Background
The need for better drug therapy for newborns, infants, children and youth is beyond debate. Although there is a record of concern about remedies for children dating back to the ‘Boke of Children’ published by Thomas Phaire in 1544 [1], progress in drug therapy was agonizingly slow until the modern era.
Beginning with recognition of some highly publicized childhood misadventures in the middle of the 20th century [2-4], focus on appropriate investigation of drug therapy in the pediatric population has emerged and interest has greatly accelerated since 1990. Beginning two decades ago, pediatricians became much more active in their demands for products with adequate product labeling and this has progressed to major efforts made in the United States and Europe to better serve the needs of the pediatric population through relevant regulatory and policy reform [5-7].
Recent data suggest that, for the first time, a majority of drugs likely to be used in care of children are now receiving appropriate research attention before licensure [8]. Furthermore, specific efforts have been made to encourage the study of drugs previously licensed with appropriate prescribing information for use in adults with the aim of extending the knowledge base to support labeling for use in children and youth [9].
This overdue interest has more recently spread to the European Community where legislation was introduced in 2007 requiring companies filing for licensure of new products to submit a Pediatric Investigation Plan unless there was no potential for use in children [10].
In both the United States and in the European Community, the policy changes introduced to encourage improved therapeutics for children have been accompanied by initiatives aimed at the development of infrastructure needed to support better labeling of drugs. In the United States this began with the support of Pediatric Pharmacology Research Units by the National Institute for Child Health and Human Development (NICHD) [11] and in Europe relevant initiatives have been supported under recent Framework Programs, including, since 2007, Framework Program 7 which has featured dedicated programs fostering therapeutic investigations both for children and for those suffering from rare disorders [12].
The Hidden Iceberg
Perhaps in this year of the Titanic centenary, we may consider the iceberg-like qualities of the challenges faced in achieving optimal therapy for children. While we are conscious of urgent needs, there are numerous challenges beneath the surface.
For a long time it was considered that the need for drug therapy in pediatrics was relatively rare, apart from the need for nutritional supplements, vitamins, anti-asthmatic drugs, seizure medications, vaccines and treatments for various communicable diseases. Indeed, there are few reports available that permit the accurate gauging of the absolute requirements worldwide for pediatric therapies; however, a number of published studies do illustrate surprisingly extensive prescribing for this age group, at least in the developed world [13-17]. From these studies it is apparent that there that has been an iceberg on the horizon for the last century that can no longer be ignored without placing the world’s childhood population in considerable peril.
 There have been two Copenhagen Consensus conferences convening leading experts including Nobel prize winners in economics and posing the question of what would be the most cost effective initiatives worldwide in health, wellness and survival [18]. At both consensus conferences the experts have agreed on a list of essential initiatives that, perhaps not surprisingly, has a disproportionate focus on measures to improve child health. While many of the recommended actions, such as provision of micronutrients, zinc and iron, or improvement in worldwide availability of vitamin A fall into the arena of preventive therapies, there is also a pressing need for drugs that may be used to manage scourges of children in tropical and low income settings, such as malaria, helminthic diseases and HIV/AIDS.
There have been two Copenhagen Consensus conferences convening leading experts including Nobel prize winners in economics and posing the question of what would be the most cost effective initiatives worldwide in health, wellness and survival [18]. At both consensus conferences the experts have agreed on a list of essential initiatives that, perhaps not surprisingly, has a disproportionate focus on measures to improve child health. While many of the recommended actions, such as provision of micronutrients, zinc and iron, or improvement in worldwide availability of vitamin A fall into the arena of preventive therapies, there is also a pressing need for drugs that may be used to manage scourges of children in tropical and low income settings, such as malaria, helminthic diseases and HIV/AIDS.
Any attempt to prioritize the greatest needs for improved pediatric treatment would be beyond the scope of this commentary; however, some representative priorities are displayed in Box 1. More refined prioritization will vary from one jurisdiction to another.
It is notable that many international organizations concerned with the welfare of children have come recently to focus heavily on their nutritional and therapeutic needs. This phenomenon explicitly recognizes the amazingly cost effective gains that can be made through provision of preventive therapies or active treatments for the common childhood conditions that are causing intolerably high levels of under-five mortality in many parts of the world [19]. Among organizations that have invested heavily in pursuit of better medicines for children, the World Health Organization, UNICEF, Save the Children Fund, Bill & Melinda Gates Foundation and Clinton Foundation stand out for their exemplary efforts.
An International Issue
While progress has been most notable in the United States and the European Community, there is growing recognition of the need for better drug therapy worldwide and leadership in this regard has been taken by the World Health Organization. The World Health Assembly, in 2007, passed a Better Medicines for Children proposal (WHA resolution 60.20) [20]. Following that landmark event, an essential medicines list for children was introduced and has now gone through two revisions [21]. The WHO has also introduced a formulary for children which represents a good start on the development of standard treatment guidelines that may be applied in a variety of settings [22].
Recent articles have highlighted the need for concerted effort in pediatric clinical pharmacology, clinical pharmacy and clinical toxicology in a variety of settings, including Latin America, Africa, Japan, China and Canada [23-27}. Investigators from the key clinical and research disciplines in this domain have also been engaged in active discussions since 2006 and have created an International Alliance for Better Medicines for Children that will bring together the nucleus of investigators from all continents possessing the research and educational capacity needed to make a difference in drug therapy for children [28].
None of the future progress required will be possible unless the methodology for study of drugs in newborns, infants, children and youth is improved. Toward that end, a new organization, StaR Child Health, has emerged with close links to the Cochrane International Collaboration. StaR Child Health has now held three meetings, Amsterdam in 2009, Vancouver, Canada in 2010 and Winnipeg, Canada in 2012 [29]. While StaR Child Health emphasizes the overall need for improved and innovative trial methodology in pediatric studies, it has also been attentive to particular conditions impeding much needed clinical research studies on innovative therapies urgently required in low and middle income countries.
Origins of the Knowledge Gap
There are many reasons why drug therapies have not been adequately studied in pediatric populations, either from the perspective of benefit or risk. Rieder et al [30] attempted to summarize the main factors impeding systematic study of drugs in the pediatric population and identified the following reasons.
- Infants, children and youth are prescribed fewer drugs than adults and for shorter time periods. These challenges are amplified even further in neonatology. Neonates, in many respects, represent a totally different population.
- Drug development costs are higher than in adult medicine and there is the perception that the potential for financial return is limited.
a. Manufacturers would likely be required to conduct separate studies for different age groups, including, neonates, infants, children and youth up to adulthood.
b. There would be a requirement for manufacturers to develop age appropriate formulations of any proposed innovative therapeutic product.
- Trial recruitment is complicated by the reluctance of parents to consent to study participation.
- Additional ethical issues, including the need for assent, must be considered when enrolling infants and children in research studies.
- The conduct of pediatric clinical trials introduces technical and logistical challenges, including difficulties in sampling, for example, obtaining of adequate blood samples from low birth weight infants. In pharmacokinetic studies, sparse sampling must be accommodated through innovative design.
- Statistical analysis of studies involving small numbers of research participants must be addressed through use of methods such as population pharmacokinetics.
Recent American Experience: Grounds for Cautious Optimism
The ideal mechanism to achieve essential pediatric drug investigation often remains contentious inside governments, across governments, within academia and in the clinical practice community.
The most notable progress of recent years has been the creation of the Pediatric Trials Network (PTN) by the NICHD in 2010 [31]. The leadership of this Network was awarded competitively to the Duke University Clinical Trials Institute and early success has been exceptional. The Network was designed to comprehensively cover all aspects of needed innovation in pediatric clinical trials and became operative almost immediately with seven studies approved within the initial six months. All studies address the required further understanding of optimal use of off -patent medications in the pediatric population. Protocols receiving early approval include trials of anti-infective agents in newborns, the use of hydroxyurea in sickle cell disease and the choice of antihypertensive treatments for children and adolescents.
The PTN program has built on earlier experience within the NICHD Neonatal Research Network, where particular success has been achieved in the study of antifungals and other anti-infectives [32-35]. Research is effectively organized around a number of cores, including program management and clinical operations, clinical pharmacology, pharmacometrics, safety and ethics, devices and mentorship [31]. The early achievements of this program bode well for continued American leadership in pediatric clinical investigation of off -patent therapies.
While the needs of developed countries will increasingly be met by well-funded clinical trial initiatives such as those now emerging in Europe, America, and elsewhere, the needs for research support for optimal therapy targeting children in low and middle income countries will remain distinctly different and require resourceful innovation. A summary of pressing research gaps is presented in Box 2.
Knowledge Translation, Knowledge Mobilization and Implementation Science
Perhaps the greatest challenge in achievement of optimal therapy for children lies in capitalizing on the knowledge base that we already possess. Notwithstanding the many obstacles described above, there is a considerable amount known about physiological development across the trajectory of childhood and our understanding is considerable concerning the impact of such development on drug disposition, drug safety and action [36, 37]. Nonetheless, because of the paucity of evidence from appropriately designed clinical trials, the evidence base concerning age-related variation in drug mechanisms of action and adverse reaction remains less than adequate. Efforts to standardize treatment guidelines suffer accordingly. 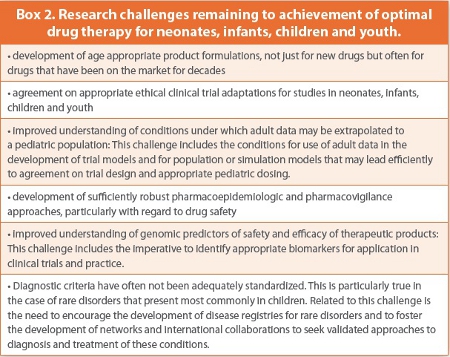
Failure to use the knowledge already at hand is inexcusable. Many have written about the need to close the gap between knowledge and action [38]. This ‘know-do gap’ is particularly important in low and middle income countries where most of the world’s children reside [39]. In the dire circumstances that prevail in many of the poorer parts of the world, neither time nor human energy should be wasted in poorly designed research studies. The current levels of under-five and maternal morbidity and mortality demand better drug therapy. Every effort must be made to assure that both public and clinical policy reflect the best current research knowledge and innovative research in basic sciences, social sciences, clinical sciences and implementation sciences must be encouraged.
Efforts such as those made by Canada’s International Development Research Centre are commendable in this regard [39]. This has also been an ongoing concern of the StaR Child Health initiative [38].
Next Steps
An iceberg of considerable proportion looms before us. We have been remiss in discounting the importance of pediatric clinical research targeting optimally safe and effective drug treatment. The world’s population has just exceeded seven billion in 2011 and more than one third of this population is under the age of 15. In some countries, such as Uganda, the median age is under 15. Even in a world where a majority of children can expect to receive good nutrition and good healthcare, there will still be an immense need for access to appropriate therapies for disease prevention and for active treatment. Manifestly, the world does not yet provide an ideal sociopolitical or economic environment and the majority of children worldwide are not only at considerable risk of malnutrition and communicable disease, but they are also likely to lack access to necessary diet and validated therapies. As the pediatric population continues to expand, many of these deficiencies will be amplified unless specific corrective actions are taken. All those who are involved in the care of children must become more effective advocates for improved pediatric research and evidence based treatment guidelines [40]. Effective alliances must be formed, engaging governments, research centers, philanthropic organizations, caregivers, children and families in an effective alliance to circumvent the hazards that so obviously lie before us.
References
1. T.E.C. Jr. The Boke of Children (1544) by Thomas Phaire, the first pediatric text published in English. Pediatrics 1981;2:182.
2. Geiling EMK, Cannon PR. Pathologic effects of elixir of sulfanilamide (diethylene glycol) poisoning. JAMA 1938;111:919-26.
3. Sutherland JM. Fatal cardiovascular collapse of infants receiving large amounts of chloramphenicol. Am J Dis Child 1959;97:761-7.
4. Taussig HB. A study of the German outbreak of phocomelia. JAMA 1962;180:1106-14.
5. United States Food and Drug Administration Modernization Act (FDAMA), 1997. http:// www.fda.gov/RegulatoryInformation/Legislation/FederalFoodDrugandCosmeticActFDCAct/ SignificantAmendmentstotheFDCAct/FDAMA/default.htm [accessed April 09, 2012]
6. United States Food and Drug Administration. Best Pharmaceuticals for Children Act, January 4, 2002. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/ ucm049876.htm [accessed April 09, 2012]
7. Commission of the European Communities. Regulation (EC) No 1901/2006 on medicinal products for paediatric use. http://ec.europa.eu/health/files/eudralex/vol-1/ reg_2006_1901/reg_2006_1901_en.pdf [accessed April 09, 2012]
8. Rodriguez W, Selen A, Avant D et al. Improving pediatric dosing through pediatric initiatives: What we have learned. Pediatrics 2008;121:530-9.
9. Pediatric Research Equity Act of 2007 (PREA). http://www.fda.gov/Drugs/ DevelopmentApprovalProcess/DevelopmentResources/ucm049867.htm [accessed April 09, 2012]
10. European Medicines Agency. Paediatric Investigation Plan. http://www.ema.europa.eu/ema/ index.jsp?curl=pages/regulation/document_listing/document_listing_000293.jsp&mid= WC0b01ac0580025b91&jsenabled=true [accessed April 09, 2012]
11. National Institute of Child Health and Human Development. Pediatric Pharmacology Research Units Network. http://www.nichd.nih.gov/research/supported/ppru.cfm [accessed April 09, 2012]
12. European Commission Research & Innovation. Framework Programme 7: the future of European Union research policy. http://ec.europa.eu/research/fp7/index_en.cfm [accessed April 09, 2012]
13. Khaled LA, Ahmad F, Brogan T, Fearnley J, Graham J, MacLeod SM. Prescription medicine use by one million Canadian children. Paediatr Child Health 2003(Suppl A);8:6A-56A.
14. Schirm E, van den Berg P, Gebben H, Sauer P, De Jong-van den Berg L. Drug use of children in the community assessed through pharmacy dispensing data. Br J Clin Pharmacol 2000;50:473-8.
15. Bertoldi AD, Tavares NU, Hallal PC, Araujo CL, Menezes AM. Medicine use among adolescents: the 11-year follow-up of the 1993 Pelotas (Brazil) birth cohort study. Cad Saude Publica 2010;26:1945-53.
16. Hong SH, Shepherd MD. Outpatient prescription drug use by children enrolled in five drug benefit plans. Clin Ther 1996;18:528-45.
17. Hahn BA. Children’s health: racial and ethnic differences in the use of prescription medications. Pediatrics 1995;95:727-32.
18. Copenhagen Consensus 2008. http://www.copenhagenconsensus.com/Home.aspx [accessed April 09, 2012]
19. Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, Bassani DG, Jha P, Campbell H, Fischer Walker C, Cibulskis R, Eisele T, Liu L, Mathers C for the Child Health Epidemiology Reference Group of WHO and UNICEF. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet 2010;375:1969-87.
20. World Health Organization. 60th World Health Assembly Resolution. WHA 60.20: Better medicines for children, 23 May 2007. http://www.who.int/gb/ebwha/pdf_files/WHA60/ A60_R20-en.pdf [accessed March 27, 2012]
21. World Health Organization. Essential medicines for children: making medicines child size. http://www.who.int/childmedicines/en/index.html [accessed April 10, 2012]
22. World Health Organization. Model Formulary for Children (2010) http://www.who.int/ childmedicines/en/ [accessed April 10, 2012]
23. Arenas-Lopez S, Fajardo C, Valls i Soler A, Garcia-Corzo JR, Lima-Rogel MV, Calle G, Leite R, Lobos E, Hume-Wright Q, MacLeod S. Pediatric clinical trials in Latin America and Guyana: present views of local practitioners and ways to embrace the future. Paediatr Drugs 2011;13:257-65.
24. MacLeod S, Finch J, Anabwani G, Macharia W. Better medicines for the children of Africa. Paediatr Drugs 2012. submitted for publication
25. Ito S, Nakamura H. Paediatric pharmacology in Japan. Paediatr Drugs 2012 in press
26. Li Z, Wang L, Wang Y, Gui YH, Vinks AA, MacLeod S. Better medicines for 300 million children in China. Report on recent progress. Pediatr Drugs 2011;13:137-40.
27. S MacLeod. The plight of pediatric drug therapy. Pediatric Child Health 2011;16:529-31.
28. MacLeod S, Peterson R, Wang Y, Li Z, Gui Y, Schaller J. Challenges in international pediatric pharmacology: A milestone meeting in Shanghai. Pediatr Drugs 2007;9:215-8.
29. StaR Child Health Summit. http://www.starchildhealth.org [accessed April 09, 2012]
30. Rieder MJ, Matsui D, MacLeod SM. Myths and challenges – drug utilization for Canadian children. Paediatr Child Health 2003;8 (Suppl A):7-8A.
31. Pediatric Clinical Trials Network. https://pediatrictrials.org [accessed August 26, 2012]
32. Laughon MM, Benjamin DK Jr, Capparelli EV, Kearns GL, Berezny K, Paul IM, Wade K, Barrett J, Smith PB, Cohen-Wolkowiez M. Innovative clinical trial design for pediatric therapeutics. Expert Rev Clin Pharmacol. 2011;4:643-52.
33. Wynn JL, Tan S, Gantz MG, Das A, Goldberg RN, Adams-Chapman I, Stoll BJ, Shankaran S, Walsh MC, Auten KJ, Miller NA, Sanchez PJ, Higgins RD, Cotten CM, Smith PB, Benjamin DK Jr; the NICHD Neonatal Research Network. Outcomes following Candiduria in extremely low birth weight infants. Clin Infect Dis 2012;54:331-9.
34. Watt KM, Cohen-Wolkowiez M, Ward RM, Benjamin DK Jr. Commentary. Pediatric antifungal drug development: lessons learned and recommendations for the future. Ped Inf Dis J 2012;31:635-7.
35. Testoni D, Smith PB, Benjamin DK Jr. The use of antifungal therapy in neonatal intensive care. Clinics in Perinatology, 2012;39:83-98 .
36. Kearns GL, Abdel-Rahman SM, Alander SW, Blowey DL, Leeder JS, Kauffman RE. Developmental pharmacology - drug disposition, action, and therapy in infants and children. New Engl J Med 2003;349:1157-67.
37. MacLeod S. Therapeutic drug monitoring in pediatrics: How do children differ? Ther Drug Monitoring. 2010;32:253-6.
38. Hartling L, Wittmeier KDM, Caldwell PH, van der Lee JH, Klassen TP, Craig JC, Offringa M and for the StaR Child Health group. StaR Child Health: Developing evidence-based guidance for the design, conduct, and reporting of pediatric trials. Clin Pharm Ther 2011;90:727-31.
39. Bennet G, Jessani N. The knowledge translation toolkit: Bridging the know-do gap. International Development Research Centre. Jointly published with Sage Publications, India Pvt Ltd. 2011
40. MacLeod S, Ito S. Walking the tightrope. Paediatr Child Health 2011;16:527.
Author Biography
Since 2002, Dr. Stuart MacLeod has been Vice President, Research & Academic Liaison for the BC Provincial Health Services Authority and Professor, Pediatrics, Faculty of Medicine, University of British Columbia. Previously, he spent 14 years at the University of Toronto and The Hospital for Sick Children (pharmacology, pharmacy, medicine and pediatrics) and was Dean, Faculty of Health Sciences, McMaster University 1987-1992. Research interests include pediatric clinical pharmacology, adverse drug reactions, drug policy, and global health.