Introduction
During the COVID-19 pandemic, the delivery of healthcare and the supply chains for critical reagents and supplies needed for the manufacturing both of established and novel therapies have been disrupted. Some critical materials may be unavailable as they could be used to produce COVID-19 related drugs or vaccines. Personal Protective Equipment (PPE), disinfectant wipes, and related materials used in clean room manufacturing facilities are likely to be in short supply for many months, if not longer. For advanced therapies, many critical materials used in the production and testing of cell, gene, and tissue therapies are obtained from sole suppliers. Some materials are unique, and some may be obtained from backup suppliers, though not all manufacturers may have pre-qualified all critical materials from backup suppliers. Further, sole suppliers or back up suppliers may be running at reduced capacity due to staffing shortages, or their own raw material supply chain disruptions. Air cargo service has dropped from pre-pandemic levels (15% as of 11 May 2020,1 26% as of 5 June 2020)2 due to the significant drop in the number of people traveling by plane (96% reduction as of 9 April 2020).3 Passenger airlines, which also carry air cargo along with passengers, were responsible for approximately 45% of air cargo capacity prior to the pandemic, and often COVID-19 countermeasures have been prioritized.1
If all materials needed for the manufacture of advanced therapies were available, the production and testing is still likely to be affected in areas where stay at home orders are in effect or may be placed in to effect following local outbreaks. And even when stay at home orders are lifted, it is certain that the availability of operators will be affected due to 1) distancing restrictions in laboratories and manufacturing facilities, 2) conversion to shifts with reduced staffing to minimize close working conditions, and 3) the possibility of COVID-19 resurgence and operator or support staff infections or quarantines. With these multi-factorial impacts on advanced therapies manufacturing, it is of heightened interest to assess various scenarios for the impact on patient access to clinical trials and to commercial products. From this information, mitigation strategies may be prioritized, and applicable to COVID-19 and future pandemics and other global disruptions of supply chains.
Methods
Using a computational simulation model, we previously developed,4 our goal was to investigate how the reduced availability in reagents (and materials), and operators could affect the supply chain of cell and gene therapy products, using Chimeric Antigen Receptor (CAR) T cells as an exemplar product. A first hypothesis to test is that there are lower bounds on reagent availability and operator availability that are needed to avoid adverse impacts on patients. A second hypothesis is that a priority queue (PQ) policy can alleviate the adverse impact of reagent or operator shortages.
At baseline, before supply chain disruptions our assumption of normal operations in a CAR T cell manufacturing facility is a first-come-first served policy (sometimes referred to a first-in-first-out, or FIFO, policy), where the order of the manufacturing requests are solely based on the request arrival time. Another policy for determining the order of manufacturing requests, which is akin to triage, is to assign the most seriously ill patients go to the front of the line, where the sickest patient requests are serviced FIFO and all other patient requests are also serviced FIFO. We refer to this policy as a priority policy (or priority queue, PQ) for ordering manufacturing requests, where in this case priority is determined on the basis of patient health status.
These two configurations were run through the simulation model to find the response surface, a method for mapping both the functional behavior of a system relative to parameter values and the variability of the behavior. In Experiment 1, given a current patient demand of CAR-T therapy, the model was queried to find the response surface of patient adverse outcome versus decreases in reagents and labor.
Subscribe to our e-Newsletters
Stay up to date with the latest news, articles, and events. Plus, get special offers
from American Pharmaceutical Review – all delivered right to your inbox! Sign up now!
Reduced operator availability may be due to illness, leave, staff spacing requirements, or partly as the result of PPE shortage, for example.
Only properly equipped personnel counts as ‘available operator’. We define the adverse outcome for patients as mortality due to disease or progression that cannot be salvaged through any available therapy. This ‘what if’ simulation study considered different durations (3 months, 6 months, and 9 months) of a pandemic. In Experiment 2, the priority queue policy was added and the same simulations as in Experiment 1 were run.
Results of Simulation Model Queries
For an autologous CAR T cell therapy, we assume therapy manufacturing can only begin if there is an initial collection of lymphocytes by leukapheresis from the patient (the raw material), an idle bioreactor, a sufficient amount of available reagent supply, and a sufficient number of available operators. We further assume that the number of bioreactors is large enough to ensure that for every patient leukapheresis collection, there will be an available idle bioreactor.
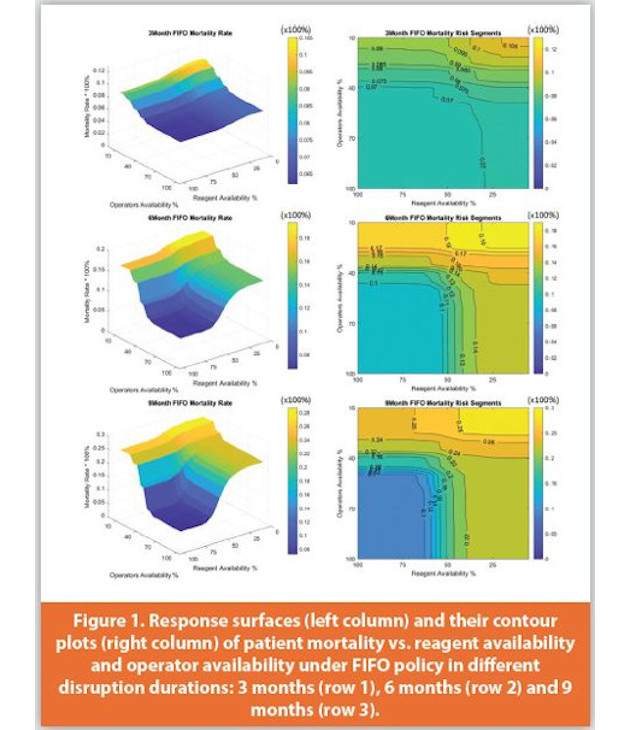
From the query, we observe that patient adverse outcome expresses an “s-curve” dependence for both reagent and operator availability. This dependence, most notably illustrated in the 6-month FIFO Adverse Outcome Rate graph in (Figure 1), implies that the adverse outcome rate stays relatively fl at as critical reagent availability percent decreases until a threshold is achieved. The first threshold, as marked by the contour line, reflects the point at which the gradient of the response surface starts to increase. Once reagent availability percent falls below this threshold, then there is a marked increase in adverse outcome rate until a second threshold is achieved, after which the adverse outcome rate flattens out again. This phenomenon also occurs as the operator availability percent decreases. For the 3-month, 6-month, and 9-month durations of the pandemic impact, from our simulation the first threshold levels at which the adverse impact will not escalate:

When these thresholds are less than 100%, this indicates a resilient system that can withstand significant drops in reagent and operator availability without significant impact on patient adverse outcome rate. This resilience is due to a significant amount of ‘cushion’ reagent availability and operator availability, each of which incurs cost. If these thresholds were closer to 100%, then the system would be considered ‘running leaner’ and would incur less cushion-related expenses. The lack of symmetry regarding adverse outcome rate should also be noted as operator availability percent and reagent availability percent decrease. This asymmetry is due to the fact that reagents can be stored in inventory whereas operators cannot. Although it is not assumed in these simulation runs that operators can be on-call, it is expected that such an assumption would tend to produce symmetries in adverse outcome rate as operator availability percent and reagent availability percent decrease. The magnitude of the asymmetry may also be addressed by cross training of staff in multiple laboratory functions to ensure greater cushion.
Implementing the priority queue (PQ) assignment scenario has only a modest impact on the value of the first threshold, compared to FIFO. However, once the reagent availability percent and/or the operator availability percent falls below this threshold, the increase in adverse outcome rate is considerably slower than the increase in adverse outcome rate for the FIFO case. Using the 9-month case as an example, the adverse outcome rate reaches 20% when operator availability percent equals 37.6% with FIFO, compared to 26.5% with PQ. The adverse outcome rate reduction due to PQ relative to FIFO is more significant when the operator availability percent is lower than the first threshold. The maximum reduction in adverse outcome rate due to PQ, relative to FIFO, for the 9-month case is more than 5%.
When both reagent availability percent and operator availability percent are above the first threshold, therapy manufacturing begins immediately for virtually all arriving leukapheresis collections for both classes of patients, whether the queuing discipline is FIFO or PQ, and hence there is little difference in the performance of these queuing disciplines. If operator availability percent is above the first threshold, then the FIFO and PQ systems perform similarly, for all values of the reagent availability percent. However, for any value of the reagent availability percent, the greater the decline in operator availability percent the better PQ performs, relative to FIFO, and hence operator availability is especially important under these conditions.
Summary of Main Findings
The findings from this simulation model confirmed that as postulated there are lower bounds on reagent availability and operator availability that are needed to avoid adverse impacts on patient access to treatments or experimental therapies during significant supply chain and operator availability disruptions. The exact numbers of personnel, bioreactors, and reagent stock levels depend on the facility configuration and treatment rates. Priority queuing has only a modest impact on the value of the lower bounds, compared to FIFO. However, once the reagent availability percentage and/or the operator availability percentage falls below this threshold, the increase in adverse outcome rate is considerably slower than the increase in adverse outcome rate for the FIFO case.
Discussion and Implications
Simulation models are useful to design options and contingency plans for advanced cell therapy manufacturing facility supply chain and personnel disruptions and to help maintain the lower bounds where patients are not adversely affected by treatment delays. While Priority Queuing has only a modest effect as examined in the scenarios modeled here, for some patients the ability to receive treatment may be life changing or lifesaving. Stringency of a priority queue may need to become greater when staff availability declines. Future interrogations using this simulation model can assess a dynamic priority queue, where the manufacturing order is determined by considering the request arrival time and the real-time patient health status. Disruption events may be of variable intensity as restrictions are implemented and lifted in a staged fashion. Additionally, the time dependency of availabilities can be modeled. The findings presented here also reinforce the contrast from manufacturing of shelf stable products or drugs and the manufacturing of on demand therapies.
Even before the COVID-19 pandemic, “just in time” inventory systems for advanced therapies in very ill patients was thought to be somewhat perilous. In addition to re-examining stocking and equipment levels, staffing, cross-training, and redesign of spaces to ensure adequate supplies and distance among staff are required contingency planning to ensure as many patients as possible may receive treatment during times of global supply chain and personnel availability disruptions.
References
- Max Finkel, The Coronavirus Is Shaking Air Cargo to Its Core, 11 May 2020, https://www.gizmodo.com.au/2020/05/the-coronavirus-is-shaking-air-cargo-to-its-core/
- Accenture report, ‘COVID-19: Effects on Air Cargo Capacity’, 5 June 2020 https://www.accenture.com/us-en/insights/travel/coronavirus-air-cargo-capacity