Bryan Thacker - Senior Scientist - TEGA Therapeutics
Charles Glass - President and CSO - TEGA Therapeutics
Susan Sharfstein - Professor - SUNY Polytechnic Institute
Heparin – An Essential Anticoagulant
Heparin is a potent anticoagulant that has been used clinically to manage blood clotting since 1935. Hundreds of thousands of doses are administered daily in the U.S. during surgery and for patients at risk of venous thromboembolism. Medical devices that come in contact with blood, such as dialysis tubing, are also coated with heparin. The importance of heparin is underscored by its inclusion on the World Health Organization’s list of essential medicines and a worldwide market of over $7B annually.
The world’s supply of crude heparin is derived predominantly from porcine intestinal mucosa, a tissue containing heparin-producing mast cells, as a byproduct of pork production. By virtue of having the world’s largest pig population, the bulk of the world’s crude heparin is produced in China. Pharmaceutical heparin is manufactured from crude extracts through downstream processing by several pharmaceutical companies. Production of an essential medicine from an animal population located predominantly in a single country places the world’s heparin supply at risk. In 2007, a widespread outbreak of blue ear disease among pig herds in China led to a global shortage of heparin. Subsequent adulteration of the heparin supply with over-sulfated chondroitin sulfate resulted in more than 250 deaths worldwide.1 Regulatory standards have since been improved to eliminate adulteration2 yet there is still concern as to whether an animal population can meet the world’s growing heparin demand, especially in light of an ongoing African swine fever that at one point, reduced the pig population in China by nearly one-third. Other anticoagulants including warfarin and new oral anticoagulants provide alternatives to heparin, yet heparin’s short half-life and fast reversibility make it the drug of choice during surgery. Additionally oral anticoagulants have largely been deemed inappropriate for pregnant women and for patients with prosthetic heart valves, renal impairment and severe liver disease.
Recombinant Biotherapeutics
While there is a long history of producing medicines from animal tissues, the advent of recombinant production technologies in the 1980s has largely eliminated animal-derived products from the pharmacy/ Insulin serves as a prime example of the success of recombinant protein therapeutics. The efficacy of insulin was first demonstrated in 1922 and insulin derived from porcine and bovine tissue was used for 60 years and saved millions of lives. Yet demand outpaced availability and concerns persisted over administration of non-human insulin to patients. Chemical modification of animal-derived insulin yielded “semisynthetic human insulin”; however challenges with purity and consistent quality remained.3 Recombinant DNA technology enabled the production of human insulin, introduced in 1982, as one of the world’s first recombinant protein products used in the clinic. Recombinant production ensured a reliable, affordable and abundant source of human insulin with improved purity and batch-to-batch consistency over animal-derived products. Recombinant human insulin remains the standard of care for diabetic patients today.
Since the 1980s, dozens of recombinant protein therapeutics have been approved for clinical use. Various mammalian cells have been used for production with Chinese hamster ovary (CHO) cells emerging as the most commonly used cell type. Over the past four decades, cell lines, media formulations and culture methods have been optimized to increase protein production efficiency, which now yields grams of protein per liter of culture volume in optimized systems. These tremendous advances in recombinant protein production have yet to be translated to production of therapeutic polysaccharides from cell culture.
Advancing to Recombinant Heparin
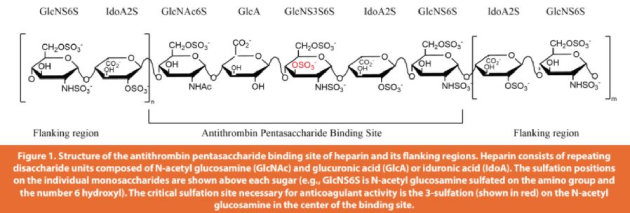
Heparin is a highly sulfated form of heparan sulfate. Heparan sulfate is a linear polysaccharide produced by all mammalian cells. Heparin and heparan sulfate are sulfated at various positions along the polysaccharide chains, forming specific protein binding sites and giving the chains their functional properties (Figure 1). Heparin is distinguished by its exclusive biosynthesis in mast cells, its high sulfate content and its potent anticoagulant activity, which is almost entirely absent in heparan sulfate. The abundance and specific positions of sulfate groups are responsible for heparin’s high anticoagulant potency.
In contrast to proteins, which are the products of single genes, heparan sulfate production is non-template driven. Rather, it is the product of a biosynthetic pathway involving more than 20 enzymes. The abundance and pattern of sulfation is determined by the expression levels of the enzymes in the biosynthetic pathway. Cell-type and tissue-specific functions result from sulfation patterns. Likewise, the chemical and biological properties of heparan sulfate in cultured cells can be manipulated by modulating the expression of biosynthetic enzymes genetically and through the cell culture conditions.
Since CHO cells have been the predominant choice for production of recombinant biotherapeutics, it is appealing to use this cell line for production of recombinant heparin. Previous work has focused on engineering the heparan sulfate biosynthetic pathway of CHO cells to produce heparin.4 Structural analyses showed that CHO cell heparan sulfate was under sulfated compared to porcine-derived heparin and lacked sulfate groups in positions that are critical for anticoagulant activity. Gene expression analyses revealed two enzymes in mast cells that were lacking in CHO cells. Subsequent overexpression of these two enzymes in CHO cells increased sulfate content but failed to recapitulate the degree of sulfation and the sulfation patterns found in heparin. Accordingly, the anticoagulant activity of engineered CHO heparan sulfate was increased over the starting cell lines but was still about 50-fold lower than the activity of porcine-derived heparin. Nonetheless, these results demonstrated the feasibility of manipulating the biosynthetic pathway to alter the composition and therefore the anticoagulant activity of heparan sulfate. Similarly, heparan sulfate from other cell lines used for research and production of biotherapeutics such as HEK293, NS0 and HeLa cells have low sulfate content.
Mast cells are the natural source of heparin, but they are not readily cultured in vitro; however, mastocytomas arise naturally in humans and other species. Stable cell lines have been isolated from murine mastocytomas and readily grow in cell culture. These cell lines are promising candidates for production of recombinant heparin because of their lineage. As such, mastocytoma cell lines produce heparan sulfate with sulfate content similar to heparin. Still, mastocytoma heparan sulfate lacks potent anticoagulant activity due to an absence of sulfation at a key position on the polysaccharide.5
Subsequent research showed that mastocytoma cells do not express a key enzyme required for production of anticoagulant potency. Overexpression of the missing enzyme resulted in heparan sulfate with substantially higher anticoagulant activity, however still about three-fold lower activity than pharmaceutical heparin.6 Through additional genetic engineering and bioprocess development, we have recently increased the anticoagulant activity of heparan sulfate derived from mastocytoma cells to equal that of porcine-derived heparin, demonstrating the feasibility of producing recombinant heparin.
Production of heparin from a recombinant cell line provides several enticing advantages. For one, the supply of heparin would no longer be coupled to the health and abundance of an animal population. It also enables production to be carried out in bioprocessing facilities located in various locations around the world, rather than being predominantly tied to a single country. Furthermore, recombinant heparin will be free from contamination and variability inherent in production from animal tissues and production can be performed under GMP conditions from start to finish. Finally, production in a genetically modified cell line raises the possibility of engineering the quality of the product, for instance, through reduction of side effects like heparin-induced thrombocytopenia.
Remaining Challenges for Recombinant Heparin
As a novel cell line for production of a biotherapeutic, there are a number of challenges to overcome to produce recombinant heparin from mastocytoma cells. Work is currently underway to understand how these cells behave in bioreactors and in chemically defined media. Additionally, purification may be complicated by the fact that mastocytoma cells store a portion of their heparan sulfate in intracellular granules. Mammalian cells also produce other polyanionic products such as DNA and chondroitin sulfate that co-purify with heparan sulfate. Development of recombinant heparin from mammalian cells benefits from bioprocessing technologies that have been developed over the past 40 years, although these resources have been developed with protein production in mind. Some knowledge, like optimal media/feed formulation and purification methods, may need to be reconsidered for optimization of polysaccharide production. Work is ongoing to address these concerns.
Technical issues aside, the biggest challenge to adoption of recombinant heparin may be economic. Crude porcine-derived heparin is sourced from pork production byproducts, which coupled with the low cost of labor in China, makes for relatively inexpensive heparin. (~$25/g) Increasing efficiency through optimizing productivity, streamlining production and increasing scale will be critical for recombinant heparin to be economically competitive. Initially, recombinant heparin may be targeted to niche applications where higher quality is needed and justifies a higher price. Cardiopulmonary bypass for patients at risk of heparin-induced thrombocytopenia is an example where recombinant heparin might be introduced.
Non-Anticoagulant Applications
Endogenous heparan sulfate interacts with hundreds of binding proteins including growth factors, cytokines, enzymes and extracellular matrix proteins, and heparan sulfate has various biological effects depending on the system. For example, heparan sulfate facilitates cell surface signaling, establishes protein concentration gradients, protects proteins from proteolysis or clearance, facilitates endocytosis and inhibits enzyme activity. Thus, production of recombinant heparan sulfates from engineered cell lines raises compelling non-anticoagulant therapeutic possibilities. A review of clinical trials conducted on hepari or heparin-like products underscores the therapeutic possibilities.7 Non-anticoagulant interventions with heparin that have been investigated clinically include conditions such as cancer, pulmonary failure, infertility, metabolic disorders and sepsis.8 In these applications, anticoagulation may be an unwanted side effect. Chemical modification of porcine-derived heparin has been used to eliminate anticoagulant activity, but these treatments have non-specific effects on the other chemical features of the polysaccharide that may limit the therapeutic use. On the other hand, targeted deletions through genetic engineering can remove certain sulfate groups to render the heparan sulfate non-anticoagulant while leaving the other features of the polysaccharide unchanged. Our investigations are currently underway to determine the effect that non-anticoagulant recombinant heparan sulfates may have in areas involving inflammation, emphysema, regenerative medicine and anemia.
Conclusion
Heparin is an essential medication that has been used by millions around the world for more than 80 years yet its supply depends on an animal population leaving it at risk of shortage or contamination. Recombinant DNA technologies have enabled the biopharmaceutical industry to produce protein therapeutics from cultured cells, but to date no polysaccharides have been developed for clinical use from recombinant mammalian cell lines. We have shown that genetic engineering of mammalian cell lines provides a method to produce recombinant heparin with high anticoagulant potency as an alternative to porcine-derived heparin. It also raises the possibility of improving the quality of recombinant heparin or developing non-anticoagulant heparan sulfates for other clinical applications.
Author Biographies
Bryan Thacker is a Senior Scientist at TEGA Therapeutics developing cell lines, bioprocessing methods and anticoagulant/non-anticoagulant applications for recombinant heparan sulfates. Bryan holds a Ph.D. in Biomedical Sciences from UC San Diego. Charles Glass is the CSO at TEGA Therapeutics overseeing multiple areas of proteoglycan research. Charles holds a Ph.D. in Zoology from UC Berkeley.
Susan Sharfstein is a Professor of Nanobioscience at SUNY Polytechnic Institute in Albany, New York. Her research focuses on the use of mammalian cell cultures for production of therapeutic proteins and carbohydrates, regenerative medicine and drug screening applications. She received her Ph.D. in Chemical Engineering from UC Berkeley.
Literature Cited
- Guerrini, M., Beccati, D., Shriver, Z., Naggi, A., Viswanathan, K., Bisio, A., Capila, I., Lansing, J. C., Guglieri, S., Fraser, B., Al-Hakim, A., Gunay, N. S., Zhang, Z., Robinson, L., Buhse, L., Nasr, M., Woodcock, J., Langer, R., Venkataraman, G., Linhardt, R. J., Casu, B., Torri, G., and Sasisekharan, R. (2008) Oversulfated chondroitin sulfate is a contaminant in heparin associated with adverse clinical events. Nat Biotechnol 26, 669-675
- Szajek, A. Y., Chess, E., Johansen, K., Gratzl, G., Gray, E., Keire, D., Linhardt, R. J., Liu, J., Morris, T., Mulloy, B., Nasr, M., Shriver, Z., Torralba, P., Viskov, C., Williams, R., Woodcock, J., Workman, W., and Al-Hakim, A. (2016) The US regulatory and pharmacopeia response to the global heparin contamination crisis. Nat Biotechnol 34, 625-630
- Landgraf, W., and Sandow, J. (2016) Recombinant Human Insulins - Clinical Efficacy and Safety in Diabetes Therapy. Eur Endocrinol 12, 12-17
- Baik, J. Y., Gasimli, L., Yang, B., Datta, P., Zhang, F., Glass, C. A., Esko, J. D., Linhardt, R. J., and Sharfstein, S. T. (2012) Metabolic engineering of Chinese hamster ovary cells: towards a bioengineered heparin. Metab Eng 14, 81-90
- Montgomery, R. I., Lidholt, K., Flay, N. W., Liang, J., Vertel, B., Lindahl, U., and Esko, J. D. (1992) Stable heparin-producing cell lines derived from the Furth murine mastocytoma. Proc Natl Acad Sci U S A 89, 11327-11331
- Gasimli, L., Glass, C. A., Datta, P., Yang, B., Li, G., Gemmill, T. R., Baik, J. Y., Sharfstein, S. T., Esko, J. D., and Linhardt, R. J. (2014) Bioengineering murine mastocytoma cells to produce anticoagulant heparin. Glycobiology 24, 272-280
- Hao, C., Xu, H., Yu, L., and Zhang, L. (2019) Heparin: An essential drug for modern medicine. Prog Mol Biol Transl Sci 163, 1-19
- Oduah, E. I., Linhardt, R. J., and Sharfstein, S. T. (2016) Heparin: Past, Present, and Future. Pharmaceuticals (Basel)
Subscribe to our e-Newsletters
Stay up to date with the latest news, articles, and events. Plus, get special offers
from American Pharmaceutical Review – all delivered right to your inbox! Sign up now!