Abstract
Three human coronaviruses originating from zoonotic events are responsible for severe acute respiratory syndrome outbreaks around the world. The first two, SARS-CoV and MERS-CoV were disseminated by symptomatic individuals and controlled by rapid quarantine of people with illness, general use of personal protection equipment such as masks, rapid testing, and contact tracing. However, because of the asymptomatic transmission of SARS-CoV-2 and the different mutations related to virus attachment and entry to the host cell, transmissibility and infection rates were higher than SARS-CoV and MERS-CoV leading to the current pandemic of COVID-19. SARS-CoV-2 showed similar genomic organization related to other human coronaviruses with specific mutations in genes related to the spike glycoprotein and other accessory genes. Current mortality rates for SARS-CoV-2 are lower than those reported for SARS-CoV and MERS-CoV but the worldwide disruption has been more significant. Therapies such as vaccines and chemotherapeutic drugs are currently under development to either prevent infections or treat sick patients with agents that will inhibit viral entry, replication, or assembly.
Coronaviruses
A new virus isolated from an acute specimen obtained during an upper respiratory infection in a medical student at the University of Chicago has recently been described….is a ribonucleic acid (RNA) virus.
Dorothy Hamre and John J. Procknow
Coronaviruses (CoV) belong to the family of viruses Coronaviridae. Based upon genomic structure and phylogenetic analysis, coronaviruses are divided into four genera, Alphacoronavirus, Betacoronavirus, Gammacoronavirus, and Deltacoronavirus.1 Alpha and Betacoronavirues are primarily mammal pathogens while Gamma and Deltacoronaviruses infect birds.
Coronaviruses are enveloped viruses with a positive-sense singlestranded RNA genome surrounded by a nucleocapsid. The genome is one of the largest among the RNA viruses with a size ranging from 26 to 32 kilobases (kb). The order of structural genes such as capsid, spike, envelope and membrane proteins is highly conserved among genera while accessory genes seemed to be strain-specific.
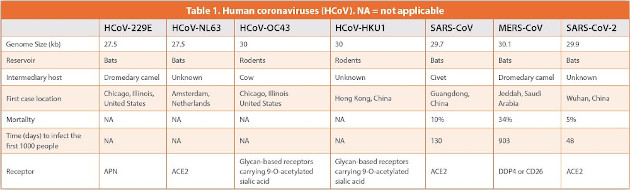
Prior to the first ever outbreaks of human coronaviruses (HCoVs) causing severe acute respiratory syndrome (SARS) in 2003 and 2012, HCoVs were known to be responsible mostly for upper respiratory illness. These viruses known as HCoV-229E and HCoV-NL63 belong to the Alphacoronavirus genus while HCoV-OC43 and HCoV-HKU1 are part of the Betacoronavirus. HCoV-229E and HCoV-NL63 were shown to have closer resemblance with bat coronaviruses while HCoV-OC43 and HCoV-HKU1 originated in rodents (Table 1). The genome sizes for HCoV-229E and HCoV-NL63 are approximately 27.5 kb while HCoVOC43 and HCoV-HKU1 have a genome size of 30 kb. HCoV-OC43 and HCoV-HKU1 use sugar-based receptors with sialic acid residues to enter host cells while HCoV-229E uses cell surface peptidases such as aminopeptidase N (APN) (Table 1). Because of the adaptive evolution and recombination events taking place in animal coronaviruses, two HCoVs were found to be associated with major SARS outbreaks.1,2 SARS-CoV was isolated in 2002 in Guangdong Province, China. A decade later another highly pathogenic HCoV, Middle East respiratory syndrome coronavirus (MERS)-CoV, was found to cause acute pneumonia and renal failure in Jeddah, Saudi Arabia. Humans were shown to be infected by intermediary hosts such as civets for SARSCoV and Dromedary camels for MERS-CoV (Table 1). Genetic analysis demonstrated several recombination events among bat, dromedary camel, and civet CoV leading to mutations in the spike glycoprotein (SP) used to enter host cells which allowed the development of new strains capable of infecting humans.1,2 When an animal CoV undergoes that type of change turning into a HCoV which subsequently infects humans then we have a zoonotic infection.2
Zoonotic diseases represent more than 60% of known human infections worldwide and continue to emerge in different continents around the world.2 This is due to changes in weather patterns, deforestation, improper practices in wet markets, population density, and environmental pollution.3 Sometimes our immune system does not have the ability to deal with some of these new microbial agents. Most of the time the agent is detected and destroyed but in some cases the microorganism mutates avoiding any immune response leading into a disorder of structure and or function in the human body, e.g., disease. There is an evolutionary race between the human immune system and microorganisms. Either the microbial agent wins the battle leading to morbidity or/and mortality or the immune system eliminates the microorganism from the body. Another possible scenario is the adaptation of the new microbial agent to the human body becoming completely harmless. For instance, several coronaviruses are extremely lethal in animals such as chickens, cats, or pigs but none of them evolved into a HCoV that will cause human infections. This might be because the animal immune system is very different with specific immune mechanisms that humans do not have. However, in some animals such as bats the immune system has evolved in such a way that bats can carry viruses without any harm due to immune mechanisms absent in other animals. For instance, bats have enhanced interferon-mediated immune responses and a strong modulation of inflammatory responses that are absent in other animals.4 As a response to these robust immune mechanisms, bat coronaviruses evolved rapid replication rates to maintain their viability and survivability. When these viruses cross over to other animals that do not have the same vigorous immune response to keep them under control, then we have diseases such as Ebola, rabies, SARS, MERS, and COVID-19.5
SARS-CoV-2
Bat-borne coronaviruses will cause more outbreaks. We must find them before they find us.
Shi Zhengli
A novel coronavirus, SARS-CoV-2, was identified as the etiological agent responsible for COVID-19 in Wuhan, China.5 The first case in the USA was reported in the state of Washington on January 19, 2020.6 The patient had returned from a family trip to Wuhan, China. The first person to person transmission in the USA was reported on January 30, 2020 in the state of Illinois.7 SARS-CoV-2 appeared to have strong structural and genetic similarities to SARS-CoV and other bat coronaviruses. SARS-CoV-2 like SARS-CoV and MERS-CoV belong to the genus Betacoronavirus. Although SARS-CoV-2 widespread transmission and infection seem to be much faster than SARS-CoV and MERS-CoV, mortality rates were lower (Table 1). However, MERSCoV appeared to be less transmissible than SARS-CoV.8 SARS-CoV was found to be transmitted by super-spreader events while MERSCoV depended on cluster outbreaks.8 However, SARS-CoV-2 has been widely disseminated by several super spreading events.10 For SARSCoV and MERS-CoV person to person transmission was documented to happen only when illness was apparent.5,8 On the other hand, SARSCoV-2 is widely disseminated by asymptomatic individuals.
The main cause of death in COVID-19 cases was Acute Respiratory Distress Syndrome (ARDS). ARDS is driven by a cytokine storm, which is a deadly inflammatory response due to the release of high numbers of pro-inflammatory molecules such as interleukin 6 (Il-6) in the infected area. This was very similar to cases with SARS-CoV and MERS-CoV.11 Unfortunately, the cytokine storm leads to a violent and relentless attack by the immune system against the body leading to ARDS and multiple organ failure.
SARS-CoV-2 Genome
We live in evolutionary competition with bacteria and viruses. There is no guarantee that we will be survivors.
Joshua Lederberg
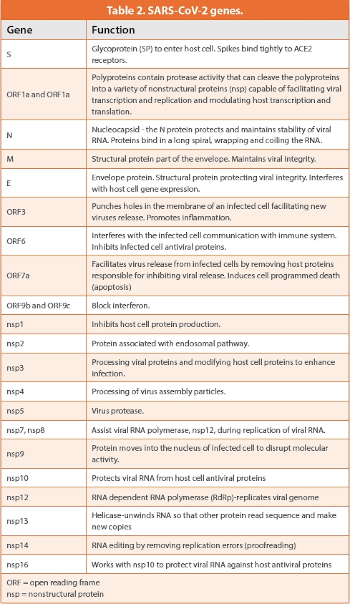
The genome of SARS-CoV-2 was found to be 29.9 kb which is bigger than SARS-CoV but smaller than MERS-CoV (Table 1). Based upon genomic sequencing, SARS-CoV-2 was very similar to SARS-Co-V but less related to MERS-CoV. However, closer relationships were found with other bat coronaviruses such as bat-SL-CoVZC45 and bat-SLCoVZXC21.8 The genome shows 14 open reading frames (ORF) coding for 27 proteins.9 Some of the known genes from SARS-CoV-2 are shown in Table 2. Structural proteins are coded by four different genes. These proteins are SP, envelope (E), membrane (M), and nucleocapsid (N) as well as several accessory proteins that participate in viral replication, infectivity and pathogenesis (Figure 1).
The SP facilitates receptor attachment by the virus and undergoes continuous mutations.11 Although genomic comparison studies showed high similarities to bat coronaviruses, the gene for SP was closer to SARS-CoV than any other coronavirus. Recent studies showed the SP of pangolin CoVs with an even closer genetic similarity to SARSCoV-2 even though genome relatedness was distant. The SP of SARSCoV- 2 comprises a S1 and S2 subunit which is structurally similar to SARS-CoV and MERS-CoV. The S1 subunit is for receptor binding while the S2 promotes cell membrane fusion. The gene coding for SP appeared to have some mutations that bind, like SARS-CoV and HCoVNL63, the human angiotensin converting enzyme-2 (ACE2) receptor.12 However, SP of SARS-CoV-2 showed more affinity and stability to ACE2 receptors than SARS-CoV. There is also a cleavage site at the junction of the S1 and S2 proteins which made enzymes such as proteases to be able to split the SP enhancing infectivity. This cleavage site is not found in any other bat or pangolin coronavirus. Entry to the host cells is enhanced by a host protease, transmembrane protease serine 2 (TMPRSS2). Upon entry, viral envelope fusion with cell membrane through the endosomal pathway leads to the releasing of viral RNA into the host cell.
Recent studies showed that the original D614 strain of SARS-CoV-2 which was spread from China to the world mutated into strain G614.13 This mutation took place in the viral SP by a substitution of the amino acid aspartic acid by glycine as a result of an A to G nucleotide mutation. Variation analysis in early March found that G614 was not widely distributed globally but was detected in Europe in higher frequencies. However, strain G614 has become the predominant pandemic strain of COVID-19. Strain G4 is related to higher viral loads and infectivity but so far it does not look more virulent than D614.
The E protein helps with virus assembly and release (Figure 1). It also enhances virus pathogenicity. The M protein is the most abundant protein that maintains viral assembly, integrity, and stability. The N protein is part of the nucleocapsid which binds to the viral RNA helping in the packaging and protection of the encapsulated viral genome.
Accessory or nonstructural proteins (nsp) are not part of the viral structure (Table 2). However, they help and enhance viral replication and pathogenicity by either replicating viral RNA (nsp7, nsp8, nsp12, nsp13, nsp13), suppressing human immune responses (nsp1, nsp3, nsp9, nsp10, nsp16), or providing support for viral assembly and release (nsp2, nsp4, nsp5). The largest nsp gene is for the replicase enzyme complex (ORF1a and ORF1b) leading to the production of two large proteins which are subsequently processed by several viral proteases. The major component of the enzyme system is responsible for viral replication and transcription. One of the enzymes in the system is the RNA-dependent RNA polymerase (RdRp) that catalyzes the synthesis of new viral RNA. The RdRp produces several species of molecules which are translated into viral proteins. These polymerases also make more copies of the RNA genome to be assembled into new virus particles. Viral proteins and genome RNA are assembled in the Endoplasmic Reticulum (ER) and Golgi Complex (GC). After assembly is completed, the virus particles are transported inside vesicles outside of the cell. SARS-CoV-2 seems to be reproduced in the upper respiratory system with subsequent migration and continuous reproduction in the lower respiratory system triggering atypical pneumonia leading into SARS. Recent studies showed high ACE2 concentration in the nose with decreasing numbers throughout the respiratory system.14 This might indicate that nasal surfaces are the dominant initial sites for SARS-CoV-2 respiratory tract infection with oral-lung aspiration as a key contributor to the virus migration to the lower respiratory system. Other accessory proteins such as ORF3 pokes holes in the infected cell membrane facilitating the release of new viral particles. It also promotes infl ammation. ORF9B and ORF9C block interferon production severely compromising the immune response to viral infections.
Detection of SARS-CoV-2 by Reverse Transcriptase Polymerase Chain Reaction
These results demonstrate that there is a new polymerase inside the virions of RNA tumor viruses…. The polymerase seems to catalyze the incorporation of deoxyribonucleoside triphosphates into DNA from an RNA template.
Howard M. Temin and Satoshi Mizutani
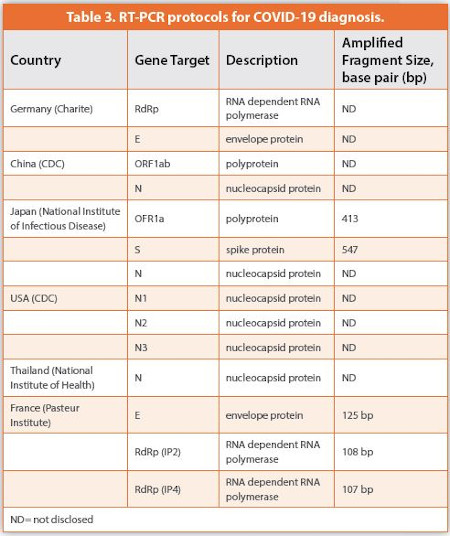
Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) is the gold standard for COVID-19 diagnosis. The purpose of the RT-PCR test is to identify part of the virus genome in the patient’s sample. Nasopharyngeal (NP), oropharyngeal (OP) or saliva samples are commonly analyzed for the presence of SARS-CoV-2.15 After extraction from patient’s samples, RT-PCR will be completed by targeting two or three genes on the SARS-CoV-2 genome. Several RT-PCR protocols have been developed by laboratories around the world (Table 3). Some protocols target the RdRp, SP, N, E, or ORF1a-ORF1b genes. The RT-PCR reaction will start with the reverse transcriptase enzyme (RTE) copying the targeted sequences from RNA to DNA. Short single stranded pieces of DNA called primers recognize unique RNA sequences along the viral genome. Two different primers are used during the reaction. The first primer binds to the viral RNA sequence then RTE makes a single stranded DNA copy called complementary DNA (cDNA). After the RNA is removed, the second primer binds to the other side of the cDNA. A second enzyme called Taq Polymerase (TP) extends the second strand to make a double stranded DNA of the target region. The DNA copy of the viral RNA gene undergoes several amplification cycles by TP to produce large quantities of viral DNA. The numbers of copies double with each cycle. A fluorescent probe is added to the reaction to quantify the concentration of DNA. The amount of fluorescence produced by the probe will be proportional to the concentration of DNA in the sample. The threshold cycle (CT) value is the number of replicating cycles needed to produce a fluorescence signal above the background fluorescence. Negative samples are always run to eliminate the possibility of false positives. The smaller the CT value the higher the concentration of viral DNA. CT values below 40 cycles indicated a positive result for SARS-CoV-2.14 Samples in a nursing facility located in the state of Washington, USA, were analyzed by RTPCR.16 CT values were reported for two genes coding for nucleocapsid proteins 1 and 2 (N1, N2). Of the 89 residents, 57 tested positive. CT values for N1 ranged from 13.7 to 37.9. More than half of the patients with positive tests were asymptomatic at the time of the testing.
Epidemiology of COVID-19
Gentlemen, it is the microbes who will have the last word.
Louis Pasteur
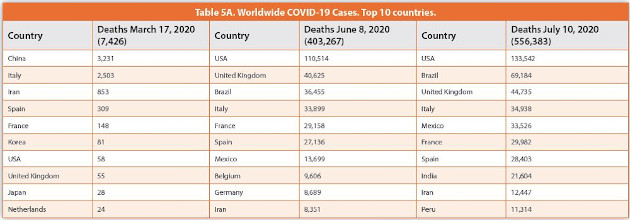
The world health organization (WHO) reported on March 17, 2020 approximately 179,122 cases of COVID-19 with 7,426 deaths.17 Most of the reported cases and deaths were in China followed by Italy and Iran (Tables 4A and 5A). The number of cases in the United States of America (USA) were reported to be 3,503 with 58 fatalities.
Mortality cases were associated to age, people older than 60, and different types of preexisting conditions related to diabetes, cardiovascular conditions, kidney problems, immunocompromised individuals, hypertension, etc. The incubation period was estimated to be 1-14 days with the numbers of infections doubling every 3-7 days. Mortality cases were significantly higher for male patients.
However, on June 8, 2020, the numbers of cases worldwide increased to 7,038,942 with 403,267 deaths (https://coronavirus.jhu.edu/map.html) (Tables 4A and 5A). COVID-19 cases in the USA increased to an astonishing 1,942,363 followed by Brazil from 234 to 691,758 cases. USA also showed the biggest increase in deaths (110,456) followed by the United Kingdom (40,570).
On July 10, 2020, COVID-19 cases worldwide increased to 12,342,043 with 556,383 deaths. USA accounted for 26% of COVID-19 cases and 24% of deaths worldwide. The USA again showed an increase of 1,198,575 cases followed by Brazil (1,064,021). However, Brazil (32,729) showed higher mortality increases than USA (23,028).
Subscribe to our e-Newsletters
Stay up to date with the latest news, articles, and events. Plus, get special offers
from American Pharmaceutical Review – all delivered right to your inbox! Sign up now!

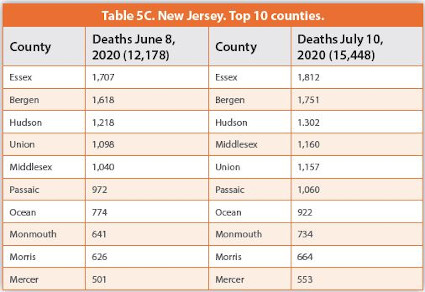
Regarding the USA, on June 8, 2020 the top 5 states with COVID-19 cases were New York, New Jersey, California, Illinois, and Massachusetts (Table 4B) (https://www.cnn.com/interactive/2020/health/coronavirus-usmaps-and-cases/). New York and New Jersey, respectively, showed the highest numbers of deaths (Table 5B). Major changes were observed on July 10, 2020 when the top 5 states were New York, California, Florida, Texas, and New Jersey. The highest growth in COVID-19 cases were reported in the states of Florida (180,207), California (171,997), and Texas (161,133). Although the state of New York reported the highest number of deaths, New Jersey showed the highest increase in mortality (3,270). The state of New Jersey is to the west and southwest of NY city. Hundreds of thousands of people commute daily to the city for jobs, education, businesses, entertainment, etc. Proximity to the COVID-19 epicenter in the USA led to the second highest numbers of morbidities and mortalities (Tables 4B and 5B). However, by July 10, 2020, the states of California, Florida, and Texas reported more cases than New Jersey. Looking at the numbers reported for the counties in the state of New Jersey, on June 8, 2020, Hudson showed the most cases followed by Bergen, Essex, Passaic, and Middlesex (https://www.nj.gov/health/cd/topics/covid2019_dashboard.shtml)(Table 4C). Mortality cases in Essex county were higher than in any other county, followed by Bergen, Hudson, Union, Middlesex (Table 5C). When it came to demographics, 50.3% of the infected individuals in New Jersey were females and 49.1% males. When cases were analyzed by ethnicity, 35.3% were white, 30.4% Hispanics, 17.2% African Americans, 11.8% other, and 5.1% Asian Americans. Mortality rates were 53.3% white, 19.4% Hispanics, 18.5% African Americans, 5.4% Asian Americans and 3.4% other. Fifty two percent of patients with COVID-19 were over 50 years old while 94% of the patients that died were older than 50. The top two preexisting conditions leading to high mortality rates were cardiovascular disease (57.3%) and diabetes mellitus (44.4%). However, on July 10, 2020 the county of Bergen showed the highest increase in COVID-19 cases (1,315) while the county of Ocean reported a higher increase in the numbers of death compared to any other county (148).
Vaccine Development
I have to do something about finding the right virus and the right virus was right in my house.
Maurice Hilleman
To provide protection and avoid COVID-19 infections, vaccines will be an important development to mitigate and terminate the pandemic. The number one target for vaccine development against SARS-CoV-2 is the SP protein. It provides several regions, and epitopes, that can elicit a strong immune response. The ultimate goal is to trigger the production of enough neutralizing antibodies that are stable and long lasting.18
There are different strategies that are currently under investigation to develop a vaccine for COVID-19. A dead virus containing SP can be injected into the human body to trigger an immune response. Attenuated virus particles with SP can also be used in a vaccine. The SP which has been isolated and purified is another possible alternative for effective vaccination. A pure preparation of SP can be delivered to develop immune protection. In some situations, a vector such as an Adenovirus can be genetically engineered to deliver the SP into the human body. Nucleic acid, DNA or RNA, vaccines with the genetic information to make SP can be translated in the host cell to produce antibodies against it.
Antiviral Drugs
For seven years of misfortune I had one moment of good luck.
Paul Ehrlich
In addition to vaccines, chemotherapeutic agents can be developed to treat people who have been diagnosed with COVID-19. Targeting some of the viral proteins can provide protection against SARS-CoV-2. Entry and fusion inhibitors block the SP binding to ACE2 and inhibit the fusion of the virus envelope with the host cell membrane. Studies have shown that by inhibiting the TMPRSS2 protease viral fusion was completely eliminated.18
The development of drugs to inhibit viral replication is very important because these enzymes are not part of the host cell. Therefore, they can be targeted without affecting the host metabolism. For instance, SARSCoV-2 viral replication is inhibited by using RdRp inhibitors.19 These drugs called nucleotide analogs inhibit the RdRp by RNA chain termination. Other possible drugs interfere with the assembly of new virus particles and subsequent release. Since SARS-CoV-2 used the ACE2 receptor, developing decoy receptors might eliminate the virus from the body due to the fact that these decoy molecules are in the body without any host cell. Therefore, when SARS-CoV-2 binds to the decoy there is no replication and infection. The decoy receptor bound to the virus can then be eliminated by the immune system.
The use of convalescent plasma (CP) from patients that recovered from COVID-19 has been shown to reduce some of the symptoms of COVID-19.18 Patient’s recovery appeared to be faster when CP was given during critical and chronic stages of the disease. CP contains antibodies (abs) mixtures (polyclonal) binding to more than one epitope of the virus structures. However, this can amplify the immune response to SARS-CoV-2. In this situation because they are different abs, they are less affected by changes in the chemical composition of the viral structures. Nevertheless, cross reactivity and batch variability will be a challenge to standardize operations.

Different monoclonal antibodies (mAbs) were developed targeting the spike proteins of SARS-CoV and MERS-CoV.18 mAbs are antibodies made by the same immune cells that are clones of a unique parental cell. mAbs have monovalent affinity to bind the specific part of the SARS-CoV-2 structure. For instance, they can bind the SP or N protein or both. They provide highly specific recognition of the viral structure targeted for destruction. They can be produced in high quantities by immortal cell lines during biopharmaceutical manufacturing. However, because of the high specificity any epitope changes will lead to a reduction in the binding capacity of the mAbs. In some situations, the combination of different mAbs will result in more efficient virus elimination.
Critical cases of COVID-19 are driven by an overreaction of the immune system led by elevated levels of inflammatory molecules in the lungs such as interleukin-6, e.g., cytokine storms. Inhibition of the receptor for Il-6 reduces the severity of the abnormal immune response. There are also several clinical trials where steroids were shown to control the abnormal immune response reducing the severity of the disease and decreasing mortality rates.
References
- Chen, Y. et al. 2020. Emerging coronaviruses: Genome structure, replication, and pathogenesis. Journal of Medical Virology 92:418-423.
- Cui, J. et al. 2018. Origin and evolution of pathogenic coronaviruses. Nature Review Microbiology 17:181-192.
- Taylor, L.H. et al. 2001. Risk factors for human disease emergence. Philos Trans R Soc Lond B Biol Sci. 29:983-989.
- Brook, C.E. et al. 2020. Accelerated viral dynamics in bat cell lines, with implications for zoonotic emergence. eLife 2020;9:e48401. DOI: https://doi.org/10.7554/eLife.48401.
- Rabaan, A.A. et al. 2020. SARS-CoV-2, SARS-CoV, and MERS-CoV: A comparative overview. Le Infezioni in Medicina 2:174-184.
- Holshue, M.L. et al. 2020. First case of 2019 novel coronavirus in the United States. New England Journal of Medicine 382:929-936.
- Ghinai, I. et al. 2020. First known person-to-person transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in the USA. Lancet 395: 1137-1144.
- Wong, G. et al. 2015. MERS, SARS, and Ebola: The role of super-spreaders in infectious disease. Cell Host & Microbes 18:398-401.
- Krogan et al. 2020. A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature 583:459-468.
- Frieden, T. R. and Lee, C. T. 2020. Identifying and interrupting superspreading events—Implications for control of severe acute respiratory syndrome Coronavirus 2. Emerging Infectious Diseases, 26:1059-1066. https://dx.doi.org/10.3201/eid2606.200495.
- He, J. et al. 2020. Molecular mechanism of evolution and human infection with SARSCoV-2. Viruses 12, 428; doi:10.3390/v12040428.
- Lu, R. et al. 2020. Genomic characterization and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet. 395:565–574.
- Korber, B. et al. 2020. Tracking changes in SARS-CoV-2 Spike: Evidence that D614G increases infectivity of the COVID-19 virus. Cell https://doi.org/10.1016/j.cell.2020.06.043
- Hou, Y.J. et al. 2020. SARS-CoV-2 reverse genetics reveals a variable infection gradient in the respiratory tract. Cell 182:1-18.
- Yan, Y. et al. 2020. Laboratory testing of SARS-CoV, MERS-CoV, and SARS-CoV-2 (2019-nCoV): Current status, challenges, and countermeasures. Review of Medical Virology 30:e2106.
- Arons, M.M. et al. 2020. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. New England Journal of Medicine 382: 2081-2090.
- World Health Organization. 2020. Coronavirus disease 2019 (COVID-19) Situation Report–57, 10 AM CET 17 March.
- Khan, S., et al. 2020. Emergence of a novel coronavirus, severe acute respiratory syndrome coronavirus 2: Biology and therapeutic options. Journal of Clinical Microbiology 58: e00187-20. https://doi.org/10.1128/JCM.00187-20.
- Yin, W. et al. 2020. Structural basis for inhibition of the RNA-dependent RNA polymerase from SARS-CoV-2 by remdesivir. Science 368:1499-1504.