 They include hexachlorophene, ethyl alcohol, sodium metabisulfite, sulfur dioxide, formaldehyde donators, e.g. imidurea, bronopol and the older quaternary ammonium compounds (QACs), such as cetrimide, cetalkonium chloride and cethexonium bromide. Benzalkonium chloride is still widely used in ocular and intra-nasal products, but its continued use is actively debated because of safety concerns in ocular17 or intra-nasal products.18,19,20
The phenols, although generally discouraged in oral and to a lesser extent in topical products based on toxicity considerations remain prominent in parenteral products, particularly biologicals.13 So do organo mercurials, although their use in vaccines remains controversial. The use of formaldehyde-donors e.g. imidurea and bronopol has decreased in topical and ophthalmic products due to concerns about formaldehyde sensitization. Hexachlorophene is an excellent disinfectant but its use as a preservative has declined because of concerns over neurotoxicity.11 Typically, the use of these older preservatives in new products has been largely discontinued because of safety considerations, with the notable exception of parenteral products, which is probably based on different risk-benefit considerations in multi-use sterile products.
Non-Biocidal Agents
Concentrated sucrose solutions can be effective preservatives in oral liquids because of their high osmotic pressure resulting in lowering of the water activity (Aw) of the formulation.21 However, sucrose has fallen from favor in liquid oral medications because of cariogenic concerns, illustrating the progressive attrition of preservation options. Polyols such as xylitol and sorbitol are more typically used and they can decrease Aw to values of about 0.8-0.9, in addition to having enhanced sweetening effects compared to sucrose. However, there are reports of such materials influencing (positively and negatively) the bioavailability of drug products, due to effects on osmotic flow and small intestinal transit times.22 Propylene glycol is often used as an adjunct to other preservatives because of its good solvent properties (superior to glycerin). There have been historical reports of adulteration with ethylene and diethylene glycols. The USP monograph for Propylene Glycol has limit tests for these toxic adulterants.23
Modes of Action of Preservatives
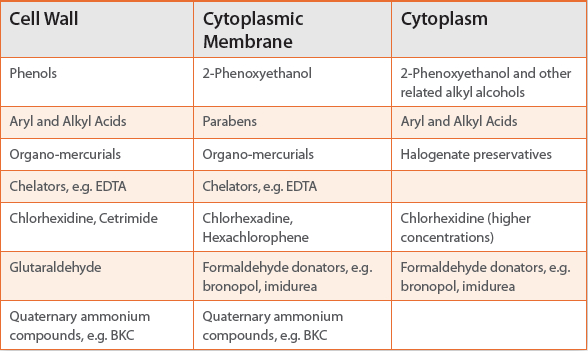
Preservatives generally show limited efficacy against viral organisms and compendial guides do not stipulate testing. Bactericides and fungicides target various microbial cellular sub-structures, for example; the cell wall, the cytoplasmic membrane or the cytoplasm. It is often difficult to assign a precise target for a specific class of preservative; the target can and does change with preservative concentration (Table 3). Consequently, preservatives may interfere with several different microbial cellular mechanisms, facilitating the use of synergistic combinations. However, the selection constraints that will be discussed in part 2 of this review, can present other barriers to use of combinations of preservatives.
Table 3. Site of Preservative Activity in Microbial Cell
A consequence of this broad-based cytoxicity strategy is that mammalian cells can also be affected. Consequently, inclusion levels should be minimized, consistent with adequate preservation. Achieving such a balance can be a major challenge. There is also a regulatory expectation that the reason for preservative inclusion, proof of efficacy, safety information, control methods in finished product and details of labeling in the finished product be addressed by the applicant in filings.24 Applicants may be challenged regarding the choice and concentration of preservatives, particularly in Europe and especially in pediatric dosage forms, where there is a preponderance of oral liquid products.
Mechanisms for biocidal activity at the cellular locations listed in Table 3 can also differ with each preservative. Antimicrobial cell wall activity may involve lysis due to enzyme inhibition, as is the case with phenols and organo mercurials. Alternatively, glutaraldehyde manifests its effect by irreversible cross-linking at the bacterial cell wall.2,3 Antibacterial cytoplasmic membrane activity may be attributed to effects on membrane potential, membrane enzymatic function or general membrane permeability.2,3 Cetrimide, chlorhexidine, hexachlorophene, 2-phenoxyethanol, parabens and phenols all affect membrane permeability, causing ‘leaking’ of essential cell constituents ultimately leading to cell death. Sorbic acid inhibits transport mechanisms across the bacterial cytoplasmic membrane and suppresses fumarate oxidation.3 Chlorhexidine also inhibits membrane ATPase, thereby inhibiting cellular anaerobic activity. At higher concentrations it induces precipitation of cytoplasmic nucleic acids and related proteins. Other biguanides induce phase separation and the formation of domains in the phospholipid bi-layer. Chelators such as edetic acid (EDTA) and the newer ethylenediamine-N,N’- disuccinic acid (EDDS) compromise the integrity of the cytoplasmic membrane by chelating Ca2+ and Mg2+, making these ions unavailable to the microbial cell and potentiating other anti-microbial agents, e.g. 4-chloroxylenol.25
Quaternary ammonium compounds bind strongly to the cytoplasmic membrane evoking general cytoplasmic membrane damage and subsequent leakage, but particularly targeting the phospholipid bi-layer. Cytoplasmic activity may result in uncoupling of oxidative and phosphorylation processes or interference with active transport mechanisms, as is the case with weak carboxylic acid and alcoholic preservatives.
Preservatives can also inhibit electron transport chains, thereby inhibiting metabolic activity in aerobic bacteria.26 Benzoic acid and the parabens inhibit folic acid synthesis.3 Organo-mercurials target thiol enzymes3 in the cytoplasm (as do silver compounds); whereas, formaldehyde donators e.g. imidurea, bronopol act on the carboxylic and amino enzymes in the cytoplasm. Phenols cause protein denaturation,27 as do the alcohols.3 Such activity, while aiding preservation can also adversely affect other quality attributes such as drug degradation or compromising excipent performance.
Preservatives may also be chosen based on antimicrobial capability for a particularly troublesome organism associated with a manufacturing site or process (as well as meeting compendial requirements). Eradication of these organisms (typically water based Pseudomonads and related species, e.g. Burkholderia cepacia) is the remit of GMP (good manufacturing practice) and the preservative system should not be used to address deficiencies in manufacturing processes. However, the resistance of certain opportunistic pathogens, e.g. Bacillus subtilis, Burkholderia cepacia to many common preservatives has re-focused attention on this problematical issue. As a consequence, many companies now include the latter microbe as an additional challenge organism in the antimicrobial efficacy test (AET) as a prudent risk mitigation strategy.28,29 However these additional organisms can be difficult to grow in classical pharmacopoeial media4,5,6 so may require bespoke testing methodology.
Choosing a Preservative
Conceptually, the preservative (or more commonly the preservation system) protects the multiuse product against microbial proliferation, particularly in oral pediatric products without compromising product performance or patient safety. In practice, this means that the preservative(s) must:
- exert a wide spectrum of antimicrobial activity at low inclusion levels, i.e. potent and efficacious,
- maintain antimicrobial activity throughout product manufacture, shelf life and usage, i.e. stable,
- not compromise the quality or performance of the active agent or other product component, pack or delivery system,
- not adversely affect patient safety or tolerance i.e. be safe
Risk Assessment
The numerous quality requirements (together with potentially conflicting requirements) mandate the importance of a structured risk assessment exercise before and during dosage form design. Typical microbiological risk assessments for non-sterile pharmaceutical preparations are included in all of the pharmacopeia.7,8,9 The process has also been described in various commentaries.30 In addition to understanding the likely microbial burden potentially associated with input materials, i.e. API, excipients, container/closure, or from the process, it is also important to take account of factors that can either potentiate or inactivate the preservative system. For instance, the optimal pH for product stability, solubility and microbial efficacy are rarely the same. This necessitates pragmatic decisions based on appropriate risk assessment tools.31 It may be necessary, for instance to use a preservative at product pHs that are not optimally effective and to increase the preservative concentration for effective antimicrobial efficacy. Potassium sorbate is optimally effective at its pKa (4.7), and it is claimed to have minimum antimicrobial efficacy at pH’s above 6;32 however it can be effective at pH values above 6.0, but at concentrations much higher than are typically used at lower pH’s, i.e. ≤ 0.2% w/v at pH’s 4-5, but ≥ 0.5% w/v at pH’s greater than 6.
Other excipients, or the active pharmaceutical ingredient (API) may enhance (or weaken) the efficacy of the preservative system by a variety of mechanisms. It may also be possible, at product design stage to formulate the product such that desired pH is aligned with optimal preservative efficacy. Many pediatric liquid formulations (particularly those containing antibacterial agents) are formulated so that pH is in the range of 4.5-5.5, a region where aryl and alkyl acids exhibit reasonably good antimicrobial efficacy at relatively low concentrations. Historically, the parabens were always utilized when the target pH of the formulation was between pH 6-8. However, recent regulatory concerns in the European Union,16 regarding parabens, and particularly butylparaben and propylparaben, are likely to restrict the capability for adequate preservation of products at neutral or higher pH’s. Such limitations or the presence of problematic organisms should be addressed as part of the preservative selection/product design process. A recent article29 on the assessment of the antimicrobial efficacy of two preserved eye drop formulations highlighted some of these key issues. Each was ‘preserved’ using the quarternary ammonium compound, BKC. The author29 described an anti-histamine eye drop product, where the preservative, i.e. BKC was present at 0.5%w/v, but there were no other potentiating excipients. In contrast, in an anti-inflammatory eye drop formulation, the preservative, i.e. BKC was present at a much lower level (0.1%w/v), but the formulation also contained additional preservatives, i.e. boric acid/borax, EDTA, and PVP. These two formulations were challenged using the five standard pharmacopeial organisms (see The Preservative Challenge Test (Antimicrobial Effectiveness Test)) and Burkholderia cepacia, a well-established objectionable organism. The AET data demonstrated an acceptable kill rate for all organisms, except Pseudomas aeruginosa in the anti-histamine formulation. Interestingly, despite BKC being present in this formulation at 5x the level of the other formulation it was ineffective at killing this pharmacopoeial challenge organism. As BKC is effective over a very broad pH range (4-10)33 it is very unlikely that differences in formulation pH, per se, will have impacted on its comparative efficacy. The likely reasons for preservation failure are twofold, (i) synergistic combinations of preservatives are often required before they are effective; as certain bacteria can be resistant to single preservative systems, e.g. BKC,34 and (ii) other excipients can potentiate the activity of preservatives by reducing the water activity of the formulation (e.g. PVP35, polyols,35 etc.) or by chelating key bacterial transport ions, e.g. EDTA.25
Assessments of the likely risks arising from objectionable organisms that may be process or facility-specific might also be part of the risk assessment and mitigation program. A decision can then be made to include those organisms in the preservative efficacy testing programs; with the caveat that the pharmacopeial methodology will not be optimized for this additional organism.
Discussion
It will be evident from the performance criteria outlined in Table 2, and the supplementary strictures on use of some agents that the current limited list of acceptable preservatives is likely to be further reduced in the future. Physicochemical and organoleptic properties also limit choice, as do possibilities for interactions with the active ingredient or excipients (particularly those with large surface areas) or the pack or delivery system. Longer chain alkyl preservatives such as propylparaben, will bind to some container/closure systems to a greater extent than less hydrophobic preservatives, e.g. methylparaben.36 Furthermore, aqueous solubility of the parabens decreases as chain length and hydrophobicity increases. For example, propylparaben has significantly decreased aqueous solubility compared to methylparaben, which can cause problems during the manufacture of the oral liquid product.37 Such properties and performance criteria could usefully be incorporated in the Quality Target Product Profile (QTPP) for the preservation system and can be addressed in the formulation design program.38 However, it is evident from such considerations that the different (and often conflicting) criteria ensures that the formulation, or re-formulation of a multi-use preserved formulation will be extremely challenging.
The Preservative Challenge Test (Antimicrobial Effectiveness Test)
Pharmacopoeial antimicrobial effectiveness tests (AET) or preservative efficacy tests (PET) involve challenging a product with a defined number of colony forming units (cfu) of a variety of test microorganisms (bacteria, yeasts and fungi), enumeration at time zero and then monitoring kill/survival rate at defined time intervals up to 28-days.39,40,41 Test organisms that are recommended by all of the pharmacopoeias include,
- Gram positive coccus, Staphylococcus aureus
- Gram negative rod, Pseudomonas aeruginosa.
- Fungi/mold, Aspergillus brasiliensis (formerly niger)
- Yeast, Candida albicans.
In addition, the USP38 and Ph. Eur.39 recommend the use of the Gram negative coliform, E. coli. As indicated earlier, the list may be supplemented by additional resistant organisms that may be associated with a particular process, facility or material, e.g. Burkholderia cepaceia an opportunistic pathogen often isolated in manufacturing environments, or Bacillis subtilis, a spore-forming bacteria. Zygosaccharomyces rouxii is also a useful test organism in formulations with high sugar (or polyol) content. Acceptance criteria for USP39 and JP41 are broadly similar with some differences between product type and presentation. All require satisfactory reduction for each challenge organism with no subsequent increase from the initial count after 14- and 28-days. It is widely recognized that the criteria of the Ph. Eur.39 are the more stringent and challenging to meet. The Ph. Eur. requires a specified reduction in bacterial count within the first 14-days with no subsequent increase from the initial count after 14- and 28-days. Scheler et al.42 assessed the antimicrobial efficacy of a variety of oral liquid formulation preserved using sorbic acid, alcoholic co-solvents, and at different pH’s. All preparations, even those without sorbic acid, met the criteria for oral products with aqueous bases according to USP and JP, which define no increase from the initial count at 14 and 28 days. However, the Ph.Eur. criteria of not less than 1 log reduction from the initial count at 14 days, were only met by preparations at pH 5 with not less than 0.15% sorbic acid.
AET tests form part of the preservative optimization studies. They also need to be performed at the end of product shelf-life to confirm adequate preservation over the total duration of the product’s use. Some regulatory authorities may also require confirmation that the product is adequately preserved during its in-use period, when it is being routinely opened, dispensed and closed and the potential for microbial contamination is at its highest. As part of process development activities, most companies will also challenge the preservative system at the extremes of pH, preservative concentration, etc.42,43
Rapid high-sensitivity test systems are being explored as possible replacements for the cumbersome, time-consuming and rather unreliable pharmacopoeial tests. Techniques include ATP bioluminescence, electrical impedance and chemiluminecence.44 These offer the potential for automation of testing, high throughput screening of formulations during development and (probably) greater test precision and reliability. Inevitably, much development, validation and corroboration would be required before adopting a replacement technique.
Meanwhile, some issues could be addressed to ensure a more pragmatic approach is taken with the current requirements. These could include:
Harmonized Compendial Monographs
There is no clear evidence that the USP performance criteria have led to poorly preserved products within the US.45 In the light of such experience and the great difficulty in getting some products to meet Ph.Eur requirements42 (with attendant cost and delays to product development), it would be beneficial for the Pharmacopeial Discussion Group (PDG) to consider AET harmonization initiatives.
Align Test Duration with Product Usage
Some oral liquid products are manufactured as solids that are constituted with water prior to use. Shelf life in the solution state is typically constrained by drug instability, as such, 7 or 10 day in-use periods are common. Performance criteria for preservatives in such products should reflect the in use period. Running the test for 30 days, when the product may fail the test for other reasons e.g. loss of preservative through hydrolysis or sublimation makes little scientific sense.
Preservative Free Formulations
Preservative-free cosmetics, medications and food/beverages are frequently promoted as safer products. These initiatives fuel demands that preservatives be omitted from medicinal products, particularly pediatric formulations. It is true that significant progress has been made in technologies for “microbiologically clean” manufacture and packaging, as well as in GMP such that gross microbial contamination can be minimized or avoided. At the same time, many materials that are used as excipients, are of biological provenance and cannot realistically be sold as sterile. Furthermore, their nature or physical properties ensure that they cannot readily be sterilized before or during incorporation into multiuse oral liquid products. Terminal sterilization may not be feasible for the same reasons. The presence of low levels of microbes cannot be obviated in such cases and, if the vehicle allows or encourages microbial growth (over the necessarily long shelf life that pharmaceutical products must possess) the inclusion of a preservative in the product is simply a prudent way to assure an important quality attribute and safeguard the patient.
In practical terms, removing preservatives from a medicinal product (even if technically feasible) would require a comprehensive re-think of quality systems throughout manufacture to provide a product that is essentially microbe-free (i.e. essentially sterile). Packs and delivery devices must also ensure that the quality built in during manufacture is maintained throughout the product’s shelf-life, in particular, during its in-use period. Such an approach might involve the following practices:
- Controls of microbial levels in product components (drug, excipients and especially water, container/closure) incorporating vendor certification, testing, validation of packaging and storage in appropriately clean areas.
- Product manufacture in a microbe-free environment, i.e. an aseptic process. In some cases it may be possible to reduce or eliminate contamination by procedures during or at end of manufacture, as is possible with some food and confectionary products. However, there is a general regulatory reluctance to use preservatives to address poor manufacturing practices, to reduce viable microbial population of a non-sterile product or to control the bio-burden prior to sterilization of a multi-dose sterile product.39,40,41 Such “post-manufacture sterilization” may deal with residual microbes but endotoxins remain and pose additional quality and safety problems.
- Product is packaged in units that maintain closure integrity during shelf life e.g. BFS ampoules. Single-use units e.g. BFS are the most frequently used preservative-free container/ closure systems, but are difficult to use, particularly for geriatric patients and are more costly.
Several preservation-free intranasal devices are available for commercialization,46 but there are relatively few multi-use preservativefree nasal commercial products. It should be stressed that even using a preservative free device, the manufacturer still needs to minimize microbial contamination during manufacture/storage; there is a need to protect the nozzle during the within-use period and preventing contamination through air-intake after device actuation.46 Strategies for preservative-free nasal devices include the use of mechanical seals, the use of embedded anti-microbial agents e.g. silver on the interior of the nozzle, filtering systems within the device to remove microbial contamination and the use of negative pressure containers to prevent ingress of micro-organisms post actuation. Some companies are developing a multi-use nasal device with self-sealing nozzle that could maintain sterility after repeated microbial challenge tests.46
There are also several novel ophthalmic container/closure systems that utilize either a 0.2 micron filter or a preservative (e.g. benzalkonium chloride) adsorbed onto a filter to maintain sterility during the in-use period, and several have been commercialized.47 The ABAK®(Laboratoires Théa, France) and COMOD®(Ursapharm, Germany) container-closure systems have been used for several different ophthalmic products, such as common beta-blockers e.g. timolol and carteolol.17
Technologies are generally available to assure such quality and controls measures. Many pharmaceutical products already utilize such approaches. The in-use period where patients use the product still remains the Achilles heel, when the closure needs to be broached or penetrated so that a dose can be withdrawn and more importantly where there is potential for microbial contamination. There is no universally reliable way that this can be achieved for each and every product type. Getting it wrong at any stage of the supply chain, manufacture, storage or in-use will almost certainly result in a return to earlier health concerns caused by microbial contamination of preservative free multi-use ‘sterile’ medicines.48
Conclusions
Preservatives, either singly or in synergistic combinations remain necessary to prevent microbial contamination of multi-use liquid or semi-solid medicinal products. Non-inclusion can result in serious patient health consequences. There are a limited number of regulatory-approved preservatives that can be included in these multi-use medicinal oral or topical products and the number is constrained even further in parenteral products. In the nearly 6 years since our first review, additional preservatives, e.g. parabens have fallen out of favor in Europe based on safety considerations, but they can still be used in the US. However, as industry typically develops multi-national products aimed at all of the major market, the strictest regulatory hurdles drive decision making. Thus it is very unlikely, that companies would develop multi-use products preserved with parabens for just the US market. Furthermore, it may be time to revisit the tests and performance requirements that products must undergo before being considered to be adequately preserved; although for exactly the reasons already outlined it is the Ph. Eur. anti-microbial efficacy test40 that drives decision making. Performance criteria and assessment techniques, based on product type, dose, environmental history in manufacture and experience during patient usage might be more appropriate than applying a single quality standard defined in pharmacopoeias that may well represent “overkill” in a microbiological and commonsense context for many products.
Preservative-free approaches are still in their infancy and much more research is required before they can be considered on an equal footing with preserved approaches. However, several preservativefree intranasal and ophthalmic devices are available and offer some promise. Finally, there is increasing regulatory expectation (particularly in the US) that additional challenge organisms, particularly the opportunistic pathogen, B. cepacia are used in the anti-microbial efficacy procedure; despite the fact that this procedure was never developed with this intent and this organism grows slowly in the standard pharmacopeial media.
References
- Moreton, C. (2010). Functionality and Performance of Excipients in a Quality-by-Design World, supplement to American Pharmaceutical Review, Volume 13(6): S2-S47.
- Fassihi, R.A. (1991). Preservation of Medicines against Microbial Contamination, in: S.A.Block (Ed.) Disinfection Sterilization and Preservation, 4th Edition, Lea and Febiger, pp. 871-886.
- Hugo, W.B., Russell, A.D. (Eds.), (1998). Pharmaceutical Microbiology, 6th Edition, Blackwell Science, pp. 201-262 and 365-373.
- European Pharmacopoeia (Ph.Eur 6.4), (2010). 2.6.13 (01/2009). Microbiological Examination of nonsterile products: Tests for specified microorganisms.
- Japanese Pharmacopeia (JP 15), (2008). 4.05. Microbiological Examination of nonsterile products: Tests for specified microorganisms
- United States Pharmacopeia (USP 38), (2015). <62> Microbiological Examination of nonsterile products: Tests for specified microorganisms.
- European Pharmacopoeia (Ph. Eur. 6.3), (2009). 5.1.4 (01/2009) Microbiological Quality of Non-Sterile Pharmaceutical Preparations and Substances for Pharmaceutical Use.
- Japanese Pharmacopoeia (JP 15), (2008). General Information 12. Microbial Attributes of Non-sterile Pharmaceutical Products as it appears in Supplement I to the Japanese Pharmacopoeia Fifteenth Edition (September 28, 2007, Notification PFSB No. 0928001). The English version was published on January 9, 2008.
- United States Pharmacopeia (USP 30), (2007). <1111> Microbiological Attributes of Nonsterile Pharmaceutical Products.
- Elder, D.P., Crowley, P. (2012). Antimicrobial Preservatives Part One: Choosing a Preservative System. Amer. Pharm. Rev. 13(6), S2-S47.
- Strickley, R.G., Iwata, Q., Wu, S., Dahl, T.C. (2007). Pediatric Drugs – A review of Commercially Available Oral Formulations, J.Pharm.Sci., 97: 1731-1774.
- Fransway, A.F. (1991). The Problem of Preservation in the 1990s: III Agents with Preservation Function Independent of Formaldehyde Release, Am. J. Cont. Derm., 2, 145- 174 (1991).
- Myer, B.K., Ni, A., Hu, B., Shi, L. (2007). Antimicrobial Preservative Use in Parenteral Products: Past and Present, J.Pharm.Sci., 96, 3155-3167.
- Penha, F.M., Rodrigues, E.B., Maia, M., Furlani, B.A., Regatieri, C., Melo, G.B., Magalhāes, O., Manzano, R., Farah, M.E. (2010). Retinal and Ocular Toxicity in Ocular Application of Drugs and Chemicals-Part III: Retinal Toxicity of Current and New Drugs, Ophthalmic Res., 44, 205-224.
- EMA (2017).Excipient labelling. http://www.ema.europa.eu/ema/index.jsp?curl=pages/ regulation/general/general_content_001683.jsp&mid=WC0b01ac05808c01f6. Accessed on 01 July 2017.
- EMA (2015). Reflection paper on the use of methyl- and propylparaben as excipients in human medicinal products for oral use. 22 October 2015 EMA/CHMP/SWP/272921/2012 Committee for Medicinal Products for Human Use (CHMP).
- Baudouin, C., Labbè, A., Liang, H., Brignole-Baudouin, F. (2010). ‘Preservatives in Eyedrops: The Good, The Bad, and The Ugly’ Progress in Retinol and Eye Research, 29: 312-334.
- EMA (2014). Questions and Answers on Benzalkonium chloride in the 5 context of the revision of the guideline on ‘Excipients in 6 the label and package leaflet of medicinal products for 7 human use’ (CPMP/463/00). 22 May 2014, EMA/495737/2013, Committee for Human Medicinal Products (CHMP).
- Bernstein, L. (2000). Is the use of benzalkonium chloride as a preservative for nasal formulations a safety concern? A cautionary note based on compromised mucociliary transport. J. Allergy Clin. Immunol., 105(1), 39-44.
- Marple, B., Roland, P., Benninger, M. (2004). Safety review of benzalkonium chloride used as apreservative in intranasal solutions: An overview of conflicting data and opinions. Otalaryngology- Head and Neck Surgery, 130(1), 131-141.
- United States Pharmacopeia (USP 38), (2015) <1112> Application of water activity determination to nonsterile pharmaceutical products.
- García-Arieta, A. (2014) Interactions between active pharmaceutical ingredients and excipients affecting bioavailability: Impact on bioequivalence, Eur. J. Pharm. Sci., 65, 89–97.
- United States Pharmacopeia (USP 38) (2015). Propylene Glycol monograph.
- EMA (2003). Draft Note for Guidance on Excipients, Antioxidants and Antimicrobial Preservatives in the Dossier for Application for Marketing Authorisation of a Medicinal Product, Committee for Proprietary Medicinal Products (CPMP), The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use, CPMP/ QWP/419/03, London 20th February 2003.
- Owen, S.C. (2006) Edetic Acid Monograph, in: R.C. Rowe, P.J. Sheskey, P. J. Weller (Eds.), Handbook of Pharmaceutical Excipients, Fifth Edition, Pharmaceutical Press, 2006, pp. 260-263.
- Zhao, J., Yang, Z., Wang, M., Lu, Y., Yang, Z. (2004) Electrochemical Evaluation of the Inhibitory Effects of Weak Acids on Zagosaccharomyces baili, J. Agric. Food Chem., 52, 7246-7250.
- Guest, R.T. (2006) Phenol Monograph, in: R.C. Rowe, P.J. Sheskey, P. J. Weller (Eds.), Handbook of Pharmaceutical Excipients, Fifth Edition, Pharmaceutical Press, 2006, pp. 514-516.
- T. Sutton, T. (2012). “Objectionable Organisms” - The Shifting Perspective. Amer Pharm Rev October, 1-10.
- Eisa, M. (2016). A novel approach in assessing the antimicrobial efficacy of eye drop products. Eur. Phar. Rev., 21(2), 40-43.
- Elder, D.P., Newby, P. (2016). Risk-Based Microbiological Testing, Eur. Pharm. Rev., 21(3), 36-40.
- ICH Q9 (2005) Quality Risk Management, Current Step 4, 09 November 2005.
- Owen, S.C. (2006) Potassium Sorbate Monograph, in: R.C. Rowe, P.J. Sheskey, P. J. Weller (Eds.), Handbook of Pharmaceutical Excipients, Fifth Edition, Pharmaceutical Press, 2006, pp. 609-610.
- Kibbe, A.H. (2006) Benzalkonium Chloride Monograph, in: R.C. Rowe, P.J. Sheskey, P. J. Weller (Eds.), Handbook of Pharmaceutical Excipients, Fifth Edition, Pharmaceutical Press, 2006, pp. 61-63.
- Sakagami, Y., Yokoyama, H., Nishimura, H.R., Ose, Y., Tashima, T. (1989). Mechanism of resistance to benzalkonium chloride by Pseudomonas aeruginosa. Appl. Environ. Micro., 55(8), 2036-2040.
- Luthra S., Obert J.P., Kalonia D.S., Pikal M.J. (2007). Impact of critical process and formulation parameters affecting in-process stability of lactate dehydrogenase during the secondary drying stage of lyophilization: a mini freeze dryer study. J. Pharm. Sci., 96, 2242-2250.
- Johnson, R., Steer, R. (2006). Propyl Paraben Monograph. Rowe, P.J. Sheskey, P. J. Weller (Eds.), Handbook of Pharmaceutical Excipients, Fifth Edition, Pharmaceutical Press, 2006, pp. 629-632.
- Guo, H., Knutsen, C. (2011). Preservative formulations and effectiveness in oral solutions and suspensions. PDA Metro Meeting, February 15 2011. https://www.pda.org/docs/ default-source/website-document-library/chapters/presentations/metro/preservativeformulation- and-effectiveness-in-oral-solutions-and-suspensions.pdf?sfvrsn=6. Accessed on 27 July 2017.
- ICH Q8(R2) (2009). Product Development. Current step 4, August 2009.
- United States Pharmacopeia (USP 34), (2010). <51> Antimicrobial Effectiveness Testing.
- European Pharmacopoeia (Ph. Eur. 6.4) (2010). 5.1.3 Efficacy of Antimicrobial Preservation.
- Japanese Pharmacopeia, (JP 19). Preservative Effectiveness Test.
- Scheler, S., Saupe, S., Herre, A., Fahr A. (2010). Preservation of liquid drug preparations for oral administration. J. Pharm. Sci., 99, 357-367.
- Nguyen, N-A.T., Wells, M., Cooper, D.C. (1995). Identification of Factors Affecting Preservative Efficacy and Chemical Stability of Lamivudine Oral Solution through Statistical Experimental Design. Drug Dev. Ind. Pharm., 21, 1671-1682.
- Newby, P.J. (2000). Rapid Methods for Enumeration and Identification in Microbiology in Handbook of Microbiological Quality Control, Editors R.M. Baird, N.A. Hodges, S.P. Denyer, Taylor and Francis, New York, London.
- Sutton, S.V.W., Porter, D. (2002). Development of the Antimicrobial Effectiveness Test as USP Chapter <51>. PDA Journal of Pharmaceutical Sciences and Technology, 56, 300-311.
- Brouet, G. (2003). Preservative-free Nasal Sprays: What Technology should be Selected and How Should it be Evaluated? Expert Opinion Biol. Ther., 3, 519-523.
- Furrer, P., Mayer, J.M., Gurny, R. (2002). Ocular Tolerance of Preservatives and Alternatives, Eur. J. Pharm. Biopharm., 53, 263-280.
- Kallings, L.O., Ringertz, O., Silverstolpe, L. (1996). Microbial contamination of medical preparations, Acta Pharm. Suecica, 3, 219-228.
Author Biographies
David P. Elder has 40-years of experience in the pharmaceutical industry. He was formerly a director in the pre-clinical group at GSK and is now an independent CMC consultant. He has a PhD from Edinburgh University, UK. He is a member of the British Pharmacopoeia Commission and an FRSC. He has written and lectured widely on the theme of product development and the challenges of preservation.
Patrick Crowley is a pharmacist by training (FRPhSGB). He worked in the Pharmaceutical Industry for over 40 years and was a VP of product development at GSK. He currently operates as a consultant and teaches Pharmaceutical Sciences at a number of Institutions. Has authored/ presented on over 40 topics related to pharmaceutical sciences.