Emilie Gauthy - Senior Manager Development & Validation, Celyad Oncology
Hannes Iserentant - Senior Director R&D and IP/European Patent Attorney, Celyad Oncology
A Decade of CAR T cells
Over the past twelve years, immunotherapy has become an important treatment option for patients in the fight against cancer. One specialized approach within the field of cancer immunotherapy harnesses the power of T cells combined with selected Chimeric Antigen Receptors (CAR) to create efficient adoptive cell therapies. CAR T cells have dramatically changed the therapeutic options for select cancers – mostly hematological ones1- 4 (such as acute lymphoblastic leukemia, B-cell lymphoma, follicular lymphoma, mantle cell lymphoma and multiple myeloma), including remarkable durable remissions for more than 10 years post treatment.5 Nevertheless, challenges remain for these cell therapies when treating a wider spectrum of patients, particularly for the treatment of solid tumors.
Evolving CAR T Landscape Towards Off-the-Shelf Approaches
Initial CAR T therapies (including those currently marketed) made use of an autologous approach, using cells obtained from the individual to be treated. Autologous CAR T cell therapies are personalized therapies that involve collecting blood components, including T cells, through apheresis from a cancer patient; engineering the T cells with a CAR recognizing a cancer antigen, then injecting the cells back into that same patient. Now, the field is moving more and more towards allogeneic therapies (i.e., using cells that are genetically dissimilar). An allogeneic CAR T cell therapy is created with T cells from healthy donors that are genetically engineered, expanded and cryopreserved to provide a ready to use therapeutic solution for multiple patients.
To understand the shift from autologous to allogeneic, it is important to realize that, while several autologous CAR T therapies received marketing authorization by the Food and Drug Administration, there are a few issues that restrict their access to a wider population, including manufacturing and operational difficulties. First, patient-to-patient variability in the starting material is an important concern that can lead to variations in the yield or effectiveness of the end-product. Indeed, several factors might influence the quantity and/or fitness of the T cells used as starting material, such as the age of the patient, or clinical background such as previous lines of treatments that might affect the immune system. This lower quality in the starting material might sometimes result in manufacturing failures and consequently, lack of treatment for a patient that already underwent the apheresis procedure. Another barrier arises from the logistics, planning, and higher costs associated with specialized medicine that require single product manufacturing and release for each individual. The manufacturing, testing and release process itself is lengthy and this delay is an important concern for patients with rapidly progressing and aggressive cancers.6,7
As these issues are inherent to autologous therapies, a different strategy is needed to potentially help address some of these limitations. One main approach is to develop allogeneic therapies. Of note, the use of healthy donors means that there is a better consistency in the starting source of cells, therefore a greater opportunity to optimize the manufacturing process and to decrease variability between therapies. In addition, the ability to scale manufacturing to treat a large group of patients versus developing a single patient treatment also helps with potential cost effectiveness and the ability to improve pharmacoeconomic benefits. Importantly, there is a quicker turnaround time from treatment decision to infusion for patients as these CAR T cells are available “off the shelf”, ready to use as and when needed.8,9
New Challenges Facing Allogeneic CAR T
While allogeneic therapies offer significant new opportunities for treatment, they are not without their own difficulties. The initial challenge facing allogeneic therapies corresponds to the risk of the donor cells attacking the patient’s healthy tissues, known as Graft-versus-Host Disease (GvHD). Yet, the biggest challenges might be the opposite situation, the swift rejection of the therapy by the patient’s immune system, known as Host-versus-Graft (HvG) reaction. Both reactions are the result of an alpha beta T cell activation resulting from the specific recognition by TCR complexes of a target Human Leukocyte Antigen (HLA)-peptide complex.
To address the potentially life-threatening GvHD risk, the industry has predominantly moved towards developing gene editing technologies disrupting the alpha chain locus of T cell receptor (TCR) complex, which prevents the expression of the entire complex at the cell surface. While efficient at disrupting the TCR, this approach comes with its own set of regulatory challenges to address potential safety concerns regarding ‘off-target’ genetic cuts and chromosomal abnormalities as it relies on double strand cut of the DNA.8,10-12
The strategy regarding HvG reaction initially focused on fine-tuning lymphodepleting pre-conditioning regimens administered to the patient prior to the CAR T infusion derived from the autologous settings. The resulting decrease of circulating lymphocytes opens a therapeutic window for the CAR T to target the tumor cells without being rejected by the patient’s immune system. Nevertheless, other strategies are currently being tested to better protect allogeneic CAR T from rejection by the patient’s immune system. The main approach involves the knock-out or knock-down of beta-2-microglobulin, thereby preventing or diminishing the expression of class I Major Histocompatibility Complexes (MHC). While complete knock-out of the MHC class I expression might prevent T cell recognition, it has the potential drawback that it might activate Natural Killer cells, thus requiring additional tools to prevent rejection (such as expression of non-classical HLA-E or HLA-G, Siglec 7 and Siglec 9 ligands).8
Finally, the use of allogeneic cells translates to significant manufacturing changes with the need for maximizing the production yield through process optimization and scale-up. New equipment is therefore required to support increased output such as bioreactor solutions, automated fill and finish systems or storage solutions. This also results in the need to maximize the product purity to ensure only engineered T cells can be injected back to the patient.
Using Non-Gene Edited Technologies to Expand Reach of Allogeneic Therapies
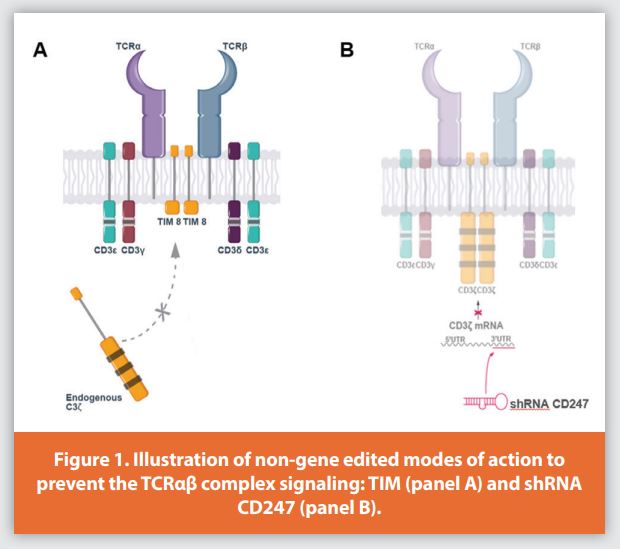
As an alternative to gene editing technologies, non-gene editing technologies provide an interesting approach to support the development of allogeneic CAR T cells. For example, non-gene editing technologies such as short hairpin RNA (shRNA) and T cell Receptor Inhibitory Molecule (TIM) are currently being used in the clinic to prevent the risk of GvHD as well as to downregulate the beta-2-microglobulin to prevent HvG rejection. They provide significant advantages because they do not act by cutting the genome but through disrupting the downstream mechanisms of action. shRNA acts at the mRNA level, before translation into protein, and TIM acts at the protein level, preventing activation of the signaling pathway within the T cell by outcompeting endogenous CD3ζ chain (i.e., CD247) within the TCR complex13 (Figure 1). The safety of these non-gene editing approaches to prevent GvHD (e.g. shRNA and TIM technologies) in allogeneic CAR T therapies is validated in current Phase 1 clinical trials performed by Celyad Oncology SA, including the Phase 1 alloSHRINK trial (NCT03692429) evaluating CYAD-101, a NKG2D-based CAR T expressing the TIM protein for the treatment of colorectal cancer and the Phase 1 IMMUNICY-1 trial (NCT04613557) evaluating CYAD-211, an anti-BCMA CAR T expressing one shRNA against CD3zeta for the treatment of multiple myeloma. So far, data from these trials have shown good tolerability and no evidence of GvHD in patients.
Untitled docuInterestingly, the use of shRNA in particular allows modulation of the effect desired: from complete to intermediate downregulation of the expression of a certain gene. For instance, to prevent for the risk of GvHD, one could select a shRNA targeting CD3ζ, a key component of the TCR complex mandatory for arrival at the cell surface, which results in complete knockdown of the TCR on T cells (Figure 2).
On the other hand, to prevent HvG rejection, one could favor a shRNA with moderate knockdown to reduce T cell allorejection while simultaneously avoiding NK cell rejection risked by a full knockout. This ability to titrate the effect of shRNA is illustrated in Figure 3. This further opens engineering possibilities to inhibit otherwise vital genes for which complete knockout would result in cellular misfunction.

Non-gene editing technologies such as TIM or shRNA can be delivered to the T cells through classical vector systems such as retro- or lentiviral vectors that have been used in the clinic for the last decades, or via newly developed systems such as transposons combined with electroporation. In both cases, one interesting feature of these approaches is the ability to engineer multiple genes in one single production step, including the expression of the chimeric antigen receptor, potential armoring with chemokines or cytokines and multiple targeted knockdowns.14,15 By way of example, it is nowadays possible to produce CAR T cells encoding up to six shRNA in one single engineering step. This obviously opens a playground to further improving the CAR T cells to maximize their potency along with their persistence. These additional weapons might be required to hopefully tackle solid cancer in the future.
Productivity and Manufacturing Go Hand in Hand
Single step delivery does not only provide scientific opportunities but also brings higher manufacturability.13 Indeed, from a process perspective, the complexity matters. Each processing step is inevitably associated with a certain performance reflected by efficacy (e.g., proportion of engineered cells within a total population) and recovery (e.g., the proportion of a desired cell lost in the process). Limiting the number of steps, including engineering and purification steps, is therefore paramount to achieve yield supporting the treatment of a maximum number of patients. In addition, it also opens the possibility to obtain significant yield with shorter ex-vivo cell culture process which has been associated with lower T cell differentiation, higher “cellular fitness” and therapeutic potential.16 This is a paradigm that clearly differentiates T cell-based therapies from more conventional biologic therapies: they rely on viable cells that functionally evolve through cellular activation signals, cellular divisions, and culture conditions, therefore currently limiting their ex-vivo expansion. Further research projects are ongoing to maximize productivity without impacting the therapeutic potential of those cells.
Will Allogeneic Outcompete Autologous CAR T?
One would need a crystal ball to answer this question. Certainly, there is still significant work ahead to demonstrate superior clinical efficacy towards the approved autologous counterparts or to provide significant clinical data for indications with limited therapeutic options such as for solid cancer. What is known today is that allogeneic CAR Ts provide an efficient solution to circumvent the key bottlenecks restraining access of CAR T cell therapeutic benefit to a larger patient population. Indeed, autologous cell therapies require lengthy vein-to-vein process and suffer from the variability of the patient-derived starting material (i.e., T cells). In contrast, allogeneic cell therapies utilizing healthy donor T cells limit variability and avoid immediate manufacturing demands as the cells are banked and ready for use. This approach is feasible thanks to the development of relevant methods that can interfere with the endogenous T cell receptor thereby avoiding GvHD, the main potential toxicity risk affecting allogeneic T cell therapy. Genetic ablation of TCR alpha using targeted gene-editing methods has been a common approach in the field, but risks related to double strand DNA breaks and complexity of manufacturing processes impacting cell fitness and/or yield are potential downsides associated with these technologies. An interesting alternative is provided by non-gene editing technologies which should be further considered as they bring potentially safer and more flexible options for the manufacturing of next-generation CAR T cells.
References
- Lee DW, Kochenderfer JN, Stetler-Stevenson M, et al. T cells expressing CD19 chimeric antigen receptors for acute lymphoblastic leukaemia in children and young adults: a phase 1 dose-escalation trial. Lancet 2015;385:517-28. 10.1016/S0140-6736(14)61403-3
- Maude S.L., Laetsch T.W., Buechner J.,., et al. Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N. Engl. J. Med. 2018;378:439–448. doi: 10.1056/ NEJMoa1709866
- Wang, M., Munoz, J., et al. KTE-X19 CAR T-Cell Therapy in Relapsed or Refractory Mantle- Cell Lymphoma. N. Engl. J. Med. 2020; 382:1331-1342. DOI: 10.1056/NEJMoa1914347
- Mikkilineni, L., Kochenderfer, J.N. CAR T cell therapies for patients with multiple myeloma. Nat Rev Clin Oncol 18, 71–84 (2021). https://doi.org/10.1038/s41571-020-0427-6
- Melenhorst, J.J., Chen, G.M., Wang, M. et al. Decade-long leukaemia remissions with persistence of CD4+ CAR T cells. Nature (2022). https://doi.org/10.1038/s41586-021- 04390-6
- Kohl U., Arsenieva S., Holzinger A., Abken H. CAR T Cells in Trials: Recent Achievements and Challenges that Remain in the Production of Modified T Cells for Clinical Applications. Hum. Gene Ther. 2018;29:559–568. doi: 10.1089/hum.2017.254. - DOI - PubMed
- Salmikangas, P., Kinsella, N. & Chamberlain, P. Chimeric antigen receptor T-cells (CAR T-cells) for cancer immunotherapy — moving target for industry? Pharm. Res. 35, 152 (2018). - PubMed - PMC
- Depil S, Duchateau P, Grupp SA, Mufti G, Poirot L. ‘Off-the-shelf’ allogeneic CAR T cells: development and challenges. Nat Rev Drug Discov. 2020 Mar;19(3):185-199. doi: 10.1038/ s41573-019-0051-2. Epub 2020 Jan 3. PMID: 31900462.
- Costariol E, Rotondi MC, Amini A, et al. Demonstrating the Manufacture of Human CAR-T Cells in an Automated Stirred-Tank Bioreactor. Biotechnol J. 2020;15(9):e2000177. doi:10.1002/biot.202000177
- Osborn M, Webber B, Knipping F, et al. Evaluation of TCR Gene Editing Achieved by TALENs, CRISPR/Cas9, and megaTAL Nucleases. Molecular Therapy. VOLUME 24, ISSUE 3, P570-581, MARCH 01, 2016 DOI:https://doi.org/10.1038/mt.2015.197
- Kosicki M, Tomberg K, Bradley A. Repair of double-strand breaks induced by CRISPR-Cas9 leads to large deletions and complex rearrangements. Nat Biotechnol. 2018;36(8):765- 771. doi:10.1038/nbt.4192
- Hahn E, Hiemenz M. Therapeutic Gene Editing with CRISPR: A Laboratory Medicine Perspective. Clin Lab Med. 2020;40(2):205-219.Maus MV, June CH. Making Better Chimeric Antigen Receptors for Adoptive T-cell Therapy. Clin Cancer Res Off J Am Assoc Cancer Res. 2016;22(8):1875-1884
- Michaux et al. Clinical Grade Manufacture of CYAD-101, a NKG2D-based, First in class, non- gene edited allogeneic CAR-T cell therapy, Journal of Immunotherapy
- Lesch, S., Blumenberg, V., Stoiber, S. et al. T cells armed with C-X-C chemokine receptor type 6 enhance adoptive cell therapy for pancreatic tumours. Nat Biomed Eng 5, 1246– 1260 (2021). https://doi.org/10.1038/s41551-021-00737-6
- Hu B, Ren J, Luo Y, et al. Augmentation of Antitumor Immunity by Human and Mouse CAR T Cells Secreting IL-18. Cell Rep. 2017;20(13):3025-3033. doi:10.1016/j. celrep.2017.09.002-16
- Ghassemi S, Bedoya F, Nunez-Cruz S, et al. Shortened T cell culture with IL-7 and IL-15 provides the most potent chimeric antigen receptor (CAR)-modified T cells for adoptive immunotherapy. J Immunol 2016, 196 (1 Supplement) 214.23