The recent introduction of US Pharmacopoeia (USP) Chapter <1602>1 highlights the need to routinely test metered dose inhalers (MDIs) using methods that more closely reflect patient use scenarios. MDIs are the frontline defense for asthma and other common respiratory illnesses but require a level of co-ordination – between device actuation and inhalation – that some patients find difficult to achieve. The use of breath-actuated MDIs (BA-MDIs) addresses this issue, but these can be expensive to develop and difficult to retrofit to existing products. An alternative option is dry powder inhalers (DPIs) which typically rely solely on the inhalation maneuver of the patient to drive drug delivery. However, DPIs require a substantial inspiratory effort for successful drug delivery and neither of these devices operate with ‘natural’ tidal breathing. These limitations are significant, particularly for patient groups that struggle to follow instruction and/or to inhale with sufficient energy.
The use of spacers and valved holding chambers (VHCs) eliminates any requirement for co-ordination by providing a contained dead volume into which the dose is aerosolized, and from which the patient inhales the drug, by breathing tidally. Practical, inexpensive and easily retrofitted to existing MDIs, such add-on devices may be supplied with a mouthpiece or facemask, to further ease patient use, but in either case alter the characteristics of the delivered dose. USP Chapterdetails test methods that can be used to assess the extent of any change in the characteristics of the delivered dose and has implications for both innovator and generic product testing. In this article we consider the test methods described in the new chapter, focusing on the equipment available to assist with their application. A key aim is to provide understanding and practical guidance to support the effective testing of MDIs under all relevant scenarios.
MDI Testing
The standard methods for MDI testing were originally developed for QC and optimized in the first instance to detect difference, and for straightforward, standardized application. These quantify emitted dose (ED) – the total amount of active pharmaceutical ingredient(s) (API) in each aerosolized dose – and the aerodynamic particle size distribution (APSD) of the API within that dose, which directly influences in vivo deposition, but make no allowance for the use of add-on devices.
It has been recognized for some time that alternative test methods are required, for both ED and APSD measurement, with substantial experience gained in Canada following the publication of a Health Canada standard2 over a decade ago. Progress towards the methods outlined in the USP Chapter <1602> is also evident in a USP stimuli to revision document released in 20123
Identified goals are to quantify the impact of spacers and VHCs in a clinically relevant way by:
- Accurately simulating the added volume associated with the use of specific equipment – spacer or VHC, with a mouthpiece or facemask
- Quantifying the impact of a time delay between actuation and inhalation for VHCs – coordinated vs. uncoordinated use.
Typical instructions for MDI usage suggest that the patient should insert the device into the mouth and then inhale slowly and deeply, triggering actuation just after the start of the inhalation maneuver, by pressing the exposed end of the canister downwards, within the actuator. Under these circumstances the dose is aerosolized directly into the respiratory system, with dispersed particles immediately entrained on the incoming breath.
Spacers consist of an open ended tube (see Figure 1) with a mouthpiece or facemask at one end and an inhaler interface fitting at the other, while VHCs additionally incorporate a one-way valve, at the mouthpiece or facemask end of the chamber. This valve ensures that the dose is held in the chamber prior to inhalation and prevents evacuation of the chamber upon unintended exhalation. Both devices therefore introduce additional volume – dead volume – into the drug delivery set-up compared with MDI-only delivery, with VHCs additionally introducing the potential for inhalation to be coordinated with actuation – temporally synchronized – or uncoordinated, with a time delay of seconds between the two.
 Figure 1. Spacers (left) and VHCs (right) come in various designs, operating as illustrated in these generalised schematics.
Figure 1. Spacers (left) and VHCs (right) come in various designs, operating as illustrated in these generalised schematics.A key effect of including an add-on device is that “almost all of the mass fraction of drug associated with particles having ballistic trajectories”1 is retained within the spacer or VHC; in other words larger particles adhere to the interior walls of the add-on device as a result of inertial impaction. Beyond this, the additional volume introduced provides an opportunity for time dependent processes such as enhanced aerosol expansion and co-solvent evaporation, gravitational sedimentation and/or electrostatic deposition4 . These processes can shift the APSD of the delivered dose, as well as altering the total mass.
Investigating Changes In Delivered Dose: ED Measurement
For an MDI, delivered dose or ED is determined by actuating the device into a Dose Uniformity Sampling Apparatus (DUSA) which captures the dose on a filter. Subsequent analysis, usually by high pressure liquid chromatography (HPLC), reveals the amount of API present. The test flow rate applied is 28.3 L/min, a figure that reflects requirements for APSD measurement by cascade impaction, but with a DUSA it is far easier to apply tidal breathing patterns during the sampling process, as in nebulizer testing, since the constant flow rate limitations of a cascade impactor are no longer relevant (see later). The new chapter calls for the application of patient-relevant breathing profiles during all ED measurements, as defined in Table 1, which is easily achieved using an appropriately specified breath simulator.
Table 1. Representative tidal breathing patterns for pMDI with spacer/VHC testing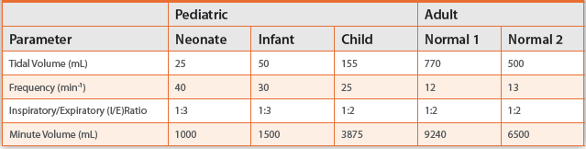
How is the effect of a facemask quantified via ED testing?
Where used, a facemask plays an active role in transporting API particles to the patient so assessing its impact on ED represents an important challenge. The new chapter specifies methods for the measurement of ED with a facemask in place thereby creating a requirement for a face model. A suitable face model set-up will:
- Have dimensional suitability for a defined patient age range
- Ensure a realistic dead space and the absence of leaks between mask and model when the facemask is applied with a clinically relevant force, typically 1.6 kg
- Simulate in vivo conditions by having physiologically accurate facial tissue in the areas where the facemask makes contact
- Provide a means of mounting the spacer/VHC such that the facemask is in correct alignment with the face, to simulate ‘real-life’ in-use conditions. The new chapter recognizes that models with ‘an anatomically accurate realization of the upper airways’ may be used, but equally allows for the use of a simpler model designed to simulate open mouth breathing with no accurate physical representation of the upper airway. A considerable amount of research (see box) has been carried out to develop face models for use within the laboratory and commercial solutions are becoming available to ease this aspect of testing (see Figure 2). Equipment such as this supports highly reproducible testing and can be substantially easier to use and validate than in-house designs.
 Figure 2. Typical system set-up for testing ED of MDIs with add-on devices utilizing a facemask (Facemask Testing Apparatus with child face model and Breath Simulator.
Figure 2. Typical system set-up for testing ED of MDIs with add-on devices utilizing a facemask (Facemask Testing Apparatus with child face model and Breath Simulator.How is the impact of uncoordinated use assessed in ED testing?
Because ED testing employs a tidal breathing pattern, uncoordinated use is assessed under the worst possible conditions, which is when actuation coincides with the onset of exhalation. In both coordinated and uncoordinated testing, sampling is continued for five breathing cycles, post actuation, to broadly simulate patient use of the product.
What metrics are recorded?
Measuring ED as outlined enables the generation of:
- ED with a facemask or mouthpiece (as relevant) under coordinated conditions for all add-on devices
- ED with a facemask or mouthpiece (as relevant) under uncoordinated conditions for VHCs only.
Where a facemask is part of the add-on device, performance with and without the facemask may also be directly compared to assess its impact simply by additional testing with the facemask removed. Comparing the coordinated and uncoordinated performance of VHCs directly assesses the efficiency of the one-way valve.
Investigating Changes In Delivered Particle Size: APSD Measurement
The APSD of MDIs is measured by cascade impaction at a test flow rate of 28.3 L/min (1SCFM) or 30 L/min in accordance with the methods specified in USP Chapter <601>10, with the Andersen Cascade Impactor (ACI) and the Next Generation Impactor (NGI) used for the majority of commercial testing. An underlying assumption with MDIs, as “active” devices is that the characteristics of the delivered dose are largely unaffected by the breathing maneuver of the patient, and the test flowrate specified is associated with the provenance of the instrumentation used, rather than having underlying clinical significance.
Cascade impaction size fractionates a dose on the basis of particle inertia, generating a series of samples that are subsequently analyzed, typically by HPLC, to produce an APSD specifically for the API11. A key feature of cascade impactors is that they must be operated at a constant flow rate. This raises the question of how best to simulate the tidal breathing pattern applied with an addon device, as with nebulizers. In fact, USP Chapter <1602> specifies an approach of exact parity with USP Chapter <601>for APSD measurement for products for adult use, with the Marple-Miller impactor highlighted as an appropriate alternative to the NGI and ACI. For non-adult patients – neonates, infants and small children – it is noted that testing at a lower flow rate may be more appropriate. The NGI is calibrated for use at 15 L/min and is therefore an appropriate choice for this application (an alternative is to use a Model 150P Marple-Miller impactor which operates at 4.9 or 12.0 L/min, though these are no longer in commercial production).
However, in this, and other aspects of testing, there is a judgment to be made regarding how far to move away from the simple, standard approach associated with QC testing, towards optimal clinical relevance, with researchers often finding that more sophisticated techniques than those specified bring value in R&D. For example, with a Mixing Inlet, which decouples the flow rate applied through a device during testing from that drawn into the cascade impactor (see Figure 3), it is possible to apply a low flow rate (in the case of paediatric relevant testing) or tidal breathing pattern (with a breath simulator) through the device, while maintaining a constant flow rate, at a calibrated value, through the impactor12. Such testing enables more representative investigation of the impact on APSD of an add-on device than can be accessed via constant flow rate analysis. The new chapter highlights the availability of such devices and their possible application.
 Figure 3. Accessories such as the child version of the Alberta Idealised Throat (shown on NGI, left) and Mixing Inlet with a Breath Simulator (right) can be used to make APSD testing more representative of clinical conditions.
Figure 3. Accessories such as the child version of the Alberta Idealised Throat (shown on NGI, left) and Mixing Inlet with a Breath Simulator (right) can be used to make APSD testing more representative of clinical conditions.Similarly, the specified test methods utilise the standard USP induction port, though the potential value of testing with more realistic throat models as exemplified by the Alberta Idealised Throat (Copley Scientific, Nottingham, UK) is also highlighted. The standard induction port is known to underestimate the amount of drug that deposits in the throat so using alternative induction ports can be a route to better in vitro in vivo relationships13.
Is the effect of a facemask quantified via APSD testing?
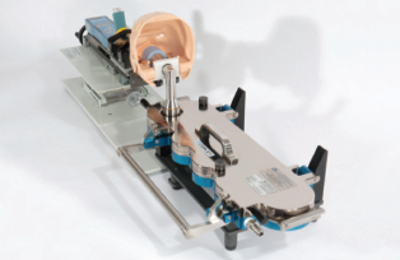 Figure 4. Commercial solutions are being developed to enable direct interfacing of a spacer/VHC with facemask to cascade impactors for APSD testing
Figure 4. Commercial solutions are being developed to enable direct interfacing of a spacer/VHC with facemask to cascade impactors for APSD testingAPSD measurements require interfacing of the spacer or VHC with an impactor. This is relatively straightforward for devices with a mouthpiece, but is more difficult with a facemask in place. The pharmacopoeial method suggests removal of the facemask to ease this aspect of testing and avoid the introduction of an ill-defined, unrepresentative connection. However, commercial products are now available that enable direct connection via a face model (see Figure 4). These provide a well-defined interface in terms of dead space representation, simultaneously easing connection of the add-on device and impactor, making it feasible to gain clinically relevant data with a facemask in place.
How are delay time-dependent APSD changes evaluated?
For VHCs, the ability to hold the aerosolized dose in the chamber prior to inhalation is reflected in the inclusion of test methods with impactor sampling starting two, five and ten seconds after actuation, as well as instantaneously-coordinated use. Two seconds is deemed to be representative of poor coordination and the bulk of deposition within the spacer occurs over this time period4,14. Testing after five and ten seconds provides further insight into how the characteristics of the dose and chamber retention can change over time in terms of parameters that are likely to impact in vivo lung deposition.
Meeting this requirement calls for equipment that can introduce a time delay between actuation of the device and impactor sampling. USP Chapter <1602> references a vertically moving shutter arrangement combined with microphone and timer. Alternatively, a timercontrolled fast-acting, two-way solenoid valve, see Figure 5, has been shown to provide a simple cost-effective solution and can be used to control both delay time and the total air volume drawn during testing, as specified14. This approach is closely aligned with pharmacopoeial DPI testing methods and is also suitable for testing BA-MDIs.
 Figure 5. A test set-up for measuring APSD of an MDI in the presence of an add-on device using the Breath Actuation Controller to control the time delay between actuation and cascade impactor sampling.
Figure 5. A test set-up for measuring APSD of an MDI in the presence of an add-on device using the Breath Actuation Controller to control the time delay between actuation and cascade impactor sampling.What metrics are recorded?
To compare drug delivery performance with and without an add-on device, determination of the following metrics is specified, typically for five spacers/VHCs:
- Mass of drug retained in spacer/VHC
- Mass of drug retained in induction port
- Stage-by-stage profile for the impactor sized mass i.e. the drug mass below the first stage of the cascade impactor used.
Other parameters may also be usefully recorded depending on the specific set-up. For VHCs, performance with and without a time delay should be directly compared and for all APSDs, a full mass balance is required, as with standard MDI measurements, to confirm the validity of the measured data.
Implications for Bioequivalence (BE) Testing
In recognition of the fact that the vast majority of MDIs will be used with an add-on device for a proportion of patients, it is usual for a manufacturer to identify a specific spacer or VHC for use with a new product. Indeed, regulatory guidance for Canada and Europe recommends this approach4. Testing to compare performance with and without the add-on device quantifies its impact, as outlined in USP Chapter<1602>, but what about BE testing for generic versions of the same product? Should this be carried out for the MDI alone, or for the MDI with the add-on device?
The purpose of BE testing is to establish that a generic product can be used interchangeably with the reference. Now that there are established methods for assessing the impact of an add-on device, the implication is therefore that BE testing should extend to comparative assessment of the MDI alone, and with the designated add-on device, suggesting two discrete BE studies. In the unlikely event that the add-on device specified with the generic is different from the reference product, a further comparison is also required4 . In summary, while the new chapter extends testing requirements for MDIs, it also brings clarity in terms of optimising in vitro testing for the demonstration of BE.
Conclusion
The introduction of USP Chapter <1602> marks a further step forward in the refinement of inhaled product testing to improve its relevance to clinical outcomes. While MDIs are used globally to enhance the daily lives of those with pulmonary diseases, it is often with the addition of a spacer or VHC which may significantly alter both the characteristics of the delivered dose, thereby impacting clinical efficacy.
USP Chapter <1602> provides details of all the test methods required, which can be used to compare MDI performance with and without an add-on device, for both new and generic products. Achieving a better understanding of how MDIs will work, in practice, for different patient groups, will make it easier to fully optimise their therapeutic efficiency.

References
- USP Chapter <1602> Spacers and Valved Holding Chambers Used with Inhalation Aerosols – Characterization Tests.
- CSA Group Standard, CAN/CSA-Z264.1-02 (R2011) ‘Spacers and Holding Chambers for Use with Metered-Dose Inhalers.’
- Mitchell, J.P. at el ‘In Vitro Assessment of Spacers and Valved Holding Chambers Used with Pressurized Metered-dose Inhalers: The Need for a USP Chapter with Clinically Relevant Test Methods’ USP Stimuli to the Revision Process 37(4) March 2012.
- Mitchell, J.P. and Dolovich, M.B ‘Clinically Relevant Test Methods to Establish In Vitro Equivalence for Spacers and Valved Holdings Chambers used with Pressurized Metered Dose Inhalers’. Journal of Aerosol Medicine and Pulmonary Drug Delivery, Vol 25, No 4, 2012
- Mitchell, J.P. ‘Appropriate Face Models for Evaluating Drug Delivery in the Laboratory: The Current Situation and Prospects for Future Advances’ Journal of Aerosol Medicine and Pulmonary Drug Delivery, Vol 21, No 1, 2008
- Morton, R.W and Mitchell, J.P. ‘Design of Facemasks for Delivery of Aerosol-Based Medication via Pressurized Metered Dose Inhaler with Valved Holding Chamber: Key Issues that Affect Performance.’ Journal of Aerosol Medicine Vol 20, Supplement 1, 2007
- Nagel, M. W. et al ‘Development and Evaluation of a Family of Human Face and Upper Airway Models for the Laboratory Testing of Orally Inhaled Products.’ AAPS PharmSci Tech (#2017) DOI: 10.1208/s12249-017-0802-5
- Xu, Z et al ‘Methodology for the ‘In Vitro’ Evaluation of the Delivery Efficiency from Valved Holding Chambers with Facemasks.’ Journal of Aerosol Medicine and Pulmonary Drug Delivery, Vol 27, 1, 2014
- Buchmann, M. A. et al ‘Performance Assessment of Valved Holding Chambers for Children with Budesonide pMDI’ Poster presented at ISAM Congress, Santa Fe, New Mexico, June 2017
- USP Chapter <601> Aerosols, Nasal Sprays, Metered-Dose Inhalers and Dry Powder Inhalers
- Copley, M. ‘Understanding cascade impaction and its importance for inhaler testing’ White paper available for download at: http://www.copleyscientific.com/documents/ww/ Understanding%20Cascade%20Impaction%20White%20Paper.pdf
- Copley, M ‘Refining inhaled product testing: a review’ White paper available for download at: http://www.copleyscientific.com/files/ww/news/COP%20JOB%20170_Refining%20 inhaled%20product%20testing%20-%20A%20Review%20%20111129.pdf
- Zhang, Y et al ‘In vivo- in vitro comparison of deposition in three mouth-throat models with Qvar® and Turbuhaler® inhalers’ Journal of Aerosol Medicine Vol 20(3) pp227 – 235, 2007
- Chambers, F. et al. ‘Evaluation of the Copley TPK-S as a Device for Control of Delay Times and Inspiration Volumes Applied to pMDI/Spacer Testing’. Poster presented at APS Inhalation, London, UK, February 2003.
Author Biography
Mark Copley graduated from the University of Bath, UK in 2000 with a Masters Degree in Aerospace Engineering. For 8 years he was Technical Sales Manager and product specialist for Copley Scientific’s range of inhaler testing equipment and is now Director for the company. Mark is considered a leading authority in testing methods and systems for metered-dose inhalers, dry powder inhalers, nebulisers and nasal sprays; authoring and contributing to more than 40 published articles. He also provides application support and consultancy, runs focused training workshops for the inhaled drug testing sector of the pharmaceutical industry and sits on the editorial advisory panel of Inhalation Magazine. An invited member of the European Pharmaceutical Aerosol Group (EPAG) impactor sub-team, Mark has also made recommendations to the Inhalanda working group, leading to subsequent revisions to Ph. Eur. and USP monographs.