Abstract
Biotechnology drug substances are often stored frozen. This approach has several advantages but is also expensive and time consuming. In the development of freeze-thaw processes for protein based products, we sought to develop a framework according to the principles of Quality by Design (QbD). This approach, as well as a mature understanding of the risks and benefits associated with the freezing of drug substances, allows design of a robust strategy that can be utilized on a wide variety of compounds and freeze-thaw configurations. This article, the first of two parts, describes the costs and benefits of freeze-thaw processes and provides the outline of a QbD approach to freeze-thaw in bottles. A subsequent article will describe a QbD approach to actively controlled freeze-thaw processes.
Introduction
Proteins have been frozen since the early days of biotechnology. Often, freezing was selected due to a lack of stability of a protein in solution, but also because it was perceived as a convenient manner to store proteins from days to years. With the advent of large scale production of proteins, novel approaches to the freezing and storage of proteins have evolved in which the freeze-thaw process is better controlled and frozen volumes have increased from several hundred milliliters to 300 liters. With greater control of these processes comes the opportunity to develop robust, validated freeze-thaw cycles that yield a consistent drug substance (DS) or drug substance intermediate (DSI), suitable for further processing.
Recent guidance from the regulatory agencies [1-3] and discussions with various industry groups [4] have resulted in a concerted effort to define and implement elements of a Quality by Design (QbD) paradigm to process and product development. QbD represents a systematic approach to development that begins with predefined objectives which establish the target product for the patient, and emphasizes product and process understanding and control based on good science as well as sound quality risk management.
Benefits, Costs and Risks Associated with Freezing Protein Containing Solutions
Protein based drug substances can be stored under a variety of conditions. While refrigerated liquids have been utilized, and spray dried powders have been explored for certain applications [5], a very substantial number of clinical and commercial drug substances are stored in a frozen state. Frozen drug substances have considerable benefits but also have costs and risks associated with them.
Drug substance storage is generally considered a conservative approach that reduces risk on stability. For clinical drug substances the initial expiry period for a batch of DS may only be 6 to 12 months. However, with a well designed formulation and a suitable stability program, this batch of DS can potentially have its expiry period extended through the life of the initial clinical trials, therefore avoiding the need for additional drug substance manufacturing. Further, with the development of high concentration monoclonal antibodies for clinical and commercial application [6], there is a growing trend to develop high concentration drug substances to provide higher doses, reduced storage volume and enable storage at a more convenient -20°C due to the increased level of amorphous solids.
One can utilize frozen bottles of drug substance to provide manufacturing flexibility when compounding a batch of drug product. Having the flexibility to select different bottles of frozen DS aids in managing batch size as well as flexibility at the fill site. This is also true for drug substances which are utilized to manufacture a variety of dosage strengths, such as clotting factors and cytokines. The ability to thaw and compound multiple bottles and batches helps to reduce wastage as well as ensure that the DS meets the appropriate specifications throughout its shelf-life.
A final advantage of frozen drug substances is that the frozen state can arrest microbial growth, especially in comparison to refrigerated drug substances. While many firms are diligent to ensure a low bioburden environment during the bottling or transfer of DS to the storage vessel, in the absence of sterility testing we cannot claim to produce sterile drug substances. While this is a risk for refrigerated drug substances, it is less of a concern for frozen DS.
There are two general types of risk for proteins associated with the freezing of larger volumes of solution: fundamental risks associated with the freezing process itself under ideal conditions and risks associated with heterogeneous freezing processes.
Denaturation of proteins that undergo freezing [7,8], has been extensively studied with lactate dehydrogenase, alcohol dehydrogenase, catalase [9,10] and interleukin 11 [11].Heterogeneous freezing contributed to the precipitation of fibroblast growth factor 20 [12]. Aggregation has been reported for several proteins as they undergo freeze-thaw. Typically, these modifications to the protein are associated with heterogeneity of the solution. For example, a Fc-fusion protein demonstrated increased levels of aggregation due to the crystallization of sorbitol in the frozen solution [13]. In addition, a monoclonal antibody was reported to also aggregate during freeze and thaw due the crystallization of mannitol [14]. Finally, the unfolding of proteins has been studied by tryptophan fluorescence analysis of proteins in which the authors argue that denaturation is due to the ice-liquid interface [15-17]. These types of denaturation events have been managed by a variety of methods including the addition of various formulation excipients. The addition of cryoprotectants such as glycerol or sucrose has demonstrated a reduced level of denaturation [15]. Finally, as with the addition of cryo-preservatives, simply increasing the protein concentration to 100 mg/mL, thus reducing the level of excipient crystallization, can have a substantial benefit with regard to reduced levels of aggregation [18]. Heterogeneous freezing rates result in substantial changes in the composition of the frozen solution. This cryo-concentration event has been well characterized in a variety of freeze-thaw systems including small containers, 2-liter bottles and cryo-vessels. Upon freezing, select buffers such as sodium phosphate can precipitate from solution, resulting in substantial pH changes to the solution [19-21]. These pH changes can have deleterious effects on protein solubility [14] as well as protein conformation [13]. Metal catalyzed degradation of proteins has been reported in the literature and may be caused by leaching of various transition metals such as iron(II) and iron(III) into solution [22]. In a well designed, scaled-down study of cryo-vessels, protein concentration at the last point to freeze was increased from approximately 20 mg/mL to up to 48 mg/mL, a 2.5x increase [23]. Similarly, osmolality increased from a target of 256 mOsm/Kg to 889 mOsm/Kg in protein containing solutions. While difficult to manage in these large freeze-thaw systems, one must be aware of the potential solution heterogeneity that exists within the frozen state.
There are three types of container closure system typically utilized for frozen drug substances: plastic or stainless steel bottles between 1-5 L, plastic bags between 1-16 L and stainless steel cryo-vessels between 125 - 300 L. In our experience, we have utilized Teflon or stainless steel bottles routinely for frozen drug substances at temperatures from -80°C to -20°C. While the individual bottles can be expensive (several hundred dollars per bottle), they are relatively inexpensive when compared to the cost of a cryo-vessel. A more cost effective option is PETG bottles but these bottles have a brittleness temperature of -40°C in contrast to PFA Teflon with a brittleness temperature of -270°C [24]. One other consideration when using plastic bottles is their permeability to carbon dioxide when shipped on dry ice which can result in pH shifts upon shipping [25]. Small bottles do not have substantial costs associated with freezing processes; often the bottles are frozen in a bath of dry ice/ethanol or liquid nitrogen. While these are not too expensive, care should be taken to ensure a safe workplace when dealing with large volumes of these liquids as well as the risk of reduced breathable air in the vicinity of the freezing tank. Frozen storage is often achieved by the use of freezers from -80°C to -40°C or walk-in freezer rooms for -20°C. Again, while not inexpensive, this type of equipment has been utilized for 20+ years and has a robust history within the biotechnology industry. Equipment and facility costs associated with large volume storage will be discussed in a subsequent article.
There are certain elements of risk that all freeze-thaw processes share, notably heterogeneity of the freezing process, process validation (including installation, operation and process qualifications), storage costs (stand alone freezers and walk-in freezers that must be suitably qualified, maintained and alarmed) as well as shipping. One aspect that requires particular attention from a QbD perspective is freezing rate.
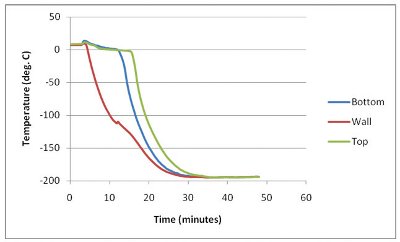
Figure 1- Heterogeneity of Freeze in a 1-L Bottle. A buffer containing 1-L Teflon bottle was frozen in liquid nitrogen. Temperature was recorded at different locations within the bottle. The wall (red) froze most quickly followed by the bottom (blue) and the top (green).
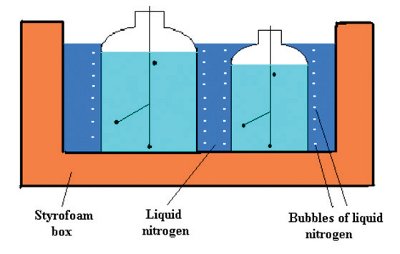
Figure 2- Freeze-thaw Profiles for Teflon Bottles: Position of Thermocouples in Bottles and Bottles in a Styrofoam box.
Figure 1 presents the heterogeneous freezing rates associated with a 1-liter Teflon bottle. Freezing a 1-liter Teflon bottle was performed by immersing the bottle up to its shoulder in liquid nitrogen (see Figure 2). The data presented in Figure 1 demonstrate that the rate of temperature decrease is quite variable depending on the position of the thermocouple. The thermocouples placed at the top/center of the solution demonstrate a substantially slower rate of freeze than those near the wall of the bottle. The top/center is typically referred to as the last-point-to-freeze (LPF). Ensuring that the contents of the bottle are properly frozen is important not only from a stability perspective but also when the bottles are transferred to a -80 °C freezer. Very often, the addition of several 1-5 liter frozen bottles, frozen in the manner described above, will cause the temperature in the freezer to decrease and go out of its normal operating range (typically -70 °C to -90 °C), resulting in an alarm. This heterogeneity in freezing rates must be recognized and accommodated when understanding the freezing and thawing processes within any freezing apparatus or container.
Quality-by-Design
Between 2000 and 2005, there was considerable discussion between regulatory agencies such as FDA and industry regarding the state of process development and understanding, and the tremendous number of process improvements that were being proposed to the regulatory authorities. This overall burden, coupled with the significant increase in applications for novel molecular entities, innovative processes and dosage forms, resulted in an initiative to better define the relationship between process design and understanding with process control, risk management and continuous improvement. These discussions resulted in two important ICH guidelines being published: Q8 Pharmaceutical Development and Q9 Quality Risk Management. These documents, which describe the regulatory expectations for the pharmaceutical development section of a Common Technical Document (CTD) and approaches for the development of suitable science driven risk management approaches, respectively, in combination with Q10 Quality Systems Approach to Pharmaceutical cGMP Regulations, resulted in the Quality by Design initiative.
ICH Q10 provides a model for a pharmaceutical quality system that evolves as a product moves from early stage (phase 1) development through late stage clinical development, commercialization and lifecycle management. By the use of this guideline, firms should be able to logically develop and implement innovative technologies and process improvements while continuing to utilize existing process characterization and understanding from the original process. This approach of continuous improvement is intended to be encouraged, thus increasing quality and or availability of pharmaceutical products, and implementation should be managed in a manner that provides openness and transparency linking the proposed process to the earlier stage processes. These improvements should be based, of course, on suitable science, risk based decisions and quality systems which are outlined in ICH Q10.

Figure 3- QbD Flow Diagram
QbD represents a scientific, risk-based, holistic and practical approach to pharmaceutical development . It provides a logical framework (Figure 3) in which the desired outcome (the quality target product profile (QTPP)) is defined early in the life cycle of the product. The QTPP is an ideal summary of the quality characteristics of the drug product. The QTPP drives process development (how one achieves the QTPP), the definition of the critical quality attributes (CQA – the characteristics of the product that must be achieved in order to satisfy the QTPP), and identification of the critical process parameters (CPP) which must be defined and controlled in order to achieve the CQAs. This logical flow is further expanded to include a timely and robust risk assessment process, similar to that used in the device industry for many years, as well as a greater and deeper understanding of process design space.
Case study - Frozen Bottles
This case study provides guidance pertaining to the freeze and thaw of protein containing solutions in Teflon bottles. This design approach can be applied to any type of bottle or container and should be scaled appropriately. Further, many of the QbD elements described for bottles are similar to those for a controlled freeze-thaw process using programmed systems for disposable bags or large stainless steel containers (addressed in a subsequent article). This and the coming two examples, therefore, are interdependent in their use of QbD.

Figure 4- Decision Tree for Freeze-Thaw Processes
The pharmaceutical scientist must first establish the appropriate volume and container closure that is to be utilized for the frozen drug substance. One could follow the guidance described in Figure 4. For bottles, one must determine whether the protein containing solution can withstand the quick freezing conditions associated with liquid nitrogen or an ethanol/dry ice bath. This data may come from small scale freeze-thaw experiments performed during pre-formulation of a compound or during the early stages of formulation and process development. In addition, one should perform DSC analysis of the samples to ensure characterization of the critical freezing points that help to establish the appropriate storage temperature. If, for example, the drug substance is to be stored at -80˚C, then the bottles should be frozen to that target temperature prior to transfer to the freezer. This will reduce the strain on the freezer and minimize temperature alarms that will occur upon transfer.

Figure 5- Fishbone diagram for a standard freeze-thaw process (Bottles)
Table 1- Potential Critical Quality Attributes for Consideration in Process Risk Assessment

Table 2- Suggested Studies for Frozen Drug Substance in Bottles

Once the QTPP has been developed, prior knowledge has been assessed and CQAs (Table 1) have been defined, process development must be planned and executed. Often the process of identifying CQAs is concurrent with development studies leading to cycles of risk assessment and a clearer definition of CQAs. Table 2 provides a list of suggested studies that could be performed as part of process development of the freeze-thaw step. These studies are intended to be a comprehensive set of experiments that address not only the specific unit operations of the freeze-storage-thaw process, but also provide suitable guidance pertaining to design space. The list of suggested studies could also take into account a thorough process description that can be constructed using an Ishikawa diagram (Figure 5). For example, in assessing the freeze-thaw profile, one should first establish the range of rates of freeze and thaw that can be achieved in 1-L and 3-L bottles. For the purpose of robustness and process definition, one could express the data in terms of freeze or thaw times as presented in Table 3. Obtaining these rates of freeze, and establishing time to freeze, allows one the ability to determine when freezing is complete and therefore when the bottles are appropriate to remove from the liquid nitrogen container and place into the freezer. Also, they define conditions by which small scale multiple freeze-thaws should be conducted. The Ishikawa diagram, in conjunction with a suitable process understanding based on experimental data (Table 2), allows one to perform an appropriate risk assessment.
Table 3- Freeze and Thaw Times for 3-L Bottles

A failure modes, effects and criticality analysis (FMECA) may be an appropriate tool for risk assessment; this will be discussed in a subsequent article. This risk assessment, in conjunction with the process understanding and CQAs, permits one to develop a comprehensive process control strategy. One must also have a deliberate strategy to define the in-process limits in terms of normal operating range compared to proven acceptable ranges. For example, cumulative hold time as unfrozen drug substance may allow 2 weeks at 2-8°C. There must be thoughtful consideration regarding how these 2 weeks should be distributed across the different unit operations (filtration, sampling and freezing, thawing, QC analyses and so on.) This strategy includes identification of potential critical process parameters as presented in Table 4. The CPP table provides a list of process inputs or set-points as well as specific in-process control ranges which are based on the data collected during process development as well as facility and operational limitations.
Table 4- Potential Critical Process Parameters – Frozen Bottles

Summary
Freezing, storage and thawing of protein based drug substances has been utilized for several decades in the biotechnology industry. While the technology for these processes has evolved from frozen bottles to cryo-vessels to cryo-bags, there is still a need for all three systems depending on the nature of the drug substance, batch volume and storage temperature. As such, all three configurations are viable for many years to come. Recent developments with the regulatory agencies pertaining to quality by design have suggested that a more disciplined and deliberate approach to process and product development is required throughout the lifecycle of a product.
References
- ICH Harmonized Tripartate Guideline: Pharmaceutical Development (ICH Q8); Current Step 4 Version dated November 10, 2005.
- ICH Harmonized Tripartate Guideline: Quality Risk Management (ICH Q9); Current Step 4 Version dated November 9, 2005.
- ICH Harmonized Tripartate Guideline: Pharmaceutical Quality System (ICH Q10); Current Step 4 Version dated June 4, 2008. 4
- A-Mab: a Case Study in Bioprocess Development; CMC Biotech Working Group (Version 2.1; 30 October 2009) available online at www.casss.org
- H Todo, H Okamoto, K Iida, K Danjo; Improvement of stability and adsorbability of dry insulin powder for inhalation by powder-combination technique (2004). International Journal of Pharmaceutics, 271, 41-52 6
- SJ Shire, J Liu, W Friess, S Jörg, H-C Mahler; High Concentration Antibody Formulations (2010) in Formulation and Process Development Strategies for Manufacturing Biopharmaceuticals, Jameel and Hershenson editors, John Wiley and Sons publishers
- PL Privalov; Cold Denaturation of Proteins (1990) Biochemistry and Molecular Biology 25, 281-305
- WJ Becktel, JA Shellman; Protein Stability Curves (1987) Biopolymers 26, 1859-1877
- E. Cao, Y. Chen, Z. Cui, PR Foster; Effect of Freezing and Thawing rates on denaturation of Proteins in Aqueous Solutions (2003) Biotechnology and Bioengineering 82:684-690
- K Shikama, I Yamazaki; Denaturation of Catalase by Freezing and Thawing (1961) Nature 190:83-84
- N. Warne and R. Koval; Freeze-Thaw of rhIL-11;1998 Conference on Protein Stability, Breckenridge, CO, July 1998
- H. Maity, C. Karkaria, J. Davagnino; Mapping of solution components, pH changes, protein stability and the elimination of protein precipitation during freeze-thawing of fibroblast growth factor 20; (2009) International Journal of Pharmaceutics 378, 122-135
- DM Piedmonte, C Summers, A McAuley, L. Karamujic, G Ratnaswamy; Sorbitol Crystallization can lead to Protein Aggregation in Frozen Protein Solutions (2007) Pharmaceutical Research 24, 136-146 1
- K. Ho, D. Luisi, D. Sek, A. Kantor and N. Warne; Characterization of Cryo Freeze and Thaw of a Monoclonal Antibody Solution in Stainless Steel: Effect of Process Scale and Excipient Level; AAPS National Meeting, Nashville, Nov. 2005
- GB Strambini, E Gabellieri; Proteins in frozen solutions: evidence of ice-induced partial unfolding (1996) Biophysical Journal 70, 971-976
- A Hillgren, J Lindgren, M Alden; Protection mechanism of Tween 80 during freeze-thawing of a model protein, LDH (2002) International Journal of Pharmaceutics 237, 57-69.
- L Bush and C Webb; Formulations for Factor IX. United States patent 6372716
- A Kantor; Frozen Biologic Drug Substance: You Freeze It, You Thaw It, What Could Go Wrong AAPS Annual Meeting and Exposition, 14-18 November 2010
- N Muase, F Franks; Salt precipitation during the freeze-concentration of phosphate buffer solutions (1989) Biophys Chem 34, 293-230
- Y Orii, M Morita; Measurement of the pH of frozen buffer solutions by using pH indicators (1977) J Biochem 81, 163-168
- L Van den Berg, D Rose; Effect of freezing on the pH and composition of sodium and potassium phosphate solutions: the reciprocal system KH2PO4-Na2HPO4-H2O (1959) Arch Biochem Biophys 81, 319-329
- S Zhao, B Zhang, E Sturm, DL Teagarden, C Schoneich, P Kolhe, LM Lewis, BK Muralidhara, SK Singh; Comparative Evaluation of Disodium Edetate and Diethylenetriaminepentaacetic Acid as Iron Chelators to Prevent Metal-catalyzed Destabilization of a Therapeutic Monoclonal Antibody (2010) Journal of Pharmaceutical Research 99, 4239-4250.
- P. Kolhe, E. Holding, A. Lary, S. Chico, S. Singh; Large-Scale Freezing of Biologics: Understanding Protein and Solute Concentration Changes in a Cryovessel – part 1; (2010) BioPharm International, June 1, 2010 2
- Temperature ratings on Nalgene® products and other information; U.S. Plastic Corporation, Article 876, 03 June 2010
- J Zerfas, T Bowie, M Kreuze, C Webb; Study of Impact of Carbon Dioxide Incursion on pH of Bulk Drug Substance and Buffer Solutions, AAPS Biotech, Boston, June 2006
- AS Rathore, H Winkle; Quality by design for biopharmaceuticals (2009) Nature Biotechnology 27, 26-34
Author Biographies
Dr. Warne is the Senior Director of the Pharmaceutics R&D Group at Pfizer BioTherapeutics R&D in Andover, Massachusetts. Nick has been at Pfizer, formerly Wyeth BioPharma and Genetics Institute, for 20 years and has focused on protein stabilization, formulation development and drug product process development. Nick holds numerous protein formulation patents and, with his group, has made over 100 presentations at national meetings and in journals.
Dr. Serguei Tchessalov is a Senior Principle Scientist at Pfizer Pharmaceutics R&D (Andover, MA). He received his Ph.D. from Institute of Applied Biochemistry (Moscow) on development of novel methods for formulation and process control during lyophilization. For the past 20 years (in Russia and US) he has wored on formulation and lyophilization process development of bacterial and viral vaccines, proteins and different biological materials. His current research is focused on lyophilization process scale up as well as processing of parenteral dosage forms (filtration, filling, freezing/thawing).
Angela Kantor is a Senior Principal Scientist in the Pharmaceutics R&D Group at Pfizer in Andover, MA. Ms. Kantor leads a group focused on the development of dosage forms for therapeutic proteins. Her responsibilities include formulation, drug substance storage, drug product process development and technology transfer for projects in all phases of development. Ms. Kantor’s projects have included both lyophilized and liquid dosage forms for high concentration proteins. Her interests also include implementation of Quality by Design for drug product. She has been at Pfizer (formerly Wyeth) last thirteen years.
This article was printed in the May/June 2011 issue of American Pharmaceutical Review - Volume 14, Issue 4. Copyright rests with the publisher. For more information about American Pharmaceutical Review and to read similar articles, visit www.americanpharmaceuticalreview.com and subscribe for free.