Department of Archaeology, Anthropology and Forensic Science
Abstract
The development of non-destructive and rapid methods of authentication is critical in an era of expanding counterfeit and poor quality medicines production. This development is critical in cases such as antimalarial medicines’ that represent one of the main classes of medicines posing a threat to the public. Amongst the promising non-destructive techniques of identification, portable near-infrared spectroscopy stands out. This is attributed to its mobility and rapid analysis as well as its capability of analyzing both the chemical and physical properties of the sample. Therefore, the present work examines the feasibility of combining near-infrared spectroscopy with multivariate data analysis algorithms for the authentication of antimalarial medicines obtained from different countries. Medicines and their corresponding constituents were measured using a portable near-infrared spectrometer equipped with a near-infrared reflectance module. Tablets were measured as received from both sides and powders were measured through transparent glass vials. The spectra of powders were collected over the wavenumber range of 4000 – 400 cm-1 and exported to Matlab R2019a where multivariate classification algorithms were applied. The results showed that the medicines showed spectral features corresponding to their constituents (whether active pharmaceutical ingredient and excipient(s)) depending on the amount these constituents were present in the medicines. This was useful in case of undeclared excipients as is the case in some generics. Applying multivariate data analysis algorithms to the near-infrared spectra goes beyond confirming the presence/absence of the constituents into locating the manufacturing sources. However, this was not possible where constituents were present in low amounts within a medicine. In summary, the results demonstrated that portable near infrared spectroscopy was useful in locating manufacturing sources of generic antimalarials and identifying unknown constituents in medicines that are present in high amounts. However, where multiple constituents were present in low concentrations a more quantitative approach is needed.
Introduction
Malaria is a widespread infectious disease that contributes to 435,000 deaths globally.1 Despite its major prevalence in developing countries, it also affects developed countries. Thus, it has been anticipated that 3.4 billion people worldwide are at risk of having malaria.2 The wide spread of malaria stimulates the urgent need of antimalarial medicines that increases the chance of counterfeit spread alongside limited resources, lack of effective drug regulations, and gaps in the supply chain. Hence, counterfeit antimalarial medicines were frequently reported on several incidents.
According to the WHO (2006), 50% of antimalarial medicines in South East Asia were counterfeit.3 The situation did not change in 2018 when antimalarial medicines, alongside antibiotics, were still one of the most common counterfeited medicines.4 Moreover, the counterfeit and poor-quality antimalarial medicines contribute to thousands of preventable deaths each year.5 Subsequently, the use of counterfeit antimalarial medicines is of high risk to patients and danger to public health,6 and can result in drug-resistant parasites, severe diseases, or even death.
A counterfeit medicine may contain no active pharmaceutical ingredient (API), the wrong API, incorrect amount of the API, or the wrong excipients.4 The WHO estimates that 70% of counterfeit medicines do not contain any API and 16% contain the wrong ingredients.7 Therefore, when authenticating antimalarial medicines, it is important to characterize not only the API but also the excipients.
Detection of counterfeit antimalarial medicines has been reported in the literature using a diverse range of analytical techniques both classical and novel. Classical techniques for detection of counterfeit antimalarials included colorimetric reactions;8 high performance liquid chromatography9 and liquid chromatographymass spectrometry.10 More novel techniques reported were Fourier transform infrared,11,12 near-infrared (NIR)13 and Raman spectroscopy.14 The aforementioned spectroscopic techniques are portable in nature and thus off er less time-consuming procedures than classical techniques. Raman was used alongside other techniques to authenticate antimalarials and antibiotics from South East Asia.9 Surface enhanced Raman spectroscopy (SERS) was deployed for detection of APIs in chloroquine and primaquine tablets.14,15 However, the aforementioned studies only identified the APIs in tablets and did not characterize other additives. Moreover, SERS was destructive in nature and that affected the integrity of the tablets. In this sense, NIRS was the ideal technique as it could characterize rapidly the physicochemical properties of tablets non-destructively. NIRS has been deployed for authentication of artesunate tablets obtained from South East Asia.13 However, it did not take into account authenticating additional antimalarial medicine classes.
Subscribe to our e-Newsletters
Stay up to date with the latest news, articles, and events. Plus, get special offers
from American Pharmaceutical Review – all delivered right to your inbox! Sign up now!
The present study utilized portable NIRS in order to investigate the quality of antimalarial medicines manufactured in different sources including both developed and developing countries. The study further explored the potential for portable NIRS to fingerprint the evaluated medicines and to track manufacturing sources of the medicines purchased from the Internet.
Experimental
Materials
A total of eleven antimalarial medicines were used in this study including: Atovaquone/proguanil (n = 2), chloroquine (n = 4), mefloquine (n = 3), and quinine (n = 3) (Table 1). One reference medicine (from the UK) was used for each API. The medicines were obtained from five countries including Cyprus, India, Saudi Arabia, Sweden, and the UK. Moreover, constituents of medicines (APIs and excipients) were purchased from chemical suppliers.
Instrumentation
NIR spectra were recorded using a portable NIR spectrometer equipped with near-infrared reflectance module (NIRM). Spectra were collected over the wavenumber range of 10,000 – 4000 cm-1. Tablets were measured from both sides by placing them directly onto the NIRM. Powders were measured through transparent glass vials that were placed on the NIRM. Two spectra were collected from each tablet and three from each powder such that each spectrum was the sum of 32 scans.
Data analysis
NIR spectra were exported into Matlab 2019a where multiplicative scatter correction-second derivative (MSC-D1) was applied to all raw spectra. Multivariate classification algorithms were then applied to the MSC-D1 treated spectra. The aforementioned algorithms were correlated in wavenumber space (CWS) and principal component analysis (PCA) algorithms. For CWS, correlation coefficient (r) value of 0.95 was considered as a match. Furthermore, PCA was used unsupervised where clusters among medicines and constituents in medicines were compared.
Results and Discussion
The antimalarial medicines evaluated comprised a diverse sample set due to the different manufacturing sources, purchase sources, and number/types of excipients present. They comprised twelve medicines of four APIs, and sourced from three countries and/or the Internet. The purchase countries were Saudi Arabia, Sri Lanka and the UK. Moreover, the websites where medicines were purchased were UK-based websites. The manufacturing sources of the medicines varied and included Cyprus, India, Saudi Arabia, Switzerland, and the UK. The APIs corresponding to the aforementioned medicines comprised atovaquone/proguanil (as hydrochloride), chloroquine (as phosphate), mefl oquine (as hydrochloride), and quinine (as sulfate). All APIs were present in high percentage mass per mass (% m/m) in the range of (20 – 60% m/m). The remaining eight medicines had a number of excipients in the range of two to nineteen excipients. The most common excipients present in the aforementioned formulations were lactose, maize starch, MCC and talc. Four medicines did not have any of their excipients reported (Table 1). As the number and types of excipients were not always reported, a challenge in authentication was introduced. It is noteworthy to mention here another challenge in authentication attributed to the low sample size of the medicines compared, and this is often encountered in real life scenarios. Therefore, the choice of the multivariate data analysis algorithm for spectral interpretation should consider the (1) diversity of excipients, (2) undeclared excipients, and (3) number of medicines used to test each algorithm.
Spectral interpretation of reference medicines and their constituents
Authenticating the aforementioned medicines comprised inspecting any differences relating to their physicochemical properties. The choice of portable NIRS for product authentication was ideal due to many reasons. It provided detailed spectral information regarding the physicochemical properties of the products without the need for extensive sample preparation. Moreover, spectra collected could be analyzed using both the inbuilt software and exported offline for further analysis.15,16 Despite being a portable instrument, the spectral information obtained from the antimalarial medicines and their corresponding constituents was numerous over the wavenumber range of 10,000 – 4000 cm-1 (Figure 1).
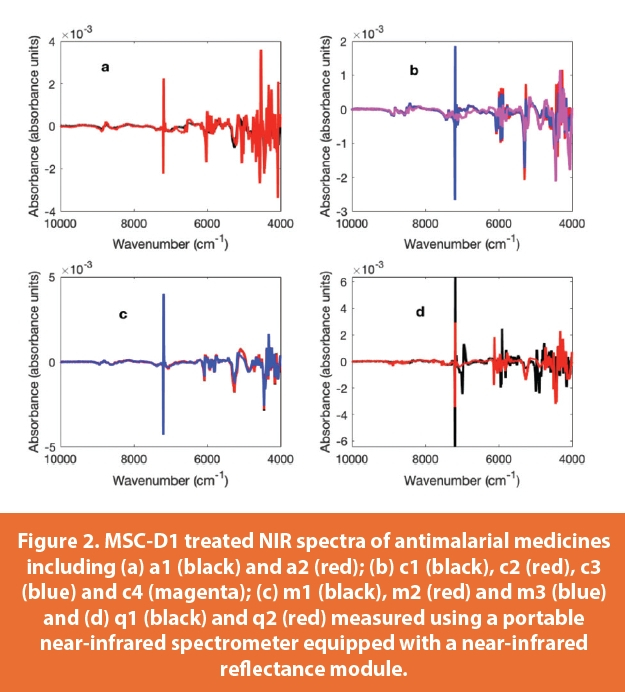
The absorbance intensities of the UK reference medicines and constituents were in the range of 0.001 – 0.005 absorbance units, with the exception of atovaquone and talc that showed stronger absorbances of 0.01 and 0.02 absorbance units respectively. Talc showed two distinctive peaks at 7182 and 7194 cm-1 that was beneficial for authentication especially when excipients were not declared. Hence talc peaks were distinctive and were prominent in M1 and Q1 that showed 21 and fifteen peaks respectively (i.e. strong absorbing). The number of peaks for the remaining medicines’ constituents and/or medicines was in the range of nineteen (for maize starch) – 33 (for chloroquine) (Figures 1 and 2). The latter findings were useful for spectral evaluation of medicines where spectral features of the constituent(s) were seen in the following medicines c1 and m1 (Figure 1). Hence, C1 showed spectral features corresponding to chloroquine. When the r values were compared C1 showed an r value of 0.8 against chloroquine that was present in a high concentration within the tablet (56.8% m/m) (Figure 3). It is noteworthy to mention that C1 showed an r value of 0.33 against maize starch despite its being a main excipient in the tablet. On the contrary, M1 showed r values of 0.72 and 0.59 against maize starch and mefloquine respectively. The remaining two medicines (A1 and Q1) showed low r values against their constituents that were below 0.7. In this respect, A1 showed maximum r value of 0.62 against MCC and Q1 showed a maximum r value of 0.44 against talc.

Test medicines comparison
The r values of the test medicines were compared against the reference medicines and their main constituents (Figure 3). Only one medicine was evaluated for each of atovaquone/proguanil (A2) and quinine (Q2) (Figure 2). In both cases, low r values were observed against reference medicines and were 0.76 and 0.61, respectively. Those results indicated that A2 and Q2 did not have common excipients as their corresponding reference medicines (A1 and Q1). It is noteworthy to mention that the excipients were not reported for A2 or Q2; yet, the presence of the peaks at 7182 and 7194 cm-1 indicated that talc was an excipient in both A2 and Q2.
The results were different for medicines containing chloroquine and mefloquine (Figure 3) that showed matches against their reference medicines. For chloroquine, C2 gave r value of 0.99 against C1 and that confirmed that both products were identical in terms of the physicochemical make up. C3 did not yield a high match against C1 (r = 0.84); but showed that peaks at 7182 and 7194 cm-1 that corresponded to talc though it had a low r value of 0.38 against talc. C4 gave low r value against C1 (0.46) and a maximum r value of 0.71 against MCC that could be a potential excipient within the tablet. Equally for mefloquine medicines, M2 gave an identical match against M1 (r = 0.99) that signposted identical physicochemical properties. M1 gave r value of 0.88 against m1 but showed that peaks at 7182 and 7194 cm-1 corresponding to talc, that indicated the presence of this excipient. Hence, CWS was ideal when the medicines obtained were manufactured by the same manufacturer and had identical physicochemical properties. However, where generics are obtained from different sources, other approaches are favored.
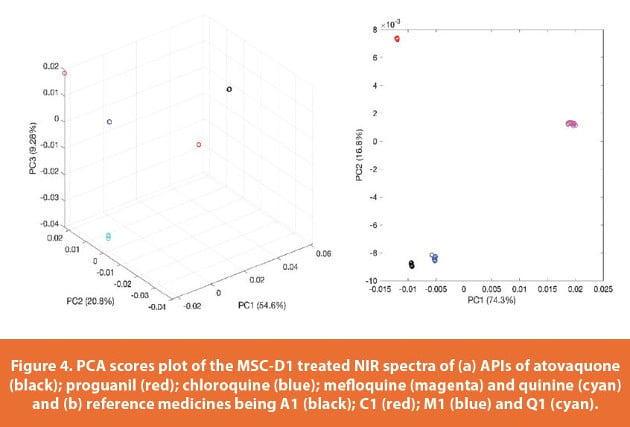
Therefore, PCA was used unsupervised on both APIs and reference medicines (Figure 4). The PC scores of the five APIs contributed to 84.7% of the variance among the data, and showed five distinct clusters corresponding to each of atovaquone, proguanil, chloroquine, mefloquine and quinine. Moreover, the PC scores of the medicines contributed to 91.1% of the variance among the data and showed four distinct clusters corresponding to A1, C1, M1 and Q1 (Figure 4). The findings assured the accuracy of the PCA model for the classification of medicines.

In this sense, PCA was applied unsupervised to the MSCD1 spectra of the medicines corresponding to each API(s): atovaquone/proguanil, chloroquine, mefloquine, and quinine (Figure 5). The PC scores of all four models showed high variance among the data (minimum 94.1%). The PC scores of atovaquone/proguanil contributed to 96.05% variance among the data and showed two distinct clusters corresponding to A1 and A2. Similarly, quinine PC scores contributed to 98.9% of the variance among the data and showed two separate clusters relating to Q1 and Q2. Chloroquine model PC scores contributed to 98.1% of the variance among the data and showed three distinct clusters: cluster 1 (C1 and C2), cluster 2 (C3), and cluster 3 (C4). Correspondingly, mefloquine PC scores contributed to 94.1% of the variance among the data and showed two distinct clusters: cluster 1 (M1 and M2) and cluster 2 (M3). Henceforth, PCA could be used to classify medicines according to manufacturers because the scores of medicines of the same physicochemical properties (i.e. C1 and C2, and M1, and M2) overlapped.

Conclusion
Portable NIRS offered a rapid and efficient technique for investigating antimalarial medicines of different sources and manufacturers. Spectral features of certain excipients (e.g. talc) were key in tracing its presence in medicines especially where the list of excipients had not been declared. CWS was useful in characterising generic antimalarial medicines but only when an identical reference medicine was available. PCA could be utilized to trace differences in physicochemical properties and cluster medicines according to manufacturing sources. Nonetheless, neither CWS nor PCA could indicate whether the generic medicine evaluated is authentic or counterfeit. Therefore, for authenticationof generic medicines a more quantitative approach is needed.
References
- World Health Organization, World Malaria Report, 2018a. Accessed August 2019. https://apps.who.int/iris/bitstream/handle/10665/275867/9789241565653-eng.pdf?ua=1
- Karunamoorthi K, Sabesan S, Jegajeevanram K, Vijayalakshmi J: The role of traditional anti-malarial plants in the battle against global malaria burden. Vector Borne Zoonotic Dis. 2013, 13: 521-544. 10.1089/vbz.2011.0946. doi:10.1089/vbz.2011.0946
- World Health Organization, Fact Sheet 275, Revised November 2006, Accessed August 2019. Accessed: https://www.who.int/en/news-room/fact-sheets/detail/substandardand-falsified-medical-products
- World Health Health Organization, Substandard and falsifi ed medical products, Revised 31 January 2018b. Accessed August 2019. https://www.who.int/en/news-room/fact-sheets/detail/substandard-and-falsified-medical-products
- Karunamoorthi, K. (2014). The counterfeit anti-malarial is a crime against humanity: a systematic review of the scientifi c evidence. Malaria journal, 13(1), 209.
- Nayyar G, Bremen JG, Newton PN, Herrington J. Poor-quality antimalarial drugs in southeast Asia and sub-Saharan Africa. Lancet Infect Dis. 2012; 12: 488-496
- WHO: The quality of Antimalarials: A Study in Seven African Countries. 2003, Geneva, Switzerland: World Health Organization, Available at http://whqlibdoc.who.int/hq/2003/WHO_EDM_PAR_2003.4.pdf. Accessed on 10th June 2013
- M.D. Green, D.L. Mount, R.A. Wirtz, Trop. Med. Int. Health 6 (2001)980–982.
- Yong, Y. L. Collaborative Health and Enforcement Operations on the Quality of Antimalarials and Antibiotics in Southeast Asia. Am. J. Trop. Med. Hyg., 92(Suppl 6), 2015, pp. 105–112. doi:10.4269/ajtmh.14-0574
- K.A. Hall, P.N. Newton, M.D. Green, M. de Veij, P. Vandenabeele, D. Pizzanelli,M. Mayxay, A. Dondorp, N.J. White, F.M. Fernández, Am. J. Trop. Med. Hyg. 75(2006) 804–811
- C. Ricci, L. Nyadong, F. Fernandez, P. Newton, S. Kazarian, Anal. Bioanal. Chem.387 (2007) 551–559
- C.C. Ricci, C. Eliasson, N. Macleod, P. Newton, P. Matousek, S. Kazarian, Anal.Bioanal. Chem. 389 (2007) 1525–1532.
- Dowell, F. E., Maghirang, E. B., Fernandez, F. M., Newton, P. N., & Green, M. D. (2008). Detecting counterfeit antimalarial tablets by near-infrared spectroscopy. Journal of pharmaceutical and biomedical analysis, 48(3), 1011-1014.
- M. de Veij, P. Vandenabeele, K.A. Hall, F.M. Fernandez, M.D. Green, N.J.White, A.M. Dondorp, P.N. Newton, L.L. Moens, J. Raman Spectrosc. 38 (2007)181–187
- Tackman, E. C., Trujillo, M. J., Lockwood, T. L. E., Merga, G., Lieberman, M., & Camden, J. P. (2018). Identification of substandard and falsified antimalarial pharmaceuticals chloroquine, doxycycline, and primaquine using surface-enhanced Raman scattering. Analytical Methods, 10(38), 4718-4722
- S. Assi, R. Watt, A. Moffat, Assay of ciprofloxacin in intact and powdered tablets by near infrared spectroscopy. Journal of Pharmacy and Pharmacology. (2008).
- S. Assi, R. Watt, A. Moffat. Identification of counterfeit medicines from the Internet and the World market using near-infrared spectroscopy. Analytical Methods. (2011) 3(10):2231-6.
Acknowledgement
The authors would like to thank Annalene Salter, Adam Naughton, Thomas Coombs and Tiffany Cullern for their contribution to the spectral collection of raw materials.
Author Biographies
Dr. Sulaf Assi is a senior lecturer in analytical chemistry at Liverpool John Moores University. Her research expertise is in pharmaceutical analysis, drugs analysis, counterfeit medicines, drugs of abuse, spectroscopy and multivariate data analysis. Dr Assi’s uses spectroscopic techniques for analysis of medicinal and lifestyle products.
Dr. Basel Arafat is a Senior Lecturer/Course Leader of the Pharmaceutical Sciences BSc (Hons.) course at the faculty of health, education, medicine and social Care (FHEMS), Anglia Ruskin University, UK. Basel is a multidisciplinary pharmaceutical scientist whose research focuses on applying advances in material science and drug carriers in the pharmaceutical field. His research also strongly focuses on bridging the gap between invitro and invivo research.
Kieran Evans is an applications scientist at PerkinElmer specializing in the utilization of materials characterization methods (FT-IR/NIR, UV/Vis and Fluorescence spectroscopy) in pharmaceutical, polymer and fuel analysis. Kieran obtained a master’s degree in chemistry from the University of Surrey and has coauthored several application notes pertaining to the novel use of material characterization techniques.
Ian Robertson has been working in the field of spectroscopy applications for over 35 years, working extensively on providing spectroscopic solutions for the pharmaceutical industry. He became a Graduate of the Royal Society of Chemistry in the 1980s achieving MRSC and CChem status. He is currently a Senior Applications Scientist in the Spectroscopy group at PerkinElmer, based in Seer Green in the UK.