Dr. Yassen Abbas - Lead Scientist, CN Bio Innovations Ltd.
Article Synopsis
Absorption, distribution, metabolism, and excretion (ADME) studies are a critical component of preclinical drug discovery, providing important insights into the pharmacological properties of a drug, including indicators of a drug candidate’s efficacy, and safety. ADME studies help to inform candidate selection for clinical progression as well as dosing regimens, to ensure clinical trials provide meaningful and actionable data and most importantly, at minimal risk to human health. Despite this, ADME studies are often held back due to a lack of human-relevant data obtained during preclinical studies.
In this article, the author discusses the common drawbacks to ADME studies using conventional methods, and how these issues can affect candidate selection and dosage. The article will also discuss emerging complementary technologies, such as organ-on-a-chip, and how these technologies allow for human-relevant in vitro preclinical ADME studies that better inform in vivo experimentation. Finally, the article will discuss bioavailability, and how using organ-on-a-chip technology can support the determination of human bioavailability to determine drug dosing regiments, reduce side-effects, and potentially recover flawed therapeutic candidates.
Absorption, distribution, metabolism, and excretion, or ADME, studies are a critical component of preclinical drug discovery; designed to provide deeper insights into how a therapeutic behaves within a living organism. The findings are harnessed to inform the direction of clinical studies, providing early data on a drug’s efficacy and the dosing regimen required for treatment. Conventionally, ADME studies are performed either using chemistry-based methods, such as determining the solubility of a compound, or using biological models that range in complexity from in vitro 2D cell culture to in vivo animal studies. However, recreating human representative biological models in the lab is challenging, making it difficult to accurately measure these important parameters and significantly impacting drug development processes. New approach methodologies (NAMs), such as organ-on-a-chip (OOC) technology, are helping to overcome these barriers, enabling researchers to reevaluate dosing regimens, reduce side effects and potentially even recover therapeutic candidates that failed due to poor ADME properties.

Drug developers carry out ADME studies early in the development pathway to understand the pharmacokinetic behavior of a therapeutic candidate; they assess a series of critical parameters of its chemical properties and how it responds in the body. These include the rate the drug is absorbed through the gastrointestinal tract, rate of clearance by the liver and identification of metabolites, and whether it can achieve sufficient concentrations in the blood to be effective at the site of action.1 These studies also factor into another essential measure of a drug’s effectiveness – bioavailability. Defined as the proportion of a drug which enters circulation when introduced into the body and so can have an active effect, bioavailability enables researchers to predict dosages required for a patient to receive an efficacious amount of a therapeutic compound. Taken together, preclinical ADME and bioavailability studies are key to identifying lead compounds with optimal properties, optimizing efficacy, and minimizing safety issues. By providing an early insight into how a molecule may behave in human clinical trials, the findings help to ensure that only safe and effective therapeutics progress. Therefore, the accuracy and efficiency of the methods chosen by researchers hold huge significance for drug developers in determining the success of programs.
The Drawbacks of Conventional Methodology
Traditionally, biological-based ADME and bioavailability studies are conducted in two stages, beginning with in vitro, 2D cell culture. This method is cost-effective, utilizing very simple monocultures of cells to enable the researcher to assess initial parameters that are crucial to a drug’s success, such as the extent of protein binding, the likelihood of inhibition of major drug metabolizing enzymes, and insights into its metabolic stability.
Following this, promising candidates can be further investigated using in vivo animal models. These complex studies enable researchers to assess a drug in the context of a living organism, providing deeper insights into its systemic effects, including across the intricate, multi-organ systems that are particularly hard to recapitulate in in vitro models, such as a complete immune system or circulatory system. When taken together, this two-stage system provides researchers with key data to make predictions about a drug’s likelihood of clinical success, and consequently make the decision whether to progress a candidate to clinical trials. However, they are not without their drawbacks. Studies have shown that as many as 5-10% of clinical failures are due to issues with pharmacokinetics.2 When considering estimates that place the total cost of progressing a drug candidate from discovery to market as high as $2.3B, the insights these studies can provide become significant, not only to maximize chance of candidate success, but also to reduce the financial burden of potential clinical failures on the industry.3
So, what limits the success of these methods in pharmacokinetic studies? In general, both in vitro 2D cell culture and in vivo animal models are limited by poor clinical translatability – inherently, the data they produce does not always accurately predict human responses. Whilst 2D cell culture can be a useful tool for initial analysis, the models lack physiological relevance and their simplicity does not facilitate researchers to account for a drug’s effects across different tissues or cell types, nor replicate complex inter-organ and systemic effects, such as blood perfusion or immune responses.
Animal models offer this level of complexity; however, a host of interspecies differences limit their predictability in humans. Humans and animals differ in many ways, ranging from gene expression profiles to metabolic capacity, for example in the human cytochrome p450 enzymes which are key players in the detoxification of drugs, cellular metabolism, and homeostasis. Furthermore, considering in vivo trials can be conducted in a range of different species, the disparity increases. Because of this, it is very hard to extrapolate data reliably from animal into humans, as evidenced by Musther et al. in 2014, where oral bioavailability was compared between various animal models and humans across a database of 184 drug compounds.4 Commonly used animal models – mouse, rat, and dog – showed poor correlation with human bioavailability (R2 = 0.25, 0.28, and 0.37 respectively). Non-human primate (NHP) models provide an improved bioavailability correlation with humans (R2 =0.69), although these models are not commonly used due to significant ethical considerations, stringent regulatory requirements, and high cost. Whilst these data do not eliminate the usefulness of animal models for pharmacokinetic analysis, it highlights that these studies are best used as qualitative indicators, rather than quantitative data.
In drug development, some of the most important innovations over the past few decades has been computational or in silico tools to screen for new compounds and to predict ADME behavior from a compound’s chemical structure. Clinical behavior can be forecasted using physiological based pharmacokinetic (PBPK) modelling which combines a compound’s chemical properties, the physiology-based properties of population being modelled, and data from ADME studies. These models are becoming increasingly important prior to trials in humans, however, their ability to accurately predict outcomes in the clinic will often be constrained by the quality of the data imputed.
Poor clinical translation can also result in significant knock-on effects in the latter stages of drug development. A lack of accurate pharmacokinetic data can lead to miscalculations of dosing regimens – an issue that, at best, can mean the drug shows a lack of efficacy, and, at worst, can cause serious adverse effects. Either way, this can result in the failure of a drug candidate. These drawbacks, considered alongside the increasing cost of in vivo animal studies (particularly NHP’s) and the associated ethical considerations, demonstrate the distinct need for improved predictors of human outcomes in preclinical research.
Organ-on-a-Chip – The Solution to Human Relevance
As awareness regarding the limitations of conventional in vitro and in vivo models gains traction, many innovative new approach methodologies (NAMs) have been developed to address the gaps. One of the leading technologies in this field is organ-on-a-chip (OOC), which, over the last decade, has emerged to bridge the gap between traditional in vitro assays and in vivo tissue functionality in humans. OOC technology, or microphysiological systems (MPS), has several key advantages over 2D in vitro cell culture. Firstly, the systems are designed to feature constant fluid perfusion, which mimics blood flow by delivering nutrients and removing waste from the cells. Also, the technology can utilize multiple human cell types, to recapitulate the architecture and multiple processes of tissues or organs. Because of this, these models exhibit similar functionality to human organs, to better reflect drug responses in the body. Perhaps most critical to advancing the field of ADME and bioavailability studies in recent years has been the development of multi-organ MPS. Using fluidic interconnection, relevant organ models can be linked together, providing human relevant systems that more closely offer the complexity of animal studies.
As mentioned previously, initial in vitro assessment of metabolism and bioavailability is often carried out using 2D cell cultures. The standard practice for these experiments is to use immortalized intestinal cell lines and primary suspension hepatocytes, cells that are known to be poor predictors for this type of study due to low expression levels of metabolic enzymes, in addition to the short duration of culture for primary cells. Using OOC, complex multi-organ MPS have been created that more accurately replicate the interactions between the gut and liver (Figure 1). These models utilize liver and intestinal microtissues, formed via seeding primary human hepatocytes and gut cells, respectively, onto specially designed scaffolds that replicate the architecture of the human organ. Fluidic connection, via micropumps, is used to ensure the flow of liquid, drug and signaling molecules between the organs, to mimic blood circulation, including expression of a range of cytochrome p450s and transporters. By accurately recreating the process of drug absorption and first-pass metabolism, these advanced MPS can derive bioavailability, offering enhanced predictivity versus animal models.
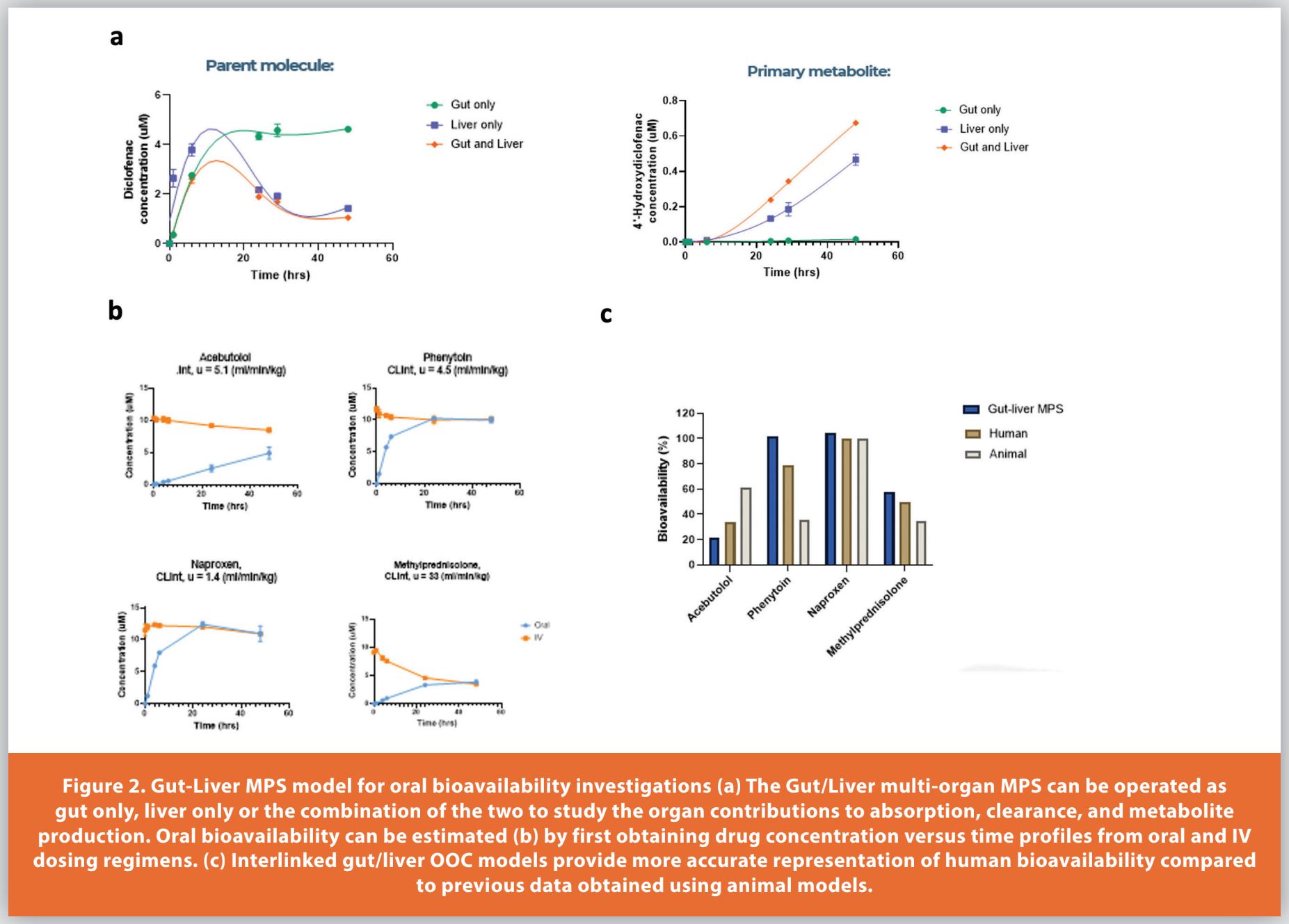
In a recent study highlighting the effectiveness and flexibility of these multi-organ MPS for ADME studies, a leading multi-organ MPS was operated as either gut only, liver only, or the combination of the two organs: gut tissue interconnected with liver tissue. Diclofenac was used as an example whereby the contributions to the clearance and production of metabolites by the gut and liver tissue could be assessed separately and when in combination. In a single experimental system, multiple key ADME parameters were shown to be estimated and then extrapolated using in silico models for in vivo prediction.5,6
Oral bioavailability is a parameter that depends on both the extent of intestinal absorption and the rate of hepatic clearance and is well suited for estimation by multi-organ MPS comprising of both gut and liver tissues. Here, the multi-organ MPS operated as either oral (both gut and liver tissues) or IV (liver only) (Figure 1), and the bioavailability was estimated by determining the area under the curves of both dosing regimens (Figure 2).6
Despite being the primary absorption site for many drug products, the gut isn’t the only organ that must be studied when seeking to measure absorption and bioavailability. Inhaled medications represent a growing portion of therapeutics due to an array of benefits offered by the lungs, including a large, thin surface area for rapid absorption, direct access to the bloodstream, and a lack of required metabolic activity relative to the gut.
However, the lung presents many challenges for ADME studies. Being a particularly large and complex organ, most in vitro models fail to account for the number of factors that can influence drug absorption here, for example, the size of a drug particle. Larger particles are likely to settle within the proximal lung – a region containing a thick mucus coating and beating cilia, presenting a significant barrier to entry unless a drug can rapidly dissolve and diffuse into the epithelium before it is cleared. By contrast, small particles will likely reach the alveolus, which contain extremely thin epithelium and provide an ideal point of entry, however, these regions also contain alveolar macrophages that can engulf foreign bodies before they can enter the bloodstream.
These difficulties in modeling are not just limited to in vitro models. Studies conducted in vivo are often constrained by the physical act of inhalation. Poor technique, or poorly fitting inhalation apparatus, can lead to significant variation in the amount of drug product entering the body. Additionally, the rate of breathing and volume per breath can vary significantly between individuals due to many factors. This is particularly pertinent during in vivo animal studies, where factors such as stress can have a serious impact on an animal’s breathing rate.
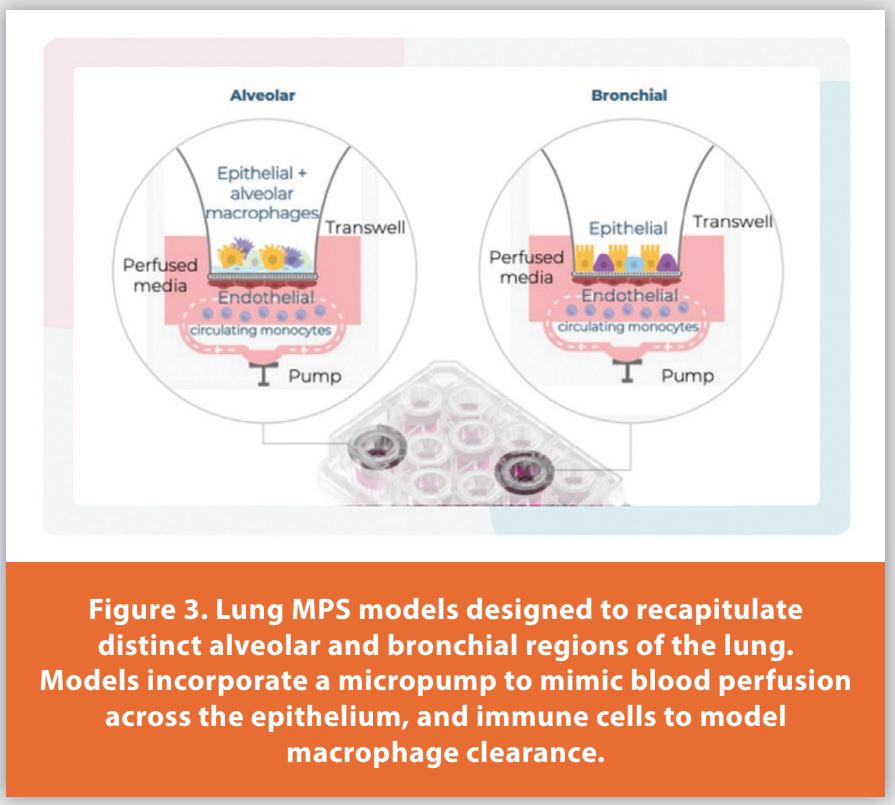
Because of these difficulties, the lung has become an area of interest amongst the OOC community. Data presented by Richardson et al. in 2023 outlined the potential of the technology to develop more human relevant in vitro models for ADME and bioavailability studies of inhaled medications.7 Given the physical variation between distinct regions of the lungs, the team developed separate models of both the alveolar and bronchial regions of the lungs using primary human cells that make up the epithelium of each region, alongside endothelium layers and a micropump to mimic blood perfusion (Figure 3). Each model was also developed to feature immune cells, enabling researchers to mimic drug loss via immune cell clearance.
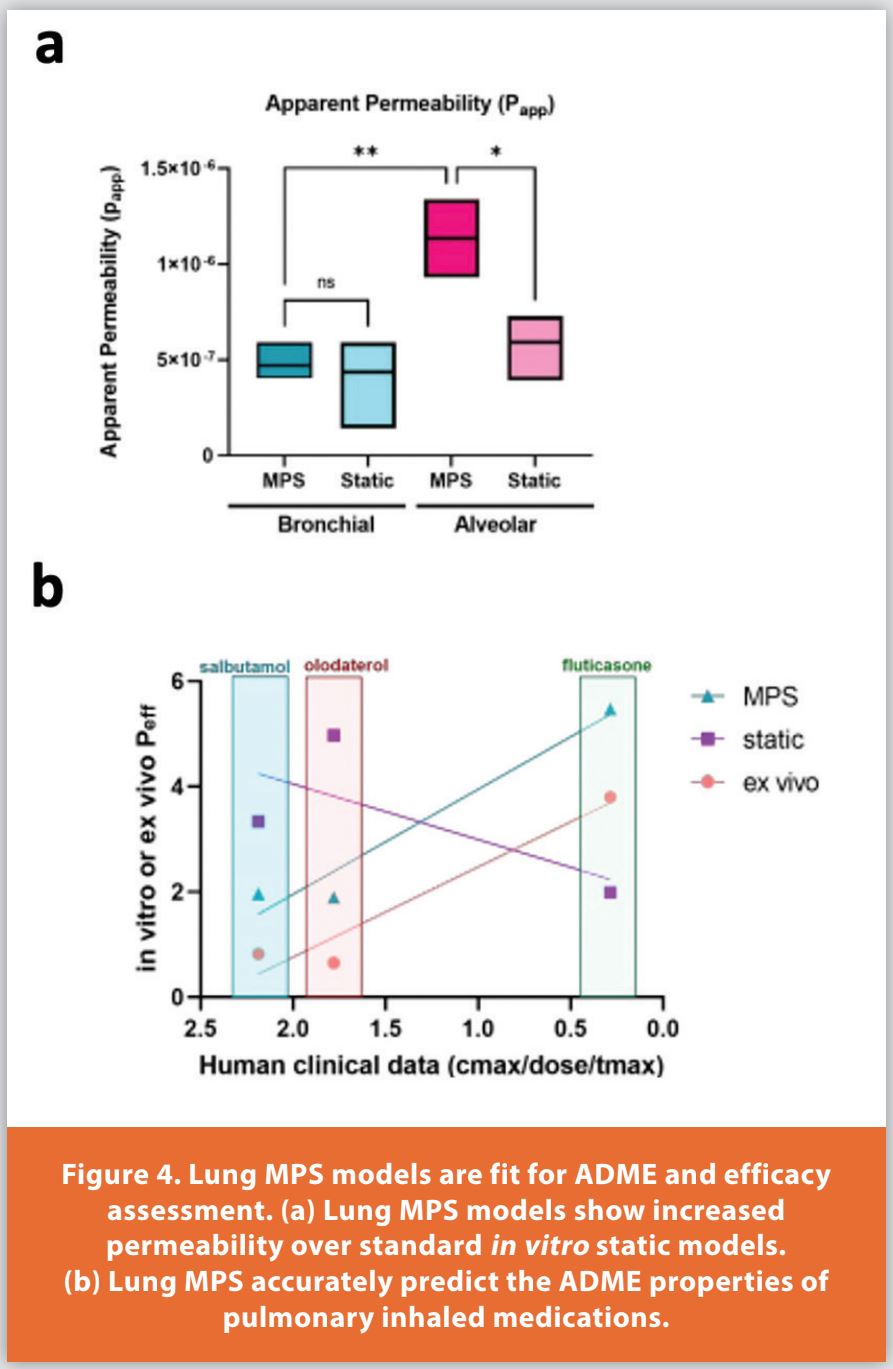
The research concluded that both models showed a significant increase in permeability relative to static in vitro cell cultures (Figure 4 a).7 These lung MPS models also showed conserved human phenotypes with both ATI and ATII cell types being expressed in the alveolar model, and mucus secretion in the bronchial model, along with the presence of goblet and club cells.
A recent study showcased the potential of lung MPS, using primary cells under perfusion, for ADME studies.7 Three inhaled medications (Salbutanol, Olodaterol and Fluticasone) were used as an example to assess drug ADME prediction of the alveolar lung MPS model compared to standard in vitro preclinical models (ex vivo and static cell culture). The study highlighted the lung MPS model as more human and clinically relevant than current standard in vitro models (Figure 4b).
A Look to the Future – ADME and Bioavailability
Advanced NAMs hold the potential to transform drug discovery programs. By providing researchers with the opportunity to recreate human physiology in the lab, MPS can be used for a myriad of applications that further our understanding of disease mechanisms, uncover potential therapeutic targets, and assist with the safe and efficacious development of potential therapeutics.
Determining the ADME and bioavailability properties of compounds is essential for lead optimization and candidate selection in early drug discovery, through to dose refinement and successful translation to clinic. The challenges of using traditional in vitro and in vivo methods demonstrate the huge potential of harnessing OOC technology throughout these investigations. Single- and multi-organ models closely predict human in vivo pharmacokinetics for more informed decision-making and provide deeper insights into the therapeutic window of a drug. Not only would this help to reduce drug attrition rates, an extremely costly issue within the pharmaceutical industry, but it could even enable drug developers to revisit candidates that were previously thought to be flawed.
A better understanding of how a drug interacts with the human body is integral to effective and streamlined drug development, the benefits to gaining these insights during the preclinical stage of research cannot be overstated. The potential of OOC technology on the world of preclinical drug development is yet to be fully realized, but as the field expands and adoption of NAMs continues to grow, we move closer to our goal of enabling safer and more efficacious drugs to get to market faster than ever before whilst reducing the number of animals required.
References
- Doogue, M.P. and Polasek, T.M. (2013) ‘The ABCD of clinical pharmacokinetics’, Therapeutic Advances in Drug Safety, 4(1), pp. 5–7. doi:10.1177/2042098612469335.
- Kola, I. and Landis, J. (2004) ‘Can the pharmaceutical industry reduce attrition rates?’, Nature Reviews Drug Discovery, 3(8), pp. 711–716. doi:10.1038/nrd1470.
- Philippidis, A. (2023) The unbearable cost of drug development: Deloitte Report shows 15% jump in R&D to $2.3 billion, GEN. Available at: https://www.genengnews.com/gen-edge/the-unbearable-cost-of-drug-development-deloitte-report-shows-15-jump-in-rd-to-2-3-billion/#:~:text=Deloitte%20found%20that%20the%20average,clinical%20 trials%20to%20the%20market. (Accessed: 19 October 2023).
- Musther, H. et al. (2014) ‘Animal versus human oral drug bioavailability: Do they correlate?’, European Journal of Pharmaceutical Sciences, 57, pp. 280–291. doi:10.1016/j. ejps.2013.08.018.
- Milani et al. (2022) ‘Application of a gut–liver-on-a-chip device and mechanistic modeling to the quantitative in vitro pharmacokinetic study of mycophenolate mofetil’, Lab Chip, 22, pp. 2868https://pubs.rsc.org/en/content/articlehtml/2022/lc/d2lc00276k
- Abbas et al. (2021). Improved prediction of oral bioavailability using a gut-liver microphysiological system. https://cn-bio.com/resource/improved-prediction-of-oral-bioavailability-using-a-gut-liver-microphysiological-system/
- Richardson et al. (2023). Evaluation of in vitro human alveolar and bronchial microphysiological systems to predict the permeability and absorption of inhaled pulmonary medications. Poster presented at: ELRIG Drug Discovery; 04/10/2023; London, UK. https://cn-bio.com/resource/evaluation-of-in-vitro-human-alveolar-and-bronchial-microphysiological-systems-to-predict-the-permeability-and-absorption-of-inhaled[1]pulmonary-medications/
Author Biography
Dr. Yassen Abbas is a Lead Scientist at CN Bio Innovations. He completed an MEng in chemical engineering at The University of Edinburgh and joined the European Space Agency as a graduate engineer. He later received a Ph.D. from the University of Cambridge and completed a postdoc fellowship, also at Cambridge, on the development of a tissue-engineered model of the human endometrium. He has experience with real-time sensor technology, organoids and the development of in vitro tissue models using human primary cells. Dr Abbas has published five peer-reviewed scientific articles, four as first author.
Publication Detail
This article appeared in American Pharmaceutical Review:
Vol. 26, No. 8
Nov/Dec 2023
Pages: 36-40
Subscribe to our e-Newsletters
Stay up to date with the latest news, articles, and events. Plus, get special
offers from American Pharmaceutical Review delivered to your inbox!
Sign up now!