Introduction
Due to the increasing prevalence of poorly water soluble compounds entering drug development, lipid-based formulations are taking an important role in enhancing the bioavailability of these drugs and bringing them to the marketplace. While they often lead to dramatic increases in drug solubilization, dissolution, and absorption, special challenges can be encountered as they are brought through development. This review summarizes the approaches that can be taken to bring a lipid-based formulation through the various stages of the drug development process.
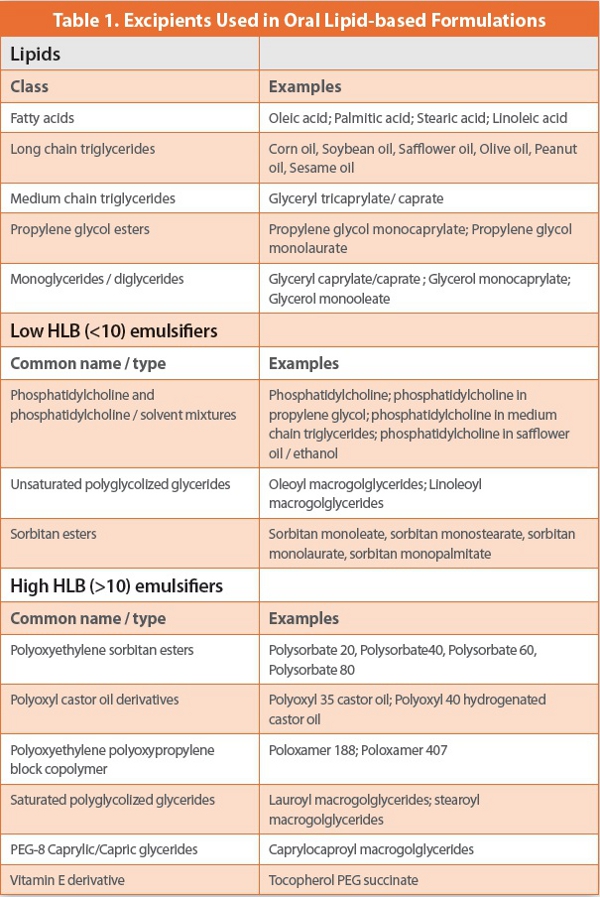
When a drug candidate is recognized to be poorly water soluble and require special delivery systems to enhance absorption, lipid-based formulations should be considered. Pre-clinical experiments should examine the solubility of the compound in excipients commonly used in lipid-based formulations; these are summarized in Table I. Along with lipids (fatty acid derivatives), surfactants are generally used to assure adequate dispersion of the formulation; these can be classified by their Hydrophilic-Lipophilic Balance (HLB) number. More lipophilic surfactants have a low value (≤10) while more hydrophilic ones have a higher value (≥10). Co-solvents such as propylene glycol, ethanol, PEG400, and glycerol may be necessary to increase solubilization. As reviewed earlier [1], a lipid-based formulation should not only solubilize adequate amounts of the drug, but also facilitate dispersion of the dosage form in the intestinal milieu, solubilize the drug in the dispersed form, adapt to the digestive processes of the GI tract such that drug solubilization is maintained or enhanced, and facilitate absorption of the drug into the intestinal mucosal cells and into the systemic circulation. Excipient combinations and formulations should be screened with these ends in mind. The most successful lipid-based formulations are self-emulsifying drug delivery systems (SEDDS), since they spontaneously form an emulsion upon addition to an aqueous medium (such as the intestinal milieu) with gentle agitation. SMEDDS (self-microemulsifying drug delivery systems) are self-emulsifying systems that form microemulsions upon addition to water. Toxicology formulations will typically be used as a starting point for designing clinical formulation candidates, provided that the additional constraints of safety and stability required for a clinical formulation are taken into account. Ideally, only excipients currently approved by the US Federal Drug Agency (FDA) should be used, in amounts already established as safe, as outlined in the approved inactive ingredients list of the FDA (http://www.accessdata.fda.gov/scripts/cder/iig/index. cfm). If novel excipients are required, regulatory hurdles will be encountered later in the development process, since safety of novel excipients is currently only evaluated in the context of a New Drug Application (NDA). Nevertheless, pathways exist for approval for novel excipients, requiring close cooperation between the pharmaceutical company and excipient manufacturers [2]. For example, tocopherol PEG succinate (tocophersolan) is a water-soluble (HLB ~13) Vitamin E derivative that can enhance solubilization and absorption of poorly water soluble drugs [3]; it was first used in the commercial formulation of the HIV protease inhibitor Amprenavir [4]. Dispersion characteristics of candidate formulations can be evaluated by microscopic observation of the formulation when mixed with water and verified by absence of drug precipitate after mixing of the formulation with water. Particle size measurement of the resulting emulsion droplets by laser light scattering is useful. Construction of ternary phase diagrams can be used to characterize behavior of a formulation along a dilution path. Finally, animal studies can identify formulations that yield adequate bioavailability. Design of oral lipid-based formulations is still largely an empirical exercise, but as reviewed earlier [1], strategies can be used to expedite the process at the early stages. Pouton has proposed a classification system for lipid-based formulations based on the formulation components and their dependence on digestion to facilitate dispersion [5,6]. Type I formulations are simple drug in triglyceride or mixed glyceride formulations; Type II formulations additionally have lipophilic surfactants to improve the dispersibility; Type III formulations are selfemulsifying systems with hydrophilic surfactants and cosolvents; and Type IV systems are composed only of surfactants and cosolvents. Type I, as well as Type II formulations to a lesser extent, are dependent on the action of intestinal lipases to initiate emulsification and absorption, but are generally efficient at maintaining drug solubilization at all stages of intestinal processing. Type III and especially Type IV formulations, while not dependent on digestion by lipases for emulsification, may be more prone to drug precipitation during intestinal processing due to the co-solvent content. When the formulation is diluted in the aqueous medium, co-solvent will likely diff use away from the emulsion droplets or micelles, decreasing drug solubility. Whichever type formulation is used, the end result of the digestion process is formation of emulsion droplets and bile salt-lipid mixed micelles from which drug will diff use and be absorbed by the intestinal mucosal cells; the high surface area of small droplet or micelle size facilitates diffusion and absorption. These guiding principles for design of lipid-based formulations are summarized in the review by Porter et al. [6].
Phase I: Formulation Approaches
Once one or more lipid-based formulations are chosen to take forward to clinical trials, a number of options are available, depending on the requirements and time constraints of the project. Normally, the purpose of First-in-Human studies is for proof-of-concept of the drug’s safety and efficacy, and the primary goal is frequently to reach the clinic as fast as possible. In this case, the simplest approach for a lipid-based formulation would likely be a ready-to-use liquid formulation in which the drug is dissolved in the lipid / surfactant / co-solvent mixture. This requires verification of at least 6 months of both chemical and physical stability of the formulation. If refrigeration is required, absence of phase changes and drug precipitation must be verified. The formulation could either be administered as is or diluted in a suitable aqueous medium to form an emulsion. In either case, taste and “mouth-feel” could be a disadvantage, which would be difficult to assess before the formulation actually reached the clinic. An advantage of this approach would be flexibility of dosage. If 6 months stability cannot be attained within the time constraints of the project, a “powder-in-bottle” approach can be examined. Manufacture consists of filling weighed amounts of the drug powder, or a simple solid drug-excipient blend, into the required number of suitable containers; a lipid / surfactant /co-solvent blend is prepared and weighed into other containers. The drug powder and the lipid mixture are then combined as needed at the clinical site and administered either as-is or as an emulsion in a manner similar to the ready-to use formulation described earlier. Stability and compatibility studies must be carried out to support all steps in the preparation and dilution process for the storage period required (generally at least 24 hours). Considerable training may be required for all personnel involved at the clinical site, since the reconstitution process will generally not be straightforward. Significant mixing time and even heating may be required to mix the drug with the possibly viscous lipid blend. The drug powder could be mixed with co-solvent prior to addition to the lipid-surfactant blend, but this would add a level of complexity that may not be feasible at the clinical site. Just as with a ready-to-use lipid formulation or emulsion, taste and “mouth-feel” could be a problem.
If the development timeline allows and/or if the ready-to-use liquid and powder-in-bottle approach are impractical due to stability problems or formulation complexity, a liquid or semi-solid formulation in a capsule can be evaluated. Capsules offer greater convenience in the clinic, and there are no taste issues. Dose ranging can be done by varying the number of capsules administered, and several capsule strengths (of different fill weights or drug concentration) can be manufactured. Furthermore, development time at later stages may be saved since the Phase I formulation is closer to the final formulation at launch, and information is gained which will be helpful at the later stages of development. Many lipid-based drug products are liquid in soft-gel capsules. However, this requires specialized equipment for manufacture and relatively large batch sizes, thus requiring a third-party manufacturer for most pharmaceutical companies. Thus, a liquid formulation in a hard gelatin capsule may be a more viable option for Phase I studies, since equipment is less expensive and smaller batch sizes are possible. Not only must adequate stability (at least 6 months) of the fill be verified, but also compatibility of the fill and shell with one another over the same time period must be monitored. Capsule softening, shell brittleness, and leakage of fill are all possible problems. Hydrophilic components such as ethanol, propylene glycol, and glycerol are particularly prone to lead to fill-shell incompatibilities. Glycerol can be an impurity in some mono- and di-glyceride lipid excipients, and levels must be carefully controlled. Semi-solid fills can also be evaluated, which may ameliorate some of the compatibility problems. However, semi-solids have potential physical stability problems. Semi-solids may require more time for development and may be more difficult to characterize. The potential for drug precipitation in the fill increases over time, with an associated decrease in bioavailability [7].
Development of Phase II/III and Commercial Formulations
After the drug has proven safe and efficacious, and the advantages of a lipid-based formulation have been demonstrated, attention must be turned to identifying formulations that can be the commercial formulation. The formulation must be robust, capable of reproducible and easily controlled manufacture, with minimal batch-to-batch variation in composition, characteristics, and performance. In earlier stages, characterization tests are primarily for functional performance, and carried out to assess drug solubility in the vehicle, dispersion characteristics, and bioavailability; stability studies verify that there was minimal loss of drug potency and no significant change in these functional characteristics. While these are still important at later stages, these tests must be complemented or replaced by those that best identify sources of batch-to-batch variability, monitor critical manufacturing parameters, and give meaningful specifications. One must recognize that the analytical tests and characterizations used earlier during development will not necessarily be those tests that are suitable to set specifications.
In particular, more attention must be paid to excipient composition. Lipids are frequently from natural sources and thus prone to variability in composition such as fatty acid chain length and degree of unsaturation; developers must work closely with vendors to assure that their supply is well-characterized and consistent with regard to these attributes. Ideally, a formulation will be chosen whose performance allows some variability in lipid chain length, unsaturation, and other properties. Batches can be prepared from different lots of excipients with a range of properties at both ends of the vendors’ specifications to assure that normal variability in excipient composition will not lead to failure of the drug product’s performance. Presence of peroxides in the excipients can be significant in lipids and particularly for PEG-based surfactants. The iodometric assay is the accepted USP method to assess lipid peroxide levels [8]. Addition of antioxidants to the formulation is always advisable, since peroxides may lead to drug instability. Aldehydes and dialdehydes can be produced by lipid peroxidation, which will likely result in gelatin crosslinking and an altered dissolution profile. Since the peroxidation pathway is complex due to the peroxide decomposition, use of a single assay to assess peroxidation in the drug product may not reflect the extent of peroxidation. Supplementation of the iodometric assay with other assays (e.g., thiobarbituric acid reactive substances assay, HPLC for specific aldehydes,and Rancimat assay) can be considered [7]. Stability studies for lipid-based dosage forms must be carefully designed to provide meaningful results. Accelerated testing at elevated temperatures may give misleading results due to possible phase changes in the fill and changes in shell-fill interactions.
There has been much debate over the most appropriate dissolution tests for poorly water-soluble drug products and for lipid-based formulations in particular. Due to the difficulty of achieving sink conditions, traditional dissolution tests in buffer are often meaningless, and in vitro-in vivo correlations are often poor. Addition of surfactants to the dissolution medium to achieve sink conditions will likely alter the dispersion properties of the formulation and give misleading results. In vitro dissolution testing in biorelevant media (i.e., simulated intestinal fluids) such as those developed by Dressman may be more appropriate [10]. Since digestion and formation of colloidal species by the intestinal milieu may be critical to the in vivo properties of a formulation, in vitro lipolysis models, as described by Mullertz [11,12] and by Dahan [13], may also be used to assess the effects of digestion on drug solubilization and release from the formulation. As mentioned earlier, tests for dispersion and dissolution specifications should assess both functional performance and also monitor batch-to- batch variability. Although some guidelines have been established for dissolution testing of poorly soluble compounds [14], choice of appropriate tests will have to be assessed on a case-by-case basis. As data is gathered on multiple candidate formulations in the clinic, those tests that give the most meaningful in vitro-in vivo correlation should be identified and modified as needed for final specifications.
Final Dosage Forms
Several choices exist for the final dosage form of a lipid-based formulation. Table 2 summarizes representative products currently or previously marketed as lipid-based formulations. Most of these are liquid formulations in soft-gelatin capsules. This requires third party manufacture but may offer several advantages. These include providing adequate drug solubilization and loading; affording robust and convenient dosage forms without leakage; and yielding favorable dissolution, release, and bioavailability properties. Recently, non-gelatin based soft capsules such as starch and hydroxypropylmethyl cellulose (HPMC) have been developed for wider appeal to consumers concerned with the animal origin of gelatin products. It is likely that use of these non-gelatin capsules will become more widely used in marketed products.

An alternative to soft capsules is hard gelatin capsules with liquid or semi-solid fill. Several kinds of equipment are available for filling; to prevent leakage, the capsules must be sealed or banded after filling. Sealing is accomplished by spraying an ethanol solution around the capsule joint, whereas banding involves wrapping a gelatin fi lm around the seal. Hard gelatin capsules are more prone to shell-fill incompatibilities than are soft-gel capsules and less tolerant of hydrophilic fill excipients. HPMC and other non-gelatin hard capsules are also available and should be considered. Shell-fill compatibility of gelatin and HPMC capsules differ significantly and must be evaluated separately. Semi-solid fills may also retard leakage but often present physical stability challenges. Mono-, di-, and triglyceride lipids often exhibit polymorphism, which can change during manufacture and storage of the formulation. The resulting dynamic nature makes controlling the phase changes and physical stability of semi-solids particularly challenging [15]. Drug crystallization may be induced by the phase changes of semi-solids, as exhibited in an extreme case by the protease inhibitor ritonavir, in which a new less soluble drug polymorph appeared in the semisolid lipid-based formulation [16]. Manufacture and filling of semisolids generally must be carried out at elevated temperature (40°- 70°C), and care must be taken that no drug degradation or capsule softening occurs under these conditions.
In some cases, a lipid-based formulation can be adapted to a traditional solid dosage form, i.e., a powder in hard capsule or even a tablet. One approach is dry emulsions (also called solid-state emulsions), wherein the drug is dissolved in a lipophilic solvent, which is combined with an aqueous phase containing bulking agents (cryoprotectants) [17]. After homogenization to form an emulsion, water is removed by lyophilization, spray drying, or granulation, and the dry powder is filled into capsules or compressed into tablets. In liquisolid compacts, drug is dissolved in a non-aqueous solvent and adsorbed onto a solid carrier; the solid can be then compressed into tablets or filled into capsules. An example is a Coenzyme Q10 self-emulsifying mixture containing lemon oil, polyoxyl 35 castor oil, and Glyceryl caprylate/caprate adsorbed onto a maltodextrin / microcrystalline cellulose carrier [18]. Both the liquid-solid compact and dry emulsion approaches have the disadvantage of low drug loading due to the requirement for high content of solid excipients in the carrier. These approaches may be suitable for high potency drugs with high solubility in lipid vehicles, and avoid the problems of shell-fill incompatibility and leakage. Other advantages include use of standard encapsulation or tabletting equipment and potentially better stability relative to liquid and semisolid fill formulations.
Lipid-based formulations can also be solid dispersions, using solid lipids and surfactants. The drug is first combined with the solid matrix component and the blend melted. The melt can then be filled directly into capsules and cooled; chilled and pulverized or spray congealed to form solid particles, which are then be filled into capsules or compressed into tablets; or extruded directly into tablets. Saturated polyglycolized glycerides are often used for this purpose [15]. As with semi-solids, drug must be thermally stable during manufacture, and must remain solubilized or amorphous in the solid dispersion formulation during storage. Changes in crystallinity in the matrix material can occur, potentially altering the dispersion and dissolution properties.
In some cases, it may be advantageous to change the dosage form of a marketed drug. For example, the protease inhibitor ritonavir (NorvirR) was first marketed as a semi-solid in a hard gelatin capsule; drug was solubilized in caprylic/capric triglycerides, polyoxyl 35 castor oil, citric acid, ethanol, polyglycolized glycerides, polysorbate 80, and propylene glycol. After the appearance of the less soluble polymorph, ritonavir was re-formulated in a soft-gel capsule; drug was solubilized in a fill composed of oleic acid, ethanol, and polyoxyl 35 castor oil. The second generation protease inhibitor ritonavir / lopinavir (KaletraR) was first formulated in a soft-gel capsule. Drug was solubilized in a fill composed of oleic acid, propylene glycol, and polyoxyl 35 castor oil; the product required refrigerated storage and dosage of 6 capsules daily. It was later re-formulated as a solid dispersion tablet composed of copovidone, sorbitan monolaurate, colloidal silicon dioxide, and sodium stearyl fumarate, which allowed storage at room temperature and a dosage of 4 tablets daily. Cyclosporine was one of the first compounds administered as a lipid-based formulation. The original product, SandimmuneR (Table 1) was a SEDDS formulation that gave a fine emulsion upon dilution in water, while the product developed subsequently, NeoralR, was a SMEDDS, and gave a microemulsion upon dilution, with about 25% higher bioavailability [19].
In conclusion, development of lipid-based formulations can be challenging at all stages of the drug development process. Nevertheless, they are a vital tool in bringing poorly soluble drugs to the marketplace. As greater understanding and experience is gained on the critical attributes important for their performance, they should gain more widespread use.
References
1. Cannon, J.B. Strategies to Formulate Lipid-based Drug Delivery Systems. Amer. Pharm. Rev. 14: 84-92 (2011)
2. Goldring, J. Novel Excipients: The Next Pharmaceutical Frontier. Amer. Pharm. Rev 12: 56-59 (2009).
3. Wu, S.H., and Hopkins, W.K. Characteristics of D-alpha tocopheryl PEG 1000 succinate for Applications as an absorption enhancer in drig delivery systems. Pharm. Tech., October 1999, 52-58.
4. Strickley, R.G. Solubilizing Excipients in Oral and injectable formulations, Pharm. Res. 21: 201- 230, (2004).
5. Pouton, C.W. Lipid formulations for oral administration of drugs: non-emulsifying, selfemulsifying and ‘self-microemulsifying’ drug delivery systems. Eur. J. Pharm. Sci. 11 Suppl. 2 S93-S98, (2000).
6. Porter CJ, Pouton CW, Cuine JF, Charman WN. Enhancing intestinal drug solubilisation using lipid-based delivery systems. Adv Drug Deliv Rev., 60: 673-91, (2008).
7. Cannon, J.B. Chemical and Physical Stability Considerations for Lipid-Based Drug Formulations. Amer. Pharm. Rev. 10: 132-138 (2007).
8. N.A. Porter . Chemistry of lipid peroxidation. Meth. Enzymol. 105: 273 (1984).
9. Wasan, K.M. Formulation and Physiological and Biopharmaceutical Issues in the development of oral lipid-based drug delivery systems. Drug Dev. Indust. Pharm. 27: 267-276 (2001).
10. Dressman JB, and Reppas C. In vitro-in vivo correlations for lipophilic, poorly water-soluble drugs. Eur J Pharm Sci., 11 Suppl 2: S73-80, (2000).
11. Zangenberg NH, Mullertz A, Kristensen HG, and Hovgaard L. A dynamic in vitro lipolysis model. I. Controlling the rate of lipolysis by continuous addition of calcium. Eur J Pharm Sci., 14: 115-22 (2001).
12. Zangenberg NH, Mullertz A, Kristensen HG, and Hovgaard L. A dynamic in vitro lipolysis model. II: Evaluation of the model. Eur J Pharm Sci., 14: 237-244 (2001).
13. Dahan A, Hoff man A. Rationalizing the selection of oral lipid based drug delivery systems by an in vitro dynamic lipolysis model for improved oral bioavailability of poorly water soluble drugs. J Control Release, 129: 1-10 (2008).
14. Brown, C.K., Chokshi, H.P., Nickerson, B., Reed, R.A., Rohrs, B.R., and Shah, P. A. Acceptable Analytical Practices for dissolution testing of poorly soluble compounds. Pharm. Tech. 28: 56-62 (2004)
15. Jannin V, Musakhanian J, Marchaud D. Approaches for the development of solid and semi-solid lipid-based formulations. Adv Drug Deliv Rev., 60: 734-46, (2008).
16. Bauer J., Spanton, S. Henry, R. Quick, J. Dziki, W. Porter, W. and Morris, J. Ritonavir: an extraordinary example of conformational polymorphism. Pharm. Res. 18: 859-866, (2001).
17. Cannon, J.B., Oral Solid Dosage Forms of Lipid-based Drug Delivery Systems. Amer. Pharm. Rev., 8: 108-113, (2005)
18. Nazzal, S., Nutan, M., Palamakula, A., Shah, R., Zaghloul, A. A., and Khan, M. A. Optimization of a self-nanoemulsified tablet dosage form of Ubiquinone using response surface methodology: effect of formulation ingredients . Int. J. Pharm. 240: 103-114, (2002).
19. Constantinides, P.P., Lipid Microemulsions for improving drug dissolution and oral absorption: physical and biopharmaceutical aspects. Pharm. Res. 12: 1561-1572 (1995).
Author Biography
Dr. John Cannon is president of a drug delivery and pharmaceutics consulting firm, Targeted Drug Solutions, Inc. He received a B.S. in Chemistry from Duke University, and a Ph.D. in Organic Chemistry from Princeton University. Dr. Cannon served in faculty positions at Northern Illinois University and Cleveland State University (Ohio). He retired from Abbott Laboratories in 2007 after a 20 year career as a pharmaceutical scientist, focusing on oral lipid-based formulations, liposomes, emulsions, and topical / transdermal delivery. Dr. Cannon coauthored a book, Drug Delivery Systems, 3rd edition, and has published about 30 papers, 12 book chapters, and 5 patents.