Abstract
Lipid formulations, while gaining increasing importance in parenteral and oral drug delivery, are also important in transdermal and topical drug delivery. Examples and mechanisms by which lipids enhance the transport of drugs transdermally (through the skin) and topically (into the skin) will be discussed. Lipid formulations can form structures such as micelles, reverse micelles, emulsions, microemulsions, and liposomes that can aid delivery into and through the skin. A case study will be presented of a topical immunosuppressant investigated for the treatment of atopic dermatitis and psoriasis. A lipid-based polymeric ointment formulation gave superior skin uptake in vitro and in an in vivo swine efficacy model.
Lipid formulations have become increasingly important in parenteral and oral drug delivery, and are also important in transdermal and topical drug delivery. There are a number of processes by which lipids facilitate delivery of drugs into and through the skin. Lipids can form unique phase structures such as micelles, emulsions, liposomes, and similar systems that can aid delivery. This article will review these processes, as well as highlight examples of transdermal and topical products that use lipids, including a case study of a lipid formulation of a topical immunosuppressant.
Transdermal products are designed to deliver a given dose of a drug through the skin into the systemic circulation. Thus, in order to control the dose and rate of administration, these products are generally patches with a defined amount of drug and a defined area that is applied to the skin with an adhesive. Topical products are designed to deliver a drug into the skin to treat skin conditions such as atopic dermatitis and psoriasis, which generally reside in the lower regions of the skin (ie, the dermis and epidermis). Therefore, topical formulations are creams, lotions, ointments, or gels that the patient can apply to the affected areas at a relatively constant thickness. Despite these differences, the rate-limiting barrier of drug delivery for both transdermal and topical delivery is the stratum corneum, the upper layer of the skin (Figure 1). The stratum corneum is composed of proteinaceous dead cells (corneocytes), with a lipid domain between the cells; it thus can be visualized as protein “bricks” held together by lipid “mortar”; the lipids are about 78% neutral lipids and 18% sphingolipids.1
 Figure 1. Structure of the skin, with applied topical formulation and transdermal patch
Figure 1. Structure of the skin, with applied topical formulation and transdermal patchSkin permeation through the stratum corneum is governed by the permeability coefficient, Kp, of Fick’s laws of diffusion as shown in the equations below. The permeability coefficient is comprised of the drug’s effective diffusion coefficient in the stratum corneum (D), the skin vehicle partition coefficient (Ps/v), and the effective diffusion path length (h) through the skin barrier. Flux (J) is the Kp multiplied by the drug concentration (c) in the donor vehicle2:

Kp is defined as being in an aqueous vehicle. The vehicle, in fact, may contain a solvent which solubilizes the drug to a greater extent than water. If the solvent does not penetrate the skin, however, the partition coefficient Ps/v will decrease by roughly the same proportion that the concentration is increased so that there is no net change in the flux, J. If, however, the solvent does penetrate the skin, Ps/v will not decrease as much, so that there will be an increase in flux. Furthermore, such a vehicle may also increase the diffusion coefficient D, providing an additional increase in flux.3 A compound that acts in such a way to increase the flux of a drug may accurately be called a penetration enhancer. Enhancers can exert their effect by influencing either D or Ps/v, or possibly both.4 Many lipids solubilize a variety of poorly water-soluble drugs and penetrate the skin, and thus can act as penetration enhancers. A number of these interact with the lipid domains of the stratum corneum, increasing their fluidity and rendering the stratum corneum more permeable. Lipids will also act as a hydrophobic occlusive barrier to prevent water loss from the underlying skin; the resulting increased hydration of the stratum corneum leads to increased permeation.2
Lipids are classically defined as biological materials that are insoluble in water but soluble in organic solvents such as methylene chloride/methanol. This definition thus encompasses a diverse group such as fatty acids, triglycerides, phospholipids, steroids, terpenes, waxes, and even fat-soluble vitamins. An alternative definition, sometimes preferred by pharmaceutical scientists, is that lipids are fatty acids and the derivatives of those fatty acids, and substances related biosynthetically or functionally to these compounds. This definition would thus include synthetic substances such as propylene glycol fatty acid esters and ethyl laurate, as well as fatty alcohols such as cetyl alcohol (1-hexadecanol) and stearyl alcohol (1-octadecanol). Figure 2A shows the structures of some of these lipids used in topical and transdermal products.
 Figure 2. A) Structures of some lipids used in topical and transdermal formulations. B) Structures of solvents examined for topical immunosuppressant
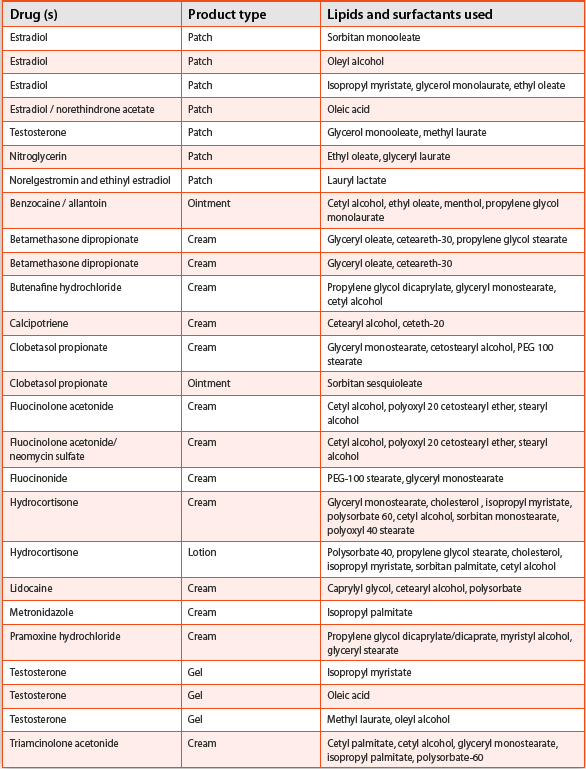
Figure 2. A) Structures of some lipids used in topical and transdermal formulations. B) Structures of solvents examined for topical immunosuppressantOleic acid (OA) has been known to be a penetration enhancer for several decades. The polar head group of OA interacts with the head groups of the stratum corneum lipids; the cis-double bond near the middle of the tail group leads to a “kink” in the chain, thus leading to increased fluidity of the stratum corneum lipids when OA intercalates with them.4 Using 2-photon scanning fluorescence microscopy, Yu et al. have shown that OA’s effects as an enhancer result from both an increase in the vehicle/skin partition coefficient and an increase in the skin diffusion coefficient.5 Fatty acids can form ion pairs with amine-containing drugs, facilitating the diffusion of this more hydrophobic species into the stratum corneum.6 While 18 carbons appear to be the optimal chain length for enhancement among unsaturated fatty acids (viz, oleic acid), 10 to 12 carbons are optimal for saturated fatty acid chains.2 Propylene glycol monolaurate (PGML) and propylene glycol monocaprate (the 10-carbon analog) are examples of enhancers in this class found in some topical and transdermal products; they are also good solvents for a variety of drugs. Glycerol monoesters (such as glycerol monolaurate, glycerol monocaprate, glycerol monocaprylate, and glycerol monooleate) are another class of enhancer lipids used topically. The 14-carbon fatty acid ester, isopropyl myristate (IPM), is found in a number of topical products and at least one transdermal patch. IPM enhances permeation primarily by increasing the fluidity of the stratum corneum lipids and reducing the diffusional resistance.7 Lipid enhancers can act synergistically with one another, as was shown with IPM and glycerol monocaprylate in permeation of pentazocine.8 Other fatty acid derivatives used in topical and transdermal products are ethyl oleate, methyl laurate, isopropyl palmitate, and oleyl alcohol. Table 1 provides a representative list of lipids used in transdermal and topical products. Some of these lipids confer desirable formulation properties on the products such as stability, viscosity, improved consistency, or spreadability, and thus may not necessarily be included to enhance drug penetration.
Table 1. Transdermal and topical products that contain lipid excipients
Another class of lipids used topically are terpenes, which are lipids built up biosynthetically from 5-carbon isoprenoid units; many of them contain ring structures and are primarily found in plant oils. Examples are menthol, limonene, and cineole (Figure 2A). They are believed to enhance penetration by increasing partitioning of drugs into the skin, extraction of skin components responsible for barrier function, and by disruption and fluidization of stratum corneum lipids.2,7,9 Menthol is a counterirritant found in many topical products to control itching; it has also been shown to enhance skin permeation. Limonene, found in lemon oil, is another example, leading to 4-fold and 26-fold enhancements in permeability for 5-fluorouracil and haloperidol, respectively, in human skin.9 One of the most potent terpene enhancers is 1,8 cineole (Figure 2A), a main component of eucalyptus oil. This compound causes up to 95-fold and 7-fold enhancements in permeability for 5-fluorouracil and haloperidol, respectively, in human skin.9 The differences in these results show that the action of these enhancers is often drug specific; the combination with a solvent such as propylene glycol can also have a large effect on the degree of enhancement. Caution must also be taken in comparing experiments with different skin type. Rodent (especially hairless mouse) skin is much more prone to enhancing effects by enhancers, particularly to terpene enhancers. Among animal skin, pig skin is generally regarded as the most representative of human skin.10 Another consideration is that large enhancements are often accompanied by an unacceptable degree of skin irritation; a 10-fold enhancement may be the conservative upper limit of enhancement before skin irritation would be a concern.
 Figure 3. Diagrams of higher-order structures formed by lipids
Figure 3. Diagrams of higher-order structures formed by lipidsAnother mechanism by which amphipathic lipids (such as phospholipids, fatty acid carboxylates, monoglycerides, and propylene glycol fatty acids) can facilitate topical and transdermal delivery is by formation of colloidal systems in the presence of water and other polar species; these include micelles, reverse micelles, emulsions, microemulsions, and liposomes (Figure 3).
Studies have demonstrated the ability of liposomes to deliver drugs such as triamcinolone acetonide locally into the epidermis and dermis.11 Possible mechanisms include penetration enhancing effects of the phospholipid components, vesicle fusion with and incorporation into stratum corneum lipid structures, and intact vesicle penetration into the stratum corneum and epidermis. It has been disputed, however, whether the latter can occur with standard liposomal preparations. More recently, “ultradeformable” liposomes containing “edge activators” such as bile salts have been indicated to have superior penetration properties compared to traditional liposomes and to promote systemic uptake of the encapsulated drugs.12 It has been proposed that a major mechanism operating for the ultradeformable liposomes is the creation of a transdermal hydration gradient which “pulls” the liposomes into skin; studies have shown these intact elastic vesicles detected well within stratum corneum.13 Similarly, ethanolic liposomes (“ethosomes”), containing phospholipids and 20% to 50% ethanol, have been shown to exhibit high deformation and skin penetration ability, and to deliver both lipophilic drugs (such as cannabinoids, testosterone, and minoxidil) as well as hydrophilic ones (eg, propranolol and trihexyphenidyl) transdermally. It is possible that a combination of mechanisms is involved in drug delivery by ultradeformable liposomes and ethosomes that depend on specific vesicle compositions and morphology, as well as on experimental conditions.11
Microemulsions are thermodynamically stable systems that form spontaneously on mixing with little or no mechanical energy applied, have droplet diameter of 6 to 80 nm, and are visually transparent or translucent.14 They are composed of an oil phase with a surfactant and a solvent or “co-surfactant,” leading to an unusually low surface tension; they have been described as “transparent water and oil dispersions” or “swollen micellar solutions.”15 Analogous to micelles and reverse micelles, microemulsions would be oil-in-water, while reverse microemulsions would be water-in-oil (ie, hydrophile in lipophile). Microemulsions have been examined in vitro and in vivo for transdermal and topical delivery of a number of drugs such as retinoic acid, diclofenac, methotrexate, cyclosporine, desmopressin, hydrocortisone, indomethacin, and ketoprofen.16,17 Possible mechanisms by which microemulsions can aid permeation of drugs include effects of penetration enhancing components; high solubilization ability that provide a high concentration gradient and high thermodynamic activity in the vehicle; hydration effects; and good wetting properties due to the low interfacial tension.16,17 As with the vesicles mentioned earlier, it is possible that a combination of mechanisms could be operating depending on the specific system.
A metronidazole microemulsion with lecithin, IPM, butanol, and water was examined for treatment of rosacea.18 Microemulsions based on IPM and/or oleic acid led to >30-fold increases in flux of estradiol across human skin relative to ethanol/buffer solutions.19
An interesting case study for use of lipids for topical delivery is delivery of a topical immunosuppressant, ABT-281 (Figure 4).20,21,22 ABT-281 (more recently named ascrolimus) is a member of the ascomycin family of macrocyclic immunosuppressants. FK-506 (tacrolimus), the most widely investigated analog of this class, is currently marketed for oral or intravenous treatment of transplant rejection, and is also marketed as a topical formulation for atopic dermatitis. However, tacrolimus can have undesirable side effects arising from systemic levels, in particular nephrotoxicity and neurotoxicity. ABT-281 has a more rapid systemic clearance in animals than tacrolimus, potentially yielding lower systemic liability than tacrolimus while still maintaining topical efficacy. The strategy for formulation development for ABT-281 was to solubilize the drug in an ointment-compatible vehicle, such that the drug is “mostly solubilized,” ie, just above saturation, with a target drug loading of 1%.
 Figure 4. Structures of the immunosuppressants ABT-281, tacrolimus, and ascomycin
Figure 4. Structures of the immunosuppressants ABT-281, tacrolimus, and ascomycinA variety of topically acceptable solvents were screened with respect to solubility of ABT-281. While the compound has low water solubility (~5 μg/mL) and LogPoctanol/water ~4, it has the highest solubility in polar organic solvents, as shown in Table 2.:
Table 2. Solubility of ABT-281 in Various Solvents

Propylene carbonate is the solubilizing agent in the tacrolimus ointment; 2 other topically acceptable solvents, dimethyl isosorbide (DMI) and ethoxydiglycol (diethylene glycol monoethyl ether), also gave high solubility values for ABT-281. Their structures are shown in Figure 2B. As would be predicted, solubility of ABT-281 in aqueous DMI and aqueous ethoxydiglycol followed a log-linear relationship; solubility in 50% cosolvent is <1 1 mg/mL. Solubility of ABT-281 in aqueous Tween 80 mixtures up to 5% Tween 80 follows a linear relationship, as expected for incorporation of drug into micelles. Up to 150 μg/mL ABT-281 can be solubilized by 5% Tween. Figure 5 shows the solubility of ABT-281 in DMI/IPM and ethoxydiglycol/IPM mixtures. These solvent systems are efficient solubilizers of the drug, and the dependence of solubility on primary solvent content (DMI or ethoxydiglycol) is more linear than log-linear; the mixtures are visually transparent. These results suggest that there are colloidal structures (reverse micellar or reverse microemulsion structures) that form between the polar primary solvents and the hydrophobic IPM, which can incorporate ABT-281 molecules.
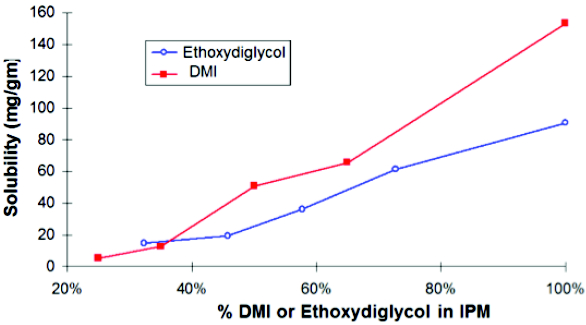
Figure 5. Solubility of ABT-281in DMI/IPM mixtures and in ethoxydiglycol/IPM mixtures
As a general approach, ointment and cream topical formulations were explored for ABT-281. For most formulations, the drug was kept in solution and close to saturation in order to maximize the driving force for drug to penetrate the skin. In some formulations, the drug was in suspension above the anticipated solubility, thereby also maximizing the driving force for drug to penetrate the skin. Acceptable prototypes were screened by: 1) physical stability and formation of drug crystals (examined by microscopy); 2) in vitro human skin penetration; and 3) in vivo swine acute contact hypersensitivity model.
The in vitro pig and human skin penetration studies were carried out in Franz diffusion cells, with [14C] ABT-281 incorporated into the formulations as a marker. The amount of drug was measured in the reservoir, stratum corneum (using tape strips), epidermis, and dermis. The in vivo swine efficacy screening involved 4- to 6-week-old domestic swine dermally sensitized to dinitrofluorobenzene (DNFB); test formulations were applied (5 mg/cm2) 30 minutes after the sensitizer challenge. Visual scores of redness and swelling are tallied by blinded observers after 24 hours.
Representative formulations examined are described below:
Petrolatum Ointments (O1): A drug solution is dispersed in petrolatum with the aid of a surfactant. Solvents examined were propylene carbonate, DMI, and ethoxydiglycol; surfactant was POE 2 stearyl ether.
Creams (C1, C2): Drug is dissolved in a semi-solid matrix of solvents and emulsifiers as an oil-in-water emulsion. Solvents were propylene carbonate, DMI, and ethoxydiglycol (aqueous phase), and PGML and glycerol caprylate/caprate (oil phase); emulsifiers were PEG-100 stearate, glyceryl monostearate, and glyceryl monolaurate.
Polymeric Ointments (P1, P2, P3): A drug solution (in DMI or ethoxydiglycol), with surfactants (glyceryl monostearate, PEG 100 stearate, or glyceryl monolaurate), was combined with copolymer (ethylene/vinyl acetate) solution in isopropyl myristate at 75°C to 90°C, homogenized and cooled.
Compositions of representative formulations and the results for the in vitro skin penetration and the in vivo swine efficacy are shown in Table 3.
Table 3. Composition and results of ABT-281 formulations

While overall in vivo/in vitro correlation was generally poor, the best overall results were from polymeric ointments, which gave good results both in vitro and in vivo. These formulations exhibited an in vivo response of 50% to 80% inhibition (drug vs. placebo) and were comparable to or higher than competitive products. For example, the percent inhibition (drug vs. placebo) values for competitive products were as follows: tacrolimus ointment, 35%; Clobetasol propionate ointment, 58%; betamethasone dipropionate ointment, 54%; fluocinonide ointment, 24%; triamcinolone acetonide ointment, 43%; and triamcinolone acetonide cream, 18%.20 Formulations P1, P2, and P3 were stable after 6 months of storage at 25°C and 40°C. These polymeric ointments were based on IPM or IPM/PGML as the primary lipid vehicle, containing a drug solution and thickened with the EVA copolymer. Figure 5 suggests that the polar drug solution is present in the lipid vehicle as a disperse phase (eg, a microemulsion). The superior performance of these polymeric ointments may be due to a combination of enhancing effects of the lipids used (IPM, PGML), and colloidal structures that aid penetration. The results support the conclusion that lipids will remain an important formulation component of transdermal and topical drug delivery.
Acknowledgments
The author wishes to thank Yeshwant Sanzgiri, John Lipari, Karl Mollison, and other colleagues from Abbott Laboratories for their work on ABT-281.
References
- Barry BW. Mode of action of action of penetration enhancers in human skin. J. Control. Release. 1987;6:85-97.
- Williams AC, Barry BW. Penetration enhancers. Adv Drug Deliv Rev. 2004;56:603-18.
- Ranade VV, Cannon JB. Transdermal Drug Delivery. In: Drug Delivery Systems. 3rd ed. Boca Raton FL: CRC Press, 2011:243-304.
- Hadgraft J. Modulation of the barrier function of skin. Skin Pharmacol. Appl. Skin Physiol. 2001;14(suppl 1):72-81.
- Yu B, Dong CY, So PT, Blankschtein D, Langer R. In vitro visualization and quantification of oleic acid induced changes in transdermaltransport using two-photon fluorescence microscopy. J Invest Dermatol. 2001;117(1):16-25.
- Stott PW, Williams AC, Barry BW. Mechanistic study into the enhanced transdermal permeation of a model b-blocker, propranolol, by fatty acids: a melting point depression effect. Int. J. Pharm. 2001;219:161-176.
- Thong HY, Zhai H, Maibach HI. Percutaneous Penetration Enhancers: An overview. Skin Pharmacol. Physiol. 2007;20:272-282.
- Furuishi T1, Fukami T, Suzuki T, Takayama K, Tomono K. Synergistic effect of isopropyl myristate and glyceryl monocaprylate on the skin permeation of pentazocine. Biol Pharm Bull. 2010;33(2):294-300.
- Sapra B, Jain S, Tiwary AK. Percutaneous permeation enhancement by terpenes: Mechanistic view. AAPS J. 2008;10:120–132.
- Godin B, Touitou E. Transdermal skin delivery: Predictions for humans from in vivo, ex vivo and animal models. Adv. Drug Deliv. Rev. 2007;59:1152–1161.
- El Maghraby GM, Williams AC, Barry BW. Can drug-bearing liposomes penetrate intact skin? J Pharm Pharmacol. 2006;58(4):415-429.
- Cevc G. Lipid vesicles and other colloids as drug carriers on the skin. Adv. Drug Deliv.Rev. 2004;56:675–711.
- Dubey V, Mishra D, Nahar M, and Jain NK. Vesicles as tools for the modulation of skin permeability. Expert Opin Drug Deliv. 2007;4:579-593.
- Water-Insoluble Drug Delivery. AustarPharma. Available at: http://www.austarpharma.com/Technologies/Channel/default_1331.shtml. Accessed September 23, 2014.
- Friberg SE, Venable RL. Microemulsions. In: Encyclopedia of Emulsion Technology, Becher P, ed. Vol. I, New York: Marcel Dekker; 1983:287.
- Santos P, Watkinson AC, Hadgraft J, Lane ME. Application of microemulsions in dermal and transdermal drug delivery. Skin Pharmacol Physiol. 2008;21(5):246-259.
- Date, AA, Patravale VB. Microemulsions: Applications in transdermal and dermal delivery. Crit. Rev Thera. Drug Carrier Systems. 2007;24(6):547-596.
- Tirnaksiz F, Kayiş A, Çelebi N, Adişen E, Erel A. Preparation and Evaluation of Topical Microemulsion System Containing Metronidazole for Remission in Rosacea. Chem. Pharm. Bull. 2012;50(5):583-592.
- Peltola S, Saarinen-Savolainen P, Kiesvaara J, Suhone TM, Urtti A. Microemulsions for topical delivery of estradiol. Int. J. Pharm. 2003;254:99-107.
- Mollison KW, Fey TA, Gauvin DM, et al. A macrolactam inhibitor of T helper type 1 and T helper type 2 cytokine biosynthesis for topical treament of inflammatory skin diseases. J Invest Dermatol. 1999;112:729-738.
- Cannon JB, Hansrani P, Hertzler TL, Lipari J, Sanzgiri YD, Wittenberger SJ. Polymorph of a Pharmaceutical. US Patent application 2003/0199537; 2003.
- Sanzgiri YD, Cannon J, Hansrani P, et al. Topical formulations for ABT-281, an immunosuppressant. Poster at 1999 AAPS Annual Meeting and Exposition, November 14– 18, 1999, New Orleans. Available at: http://abstracts.aaps.org/published/ContentInfo. aspx?conID=38903.