Keywords
Pyrogens, Fever, endotoxin, Non-endotoxin Pyrogen (NEP), Monocyte, Pharmacopeia, Bacterial Endotoxin Test (BET), Monocyte activation test (MAT), synergisms
Abstract
At the beginning of the 20th century the first commercially available infusion/injection solutions were administered to patients. Pyrogenic side effects termed “Injection fever” or “water fever” (associated to the diluent) were described occasionally. As a consequence the Rabbit Pyrogen Test (RPT) was implemented into the British pharmacopeia (1912), the United States Pharmacopeia followed in 1942. Since then both the predictive RPT and improved pharmaceutical manufacturing contributed to the safety level achieved today. Frequently the (nonspecific) RPT has been replaced by the (specific) Bacterial endotoxin test (BET). New in-vitro alternatives to the RPT as the Monocyte Activation Test (MAT) combine the advantages of the RPT (assessment of pyrogenicity beyond gram-negative endotoxin) with the benefits of an in-vitro method (non-animal, high-throughput, easy to modify). Several drugs (including modern vaccines containing detoxified endotoxin as adjuvant) will benefit from these new options. The replacement of animal experiments by validated alternatives is statutory according to European law.
Introduction
In a worst-case scenario pyrogenic contaminations in parenterals (mainly i.v.) induce a fatal systemic response of the patient’s innate immune system. Symptoms range from fever to septic shock like symptoms. The RPT is a true pyrogen test, after intravenous application of the drug into three rabbits the body temperature is recorded for 180 minutes. The drug complies if the sum of the temperature increase (…fever) is within defined temperature ranges. The different setups from EP, USP and JP obviously generate the same level of safety.1 By its design it’s a qualitative (pass/fail) safety test for typically non-pyrogenic drugs.2 Products with intrinsic pyrogenicity do not fit into the current RPT design, recently this problem occurred with modern vaccine formulations containing Outer Membrane Vesicles (OMV)3 or modified endotoxins.4 For many products the RPT was replaced by the Bacterial endotoxin Test (BET; Limulus Amebocyte Lysate Assay (LAL)) after successful validation. The BET is specific for endotoxin (Lipopolysaccharide, LPS), the main constituent of the outer cell wall of gram-negative bacteria. LPS is the best known pyrogen, and due to its chemical robustness and outstanding biological activity a highly relevant threat for drug and patient safety. The BET is much more sensitive for endotoxin than the RPT, and is typically performed as a quantitative assay with a wide dynamic range (kinetic versions). The endotoxin content enumerated allows both a safety estimation (for the given drug batch) as well as a consistency estimation (between different batches of the same drug). Though replacing the RPT for many drugs, the BET is a specific assay for endotoxin, not for pyrogenicity.
The MAT as well as the RPT provide information about the biological impact of the sample, whereas the BET determines the endotoxin content (Table 1). Consequently the RPT and the MAT are better performed as end-product assays (a failed batch is lost), whereas the BET due to its speed and precision is additionally valuable as in-process control. In line with the Process Analytical Technology (PAT) initiative established by the FDA it offers the possibility to react during the production based on quick test results. Indeed most of BET are performed on starting materials and in-process controls (including process water). The MAT has a small dynamic range, comparable to the end-point versions of the BET. The MAT is an unspecific test, detecting various Pathogen associated molecular patterns by several receptors.5 The nonspecific nature of the MAT makes it superior to the BET in the assessment of multiple innate immune response modifiers.6 The detection of relevant or unusual endotoxin levels in a sample is a sign of danger, but presence or absence of endotoxin can´t be directly converted into pyrogenicity/absence of pyrogenicity. The BET-activity of various endotoxins compared to the E. coli Standard varies by a factor of up to 1000,7 different endotoxins exhibit different levels of pyrogenicity in the RPT8 or MAT.7,9 The susceptibility of different endotoxins to Low Endotoxin Recovery (LER) or endotoxin masking10 too is depending on structural differences between various endotoxins (additionally depending on sample matrix), highlighting again the diversity of endotoxins.
Table 1. Difference of Pyrogen/Endotoxin Testing: Physiological effect of the sample versus sample content.
The endotoxin regions required for Factor C activation (first reaction step of BET) and membrane receptor binding are different, thus BET in contrast to MAT or RPT can´t distinguish chemically detoxified endotoxin (nonpyrogenic, e.g. MPL derived adjuvants)) from pyrogenic endotoxin.11 Pyrogenicity elicited by Non-endotoxin Pyrogens (NEP)12 and conflicting BET/RPT/MAT results have been reported.13,14
Monocyte Activation Test
Exogenous pyrogens (like LPS) induce the release of endogenous pyrogens, which finally are the elicitors of fever. IL-1ß, IL-6 and TNFα are endogenous pyrogens, if their release exceeds a threshold limit this signal finally induces a shift in the temperature regulation center of the Hypothalamus. As soon as suitable reagents were available, the first approaches to perform in-vitro pyrogen tests were developed.15 These in-vitro pyrogen tests (IVPT) or monocyte activation tests (MAT) follow a similar approach. Human monocytes (whole blood, peripheral blood mononuclear cells (PBMC) or monocytic cell lines) are incubated together with the sample of interest under pyrogen-free conditions (all consumables cell culture grade). At the end of the incubation the supernatants are screened for endogenous pyrogens (mostly IL-6 or IL-1ß), the response is compared to the response elicited by an endotoxin standard curve (or a reference batch of the drug) within the given experiment. The critical endotoxin concentrations are known for the international endotoxin Standard derived from E. coli from animal data1,16 and tests with volunteers.17–19 The derived threshold limits are based on the assumption that endotoxin is the only proinflammatory contamination in the test sample. In contrast to the specific BET, the MAT is able to detect synergistic effects between subfebrile amounts of several contaminations (or a proinflammatory drug).20,21 To resemble the most sensitive RPT (injection of 10 ml sample per kg bodyweight of the rabbit), a MAT must at least detect 50 pg LPS/ml sample (fever threshold of rabbits is 500pg/kg body weight; for 10 ml injection volume this resembles 50pg/LPS per ml).1 Depending on the test setup this minimal sensitivity of 50 pg LPS/ml can be increased to approximately 3 pg/ml.
Endotoxin is the exogenous pyrogen, the pro-inflammatory cytokines are the executors of the endotoxic impact. The comparison of the resulting cytokine levels induced by the samples to the cytokine levels induced by known amounts of standard endotoxin provides an estimation about the pyrogenic potential of the sample. Six variations of MAT had been validated successfully in Europe from 2000-2003,22 an update was conducted in 2004.23 The European MAT Chapter 2.6.30. came into force in 2010. The need to comply with EU Directive 2010/63/EC (protection of animals used for scientific purposes) led to a revision of 2.6.30. (additionally 5.1.10. (Guidelines for using the test for bacterial endotoxins) and 2.6.8. (Pyrogens))), which was finished in 2016. In Europe the RPT is to be replaced by MAT or BET now. The phrasing of the MAT Chapter 2.6.30. was intentionally deduced from the BET Chapter. The MAT-calculations are based on the resulting readout levels induced by either endotoxin (standard), the test sample, and the combination of both (interference test). In the MAT Chapter 2.6.30. the endotoxin Equivalent unit (EEU) was established, 1 EEU equals the amount of readout which is induced by 1 EU (100pg/ml) endotoxin within the given experiment. As 1 EEU = 1 EU, the endotoxin Limit Concentration (ELC) of drugs equals the Contaminant Limit Concentration (CLC) of the drug for the MAT. ELC (or CLC) are calculated by dividing the K-value (depending on the route of administration) by the maximum recommended dose of product per kilogram of body mass (or square meter body surface). If no K-value is defined for the intended application, the endotoxin/Contaminant Limit is determined on results from the development phase.
The typical sensitivity (estimated LOD, eLOD) of the chosen MATversion for endotoxin resembles the Lysate sensitivity (λ) of the BET. If the CLC (equals the ELC) of a product is known, appropriate MATversions can be selected by their stated eLOD. In general, the sensitivity of the MAT can be in increased by expanding the sample volume. The Maximal Valid Dilution (MVD) is derived by dividing the CLC by the eLOD.
Methods A (quantitative Assay) and B (semiquantitative or limit test) are only possible if a MVD can be calculated and valid results (in terms of interference) can be obtained within the MVD. In A and B the product-induced readout level is compared to the readout generated by the endotoxin standard curve.
For products with incalculable MVD (e.g. no K-value), or products where interference can´t be overcome within the MVD or intrinsic pyrogenic products Method C (Reference Lot Comparison Test) is the correct choice. In Method C, the batch under investigation is compared to a reference batch (which might be a pyrogenic (bad) batch or a nonpyrogenic (representative)) batch.
Methodology
According to the revised Monograph 2.6.30. cells intended for pyrogen testing have to be qualified initially for the detection of at least two different NEP. Suitable NEP sources have been described.14 NEP have to exhibit (if at all) an endotoxin contamination far below the detection limit of the chosen MAT. The sensitivity for the endotoxin standard is determined. Typically these QC assurances (including tests for absence of specific blood borne diseases (as for transfusion purposes)) are delivered by the supplier of the cells. If pooled cells are used, the averaging effect should be considered (e.g. stricter safety limits). If the cells are prepared by the user itself, the local legal and ethical requirements as well as safety precautions have to be taken into account.
The methodology has been described extensively.14,22–25 During the incubation phase (37°C, 5% CO2, cell culture breeder) all consumables and media have to be pyrogen free (typically low endotoxin, as tested by BET), at least far below the detection limit of the MAT chosen. Incubation times range from 8 to 24 h.22,23,25 All samples (including endotoxin standard curve and negative control) are incubated in the MAT in four separate wells (true replicates). This is performed to balance the inherent variability of the bioassay, and to facilitate outlier procedures if necessary. The spike concentration is around the middle of the standard curve (Method A) or at 2 eLOD (Method B). The detection is performed by ELISA or other suitable techniques. During the product specific validation, the pure sample should be tested on the ELISA too to exclude interference with the detection system. Dilutions within the MVD with a spike recovery between 50-200% are identified. From these, the product dilution for the batch release is assigned. Three dilutions (including the release dilution) are used in routine testing (Methods A and B). For Methods A and B, the samples are incubated with (interference) and without endotoxin, the resulting analyte release is compared to the levels induced by the endotoxin standard curve. In Method C, the samples are compared to reference samples. The eLOD has to be confirmed within 50-100%, spike recovery has to be between 50-200%.
Example: Human Serum Albumin 50 ml
A manufacturer of 20% HSA detected a pyrogenic 50 ml batch in the RPT. Instead of instantly discarding the batch, the manufacturer kindly offered us this uncommon batch for MAT development as a true pyrogenic sample.
Procedure:
A human serum albumin preparation (50 ml) is to be tested. The eLOD of the MAT chosen is stated to be 50 pg LPS/ml. If 50 ml are chosen as the maximal intravenous human dose for an average adult (70 kg body weight), the CLC is:
CLC = K/M = (5 EU/kg)/(50 ml/70 kg) = 7 EU/ml
MVD = CLC/eLOD = (7 EU/ml)/ (0.5 EU/ml) = 14
For children or cachectic patients lower mean body weights are to be applied. The samples (incriminated batch and marketed batch) were tested in the MAT according to Method B (semi-quantitative or Limit test). A Cryoblood pool of four donors (stored since 150 days at -80°C) was used, the chosen readout was a mix of IL-ß and IL-6.
The samples were tested undiluted, 1:7 and 1:14 (MVD). According to the eLOD of 50 pg/ml the samples were spiked with 100 pg/ml (2 eLOD). The incriminated batch was clearly positive (and therefore different from the marketed batch) undiluted, at the 1:7 dilution and 1:14 (MVD). Spike recovery was very good for all dilutions (Figure 1).
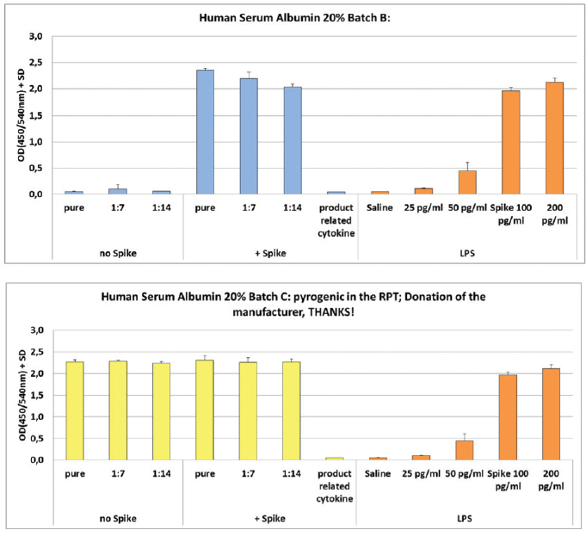 Figure 1. MAT of a nonpyrogenic and pyrogenic HSA 20% batch.
Figure 1. MAT of a nonpyrogenic and pyrogenic HSA 20% batch.If Methods A or B are performed with an eLOD of 50 pg/ml (resembling sensitive rabbits and 10 ml injection volume), a result < 0.5 EEU/ml at the MVD is as safe as the most sensitive rabbit test. If desired, a higher concentration of the test item might be used for release testing. Test sensitivity can be increased by enlarging the sample volume, thus enlarging the MVD too.
Discussion
The MAT was developed to replace the RPT. Mainly not for safety reasons, but to fulfil the legal requirements of animal protection. By choosing a minimal sensitivity for endotoxin of 50pg/ml, the MAT is at least as sensitive as the most sensitive RPT. There is no mandatory need to perform the MAT more sensitive than the RPT for the same product. The more sensitive MAT-setups (eLOD 3-6 pg/ml possible) offer the opportunity for stricter pyrogen testing if required. The capability of the MAT to disclose synergistic effects of multiple stimuli is of special interest in the case of ß-Glucans, which are frequently present as process related impurity in several drugs.26 In contrast to the RPT and the MAT (biological impact of the sample), the BET determines specifically the amount of endotoxin. This is especially relevant during the production of a drug (trending; process analytical technologies). Consequently, much more BET-assays are performed during the production (API, drug substance, process water) of a drug than compared to the final product testing. The RPT in contrast is a typical end product safety test. The MAT is a compendial method in Europe, but until now not in the United States. The USP has announced to create a MAT-Chapter in their current five year plan, they already published a revision proposal of ChapterPyrogens in which the use of validated equivalent in-vitro pyrogen tests is mentioned. The FDA has mentioned both the MAT and the rFc in their 2012 “Guidance for Industry Pyrogen and endotoxins Testing: Questions and Answers”.
A compelling way to replace the RPT would be to implement the MAT on the end product testing, but to keep the BET on the process steps, thus combining the advantages of the MAT (in-vitro pyrogen test) with the known advantages of the BET (specific, fast, trending). The MAT is a necessary replacement for the RPT, and a predictive and versatile tool for special applications (e.g. drugs with intrinsic pyrogenicity; vaccines, adjuvants, detoxified LPS …). The introduction of the MAT as replacement for the RPT will hopefully initiate the further exploration of its capabilities (e.g. Masking/Demasking of endotoxin; selection of representative donor pools (age, gender, genetical background) for various applications). If manufacturers decide to switch from the RPT to the BET, the presence of Non endotoxin pyrogens (NEP) has to be excluded by the MAT (as it has been done in the past by the RPT). If the RPT data are there from the past (indicating no pyrogenic problems apart from endotoxin), no additional animal experiments are required. Variations in the production scheme initiate a further comparison of MAT vs. BET (typically three production batches).
The BET is no animal experiment, but the Lysate is derived from a wildlife stock of animals. The animals survive this well designed procedure, but the demand for Lysate is growing continuously. Consequently the number of animals used for bleeding is growing. All four Horseshoe crab species are listed on the red list of the International union for the conservation of nature (IUCN). The main BET-supplier (Limulus polyphemus; east coast of the USA) is well protected and surveilled, but the situation of the three Asian species is alarming. The implementation of recombinant Factor C (or other recombinant setups) or BET-Assays with reduced Lysate volume would be sustainable, and make the patients, the industry and the regulators less dependent on these fascinating animals.
It’s time to use the new tools. The Paul-Ehrlich-Institut fully replaced the RPT by the MAT, and is currently evaluating recombinant BETAssays for batch release.
Acknowledgements
The authors express their gratitude to the technical staff of the Section 1/3 Microbial safety of the Paul-Ehrlich-Institut, the Members of the EDQM Working Partiy “BET (and MAT)” and various contacts in international agencies and companies for excellent permanent support on the behalf of endotoxin / Pyrogen testing.
References
- Hoffmann, S., Luderitz-Puchel, U., Montag, T., & Hartung, T. Optimisation of pyrogen testing in parenterals according to different pharmacopoeias by probabilistic modelling. J.Endotoxin.Res. 11 (1), 25–31 (2005).
- Williams, K.L. Endotoxins: Pyrogens, LAL testing, and depyrogenation. 2nd ed. Marcel Dekker, New York u.a. (2001).
- Vipond, C., Findlay, L., Feavers, I., & Care, R. Limitations of the rabbit pyrogen test for assessing meningococcal OMV based vaccines. ALTEX 33 (1), 47–53 (2016).
- Gerke, C., et al. Production of a Shigella sonnei Vaccine Based on Generalized Modules for Membrane Antigens (GMMA), 1790GAHB. PLoS ONE 10 (8), e0134478 (2015).
- Hasiwa, N., et al. Evidence for the detection of non-endotoxin pyrogens by the whole blood monocyte activation test. ALTEX. 30 (2), 169–208 (2013).
- Verthelyi, D. & Wang, V. Trace levels of innate immune response modulating impurities (IIRMIs) synergize to break tolerance to therapeutic proteins. PLoS ONE 5 (12), e15252 (2010).
- Dehus, O., Hartung, T., & Hermann, C. Endotoxin evaluation of eleven lipopolysaccharides by whole blood assay does not always correlate with Limulus amebocyte lysate assay. J.Endotoxin.Res. 12 (3), 171–80 (2006).
- Greisman, S.E. & Hornick, R.B. Comparative pyrogenic reactivity of rabbit and man to bacterial endotoxin. Proceedings of the Society for Experimental Biology and Medicine. Society for Experimental Biology and Medicine (New York, N.Y.) 131 (4), 1154–8 (1969).
- Bache, C., et al. Bordetella Pertussis Toxin does not induce the release of pro-inflammatory cytokines in human whole blood. Med.Microbiol.Immunol. 201 (3), 327–35 (2012).
- Reich, J., Lang, P., Grallert, H., & Motschmann, H. Masking of endotoxin in surfactant samples: Effects on Limulus-based detection systems. Biologicals journal of the International Association of Biological Standardization 44 (5), 417–22 (2016).
- Brandenburg, K., Howe, J., Gutsman, T., & Garidel, P. The expression of endotoxic activity in the Limulus test as compared to cytokine production in immune cells. Curr.Med.Chem. 16 (21), 2653–60 (2009).
- Huang, L.Y., Dumontelle, J.L., Zolodz, M., Deora, A., Mozier, N.M., & Golding, B. Use of tolllike receptor assays to detect and identify microbial contaminants in biological products. J.Clin.Microbiol. 47 (11), 3427–34 (2009).
- Perdomo-Morales, R., Pardo-Ruiz, Z., Spreitzer, I., Lagarto, A., & Montag, T. Monocyte Activation Test (MAT) reliably detects pyrogens in parenteral formulations of human serum albumin. ALTEX. 28 (3), 227–35 (2011).
- Solati, S., Aarden, L., Zeerleder, S., & Wouters, D. An improved monocyte activation test using cryopreserved pooled human mononuclear cells. Innate immunity (2015).
- Dinarello, C.A. Cytokines as endogenous pyrogens. J.Infect.Dis. 179 Suppl 2 (0022-1899 (Print)), S294-S304 (1999).
- Spreitzer, I., Fischer, M., Hartzsch, K., Luderitz-Puchel, U., & Montag, T. Comparative study of rabbit pyrogen test and human whole blood assay on human serum albumin. ALTEX. 19 Suppl 1 (0946-7785 (Print)), 73–5 (2002).
- Hochstein, H.D., Fitzgerald, E.A., McMahon, F.G., & Vargas, R. Properties of US Standard Endotoxin (EC-5) in human male volunteers. Journal of Endotoxin Research 1, 52–6 (2010).
- Suffredini, A.F., Hochstein, H.D., & McMahon, F.G. Dose-related inflammatory effects of intravenous endotoxin in humans: evaluation of a new clinical lot of Escherichia coli O:113 endotoxin. J.Infect.Dis. 179 (5), 1278–82 (1999).
- Engler, H., Benson, S., Wegner, A., Spreitzer, I., Schedlowski, M., & Elsenbruch, S. Men and women differ in inflammatory and neuroendocrine responses to endotoxin but not in the severity of sickness symptoms. Brain Behav. Immun.
- Pardo-Ruiz, Z., Menéndez-Sardiñas, D.E., Pacios-Michelena, A., Gabilondo-Ramírez, T., Montero-Alejo, V., & Perdomo-Morales, R. Soluble β-(1,3)-glucans enhance LPS-induced response in the monocyte activation test, but inhibit LPS-mediated febrile response in rabbits: implications for pyrogenicity tests. European journal of pharmaceutical sciences official journal of the European Federation for Pharmaceutical Sciences (2015).
- Kikkert, R., Bulder, I., Groot, E.R. de, Aarden, L.A., & Finkelman, M.A. Potentiation of Tolllike receptor-induced cytokine production by (1-->3)-beta-D-glucans: implications for the monocyte activation test. J.Endotoxin.Res. 13 (3), 140–9 (2007).
- Hoffmann, S., et al. International validation of novel pyrogen tests based on human monocytoid cells. J.Immunol.Methods 298 (1-2), 161–73 (2005).
- Schindler, S., et al. International validation of pyrogen tests based on cryopreserved human primary blood cells. J.Immunol.Methods 316 (1-2), 42–51 (2006).
- Daneshian, M., Aulock, S. von, & Hartung, T. Assessment of pyrogenic contaminations with validated human whole-blood assay. Nat Protoc 4 (12), 1709–21 (2009).
- Koryakina, A., Frey, E., & Bruegger, P. Cryopreservation of human monocytes for pharmacopeial monocyte activation test. J. Immunol. Methods 405, 181–91 (2014).
- Barton, C., et al. Beta-glucan contamination of pharmaceutical products: How much should we accept? Cancer immunology, immunotherapy CII 65 (11), 1289–301 (2016).