Introduction
The pivotal role of human behavior in aseptic operations cannot be overstated, as it significantly influences the safety and efficacy of sterile drug products. This article delves into the incorporation of human factor principles as a proactive and strategic move, aiming to navigate the complexities inherent in aseptic operations and, in turn, ensure the steadfast safety and efficacy of sterile drug products. The approach systematically addresses human factors that may impact aseptic operations. First, organizations recognizing and accounting for the human element in the aseptic manufacturing process go a long way in initiating mitigation activities.
Recent regulatory scrutiny and the lessons drawn from FDA form 483s and Warning Letters1,2 underscore the urgency for a paradigm shift towards enhanced human factor risk management and intervention strategies. Most behavioral observations pertained to violations of first air principles, especially in Grade A areas during aseptic filling operations. The cleanroom behaviors, such as slow and deliberate movement in such a way that unidirectional airflow is not disrupted, routine hand sanitization, sterile gown/glove management during operation, going over vials, equipment open door/closed door setup, vial loading/unloading, stopper replenishment process steps, handling of broken vials, and interventions were all examples of areas where the regulator was concerned for RABS systems. In some cases, the CCTV video observed by the regulator proved that the documented activities were indeed not performed, questioning employee integrity and management effectiveness. The observations also emphasized the importance of air visualization studies. The inspectors closely monitored the interventions either live or via CCTV footage to ensure aseptic product safety and to assess the effectiveness of aseptic processing simulations. In many cases, organizations encountered shortcomings here. The challenges encompass a spectrum of factors, ranging from lapses in personnel training, personal integrity, and awareness, to equipment design and facility layout issues. The consequences of overlooking these crucial aspects can be severe, with potential ramifications for the quality and safety of sterile drug products and the organization. These recent instances have cast a spotlight on the imperative for the industry to fortify its human factor risk.
Cleanroom Behaviors Impacting Patients
The sterility of a cleanroom component or the final product means the complete absence of viable microorganisms, including viruses, which pose a risk to the patient during administration. While achieving sterility in parenteral manufacturing is important, it does not guarantee the absence of non-viable pyrogens. To prevent pyrogenicity, it is essential to avoid endotoxins, which are lipopolysaccharides that are shed into the environment once a gram-negative bacterium dies and lyses. Endotoxin levels are determined by the Limulus Amoebocyte Lysate (LAL) test based on the clotting reaction of the hemolymph of the horseshoe crab. Clinical cases3 have confirmed the serious risks associated with endotoxins, which can lead to anaphylactic shock and death of patients.
Conducting smoke studies in cleanrooms is crucial to validate the effects of operational interventions on unidirectional airflow. Swift movements by operators can disrupt the airflow, leading to the generation of airborne particles. Research indicates that the movement of operators results in the formation of recirculation zones, causing localized turbulence and the entrapment of contaminants.4 The establishment of a low-pressure zone, either by the presence of personnel or an obstacle, may lead to a reversal of airflow, detrimentally affecting the initial air curtain designed to prevent the entry of contaminants.
The primary goal of utilizing sterile gloves in a cleanroom setting is to prevent the introduction of human skin-associated microorganisms and to prevent cross-contamination. The effectiveness of this preventive measure relies on the integrity and proper selection of the gloves. Notably, nitrile gloves exhibit less elasticity compared to latex or vinyl gloves. Vinyl gloves may also have lower resistance to alcohol compared to latex.5 The process of donning sterile gloves, influenced by the operator’s skill, has the potential to introduce contamination. It is crucial to emphasize that merely observing an operator wearing gloves without assessing their glove management behavior leads to a false sense of confidence. Glove management behavior encompasses the operator’s consistent disinfection of gloved hands, the use of a reproducible disinfection technique, disinfecting before and after use, and the regular changing of gloves after interventions. Wearing gloves despite the hands being damp from either disinfectant or handwashing is a common occurrence. Additionally, the operator ensuring a consistent transition from dirtier to cleaner area while simultaneously managing the operations task is very hard. This behavioral-based glove-to-glove, glove-to-surface, and surface-to-glove cross-contamination potentials have been well established. The glove disinfection stations/containers contaminated with pathogens from improper usage can serve as an additional potential source. Glove integrity can be breached by operators, introducing risks.
The primary source of contaminants in cleanrooms is personnel.6 Therefore, maintaining aseptic gowning practices is crucial for controlling contamination and preventing the transmission of microbes and bodily fluids during cleanroom activities. The behavior of the operators and the integrity of the gown itself can pose contamination risks. For example, after washing and irradiation, reusable cleanroom apparel has been shown to significantly degrade its Bacterial Filtration efficiency (BFE).7 Human activities and perspiration can contribute to contamination, making the length of wearing a gown and individual operator physiology key variables in addition to clean room temperature/RH conditions. Even with cleanroom contamination controls, viable organisms and non-viable particulates may persist in the cleanroom air and on various surfaces, including walls and equipment, because of ongoing activities (Figure 1). This contamination can transfer onto the operator’s gown. Contamination from particulates generated by humans can have a considerable impact on the cleanliness of a cleanroom. Whether stationary or walking, an individual dressed in cleanroom attire can produce between 100,000 and 1,000,000 particles per minute.8 Hence, it is crucial to regulate the occupancy of a cleanroom. Personnel following proper gowning practices, including good personal hygiene, are essential to minimize contamination risks in cleanroom environments. The management of pre-sterilized materials, sterile components, environmental monitoring plates, operational interventions, and various other factors influenced by human behavior also has the potential for introducing contamination.
Established Industry Best Practices
Aseptic processing contamination has been attributed to being caused primarily by three factors (Figure 2). Once the operational design, environmental, and engineering controls are in place and monitored, the major residual risk becomes the consistency and adequacy of personnel practices during aseptic operations. Hence, the industry has been developing and implementing best practices specific to aseptic manufacturing operations.10-15
![Figure 1. RABS Filling Line [Courtesy: Itaan Pharma]](http://media.americanpharmaceuticalreview.com/m/28/article/611943-1.jpg)
The best practices10 reiterate that theoretical knowledge is insufficient, and operators must excel in their aseptic practice. While gowning qualification establishes the operator’s practical gowning proficiency, the operator’s proficiency in aseptic processing is established through participation in media fill. It is recognized that the operator’s aseptic technique deteriorates with time; hence, as part of the process simulation and during risk assessment, personnel fatigue factors need to be always considered. Some of this can be eliminated through the improvement of ergonomics in an operational setting. All aseptic manipulations need to be made in First Air, not having passed any other components or being blocked by the operator’s own hands; again, these are tasks requiring meticulous skill to avoid contamination. A clear delineation of primary and secondary operator activities is required such that they don’t pose incremental risks to the product. The primary operator, by procedure, needs to be always cognizant about not contacting non-sanitized or non-sterilized during the entire aseptic operation. The operator should conduct the aseptic removal of the final wrap only during the introduction stage. The component preparation teams’ wrapping skills often come into play for seamless unwrapping and installation. Sterile tools associated with sterile supports, hangers, and their adequate placements are required to minimize contact between the toll and surfaces. The sampling step should be performed in such a way that it does not pose any contaminating risks. Where possible, best practices highlight that significant assembly is avoided by using sterilized pre-assembled items. Overall, the long-established industry best practices in aseptic operations are highly influenced by the operator’s level of training and the resulting behavioral patterns displayed.
COM-B Framework for Behavioral Change
The Capability, Opportunity, Motivation-Behavior (COM-B) model is a systematic theoretical framework of behavior change developed by Susan Michie, Maartje van Stralen, and Robert West in 2011.16 The human behavior model identifies capability (C), opportunity (O), and motivation (M) as the three key factors capable of influencing behaviors. The theory identifies that behavioral changes can be induced by modifying one of the components. A recent study 17 identified that opportunity and motivation directly affected hand hygiene behavior. While capability and opportunity were indirectly linked to hand hygiene behavior through motivation (Figure 3). The study substantiates the direct applicability of the COM-B Model in enhancing aseptic behaviors, which include hand hygiene practices.
Factors such as those in Table 1 can induce positive behaviors during aseptic processing.
Introducing Critical Behavioral Attributes (CBAs)
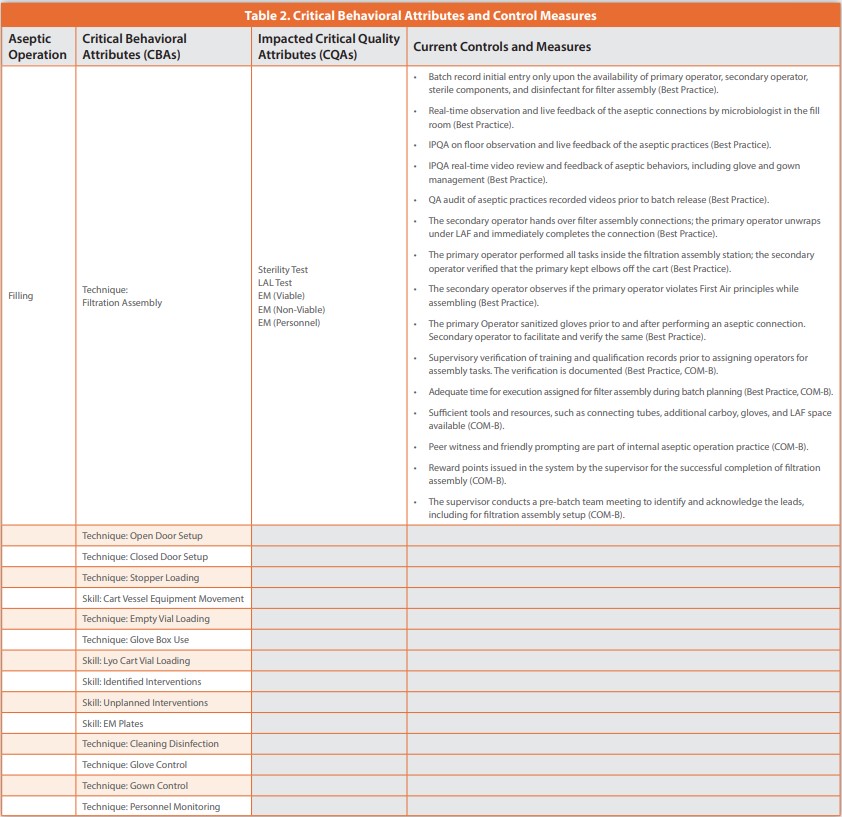
Based on the above discussions, it is evident that aseptic behavior requirements and human behavior improvement traits are well understood and characterized; the limitation now becomes establishing a product/process-specific model to ensure consistent adoption of these behavioral requirements. The repeated aseptic behavior failure during regulatory inspection necessitates a renewed look at how behavioral requirements need to be identified and controlled upfront as part of process development itself. The sources of variability addressed during development include- material (ex., raw materials, components), machine (ex., manufacturing equipment), method (ex., manufacturing process, cleaning process, analytical process), measurement (ex., analytical instrument), mother nature (ex., temperature, humidity conditions), and man (ex. operators, analysts). An ICH Q8 (QbD) 18-based process development (Stage 1 of the process validation lifecycle) identifies the Critical Material Attributes (CMAs) and Critical Process Parameters (CPPs) and determines their degree of impact on Critical Quality Attributes (CQAs) through the planned Design of Experiments (DoEs). The equipment, instrument, facility- temperature, and humidity variability are well understood and controlled as part of qualification efforts (Stage 2A of the process validation lifecycle). Raw material attributes are established and controlled as part of development. While components are qualified for aseptic operations, their sterility maintenance is also ensured. The process control strategy should encompass the controls related to minimizing potential sources of variability that impact CQAs. In addition to the above parameters and attributes affecting product Safety, Identity, Strength, Purity, and Quality (SISPQ), an aseptic process needs to also focus on personal aseptic behavioral controls. The reason is that personal behavioral variability can result in loss of product sterility and cross-contamination, both patient-critical. For this reason, we propose a new set of behavioral criteria, namely- Critical Behavioral Attributes (CBAs) similar to CMAs and CPPs in the case of aseptic manufacturing processes. The CBAs need to be identified, and the additional controls in place need to be enumerated since these human behavioral attributes are difficult to qualify. Table 2 displays one such example.

The purpose of identifying CBAs per operation and applying risk-based controls as part of Stage 1 (of the process validation lifecycle) is to reduce the variability associated with patient-impacting behaviors. The consistency of the CBAs needs to be confirmed during PPQ (Stage 2B ), and CBAs need to be monitored as part of the CPV (Stage 3) program.19 When adequate electronic or automation technology becomes available, organizations should switch to those solutions to reduce behavioral bias as much as possible. Switching from manual Tyvek lid removal and inner liner removal of the Pre-Filled Syringe (PFS) tub to automatic removal by robotic arms is one example. Tools such as the Post Approval Change Management Protocol (PACMP), as stipulated in ICH Q12,20 may be utilized to implement the change, thereby minimizing the impact of a CBA, i.e., tub loading technique.
Conclusion
Aseptic best practices have been in place in the industry for decades. However, the Quality by Design (QbD) concepts to process development and the Capability, Opportunity, and Motivation Behavior (COM-B) model for behavioral change are relatively new concepts introduced in 2008 and 2011, respectively. The industry has also adopted lifecycle concepts since the introduction of the US FDA process validation guidance in 2011. As established in the industry best practices guidance, aseptic processes peremptorily require control of aseptic behaviors to meet patient safety and product quality needs. Further, to align with the current ICH and lifecycle concepts, early identification and systematic mitigation or development of a control strategy is required as part of product development (Stage 1). The introduction of the Critical Behavioral Attributes (CBAs) elements supports defining and enumerating the aseptic behavior controls established for the product. The existence of CBA in your control strategy acknowledges the importance of behavioral elements to achieve sterility and prevent cross-contamination. The availability of CBAs allows for future risk reduction opportunities, such as the introduction of automation solutions. This is supported by the US FDA’s drive to modernize the industry.
This article integrates behavioral science concepts (COM-B model) and CBAs with pharmaceutical best practices and regulatory considerations (QbD and PV lifecycle). This connection emphasizes the need for the identification and systematic mitigation of behavioral challenges at an early development stage rather than addressing them reactively. The authors take this opportunity to call on manufacturers to adopt this improved framework for addressing the current aseptic behavior regulatory challenges and to achieve consistent behavioral patterns. The facility’s contamination control strategy may also incorporate the presence of a site COM-B model and the existence of CBA controls for aseptically manufactured products. The introduction of the framework also enhances the site’s Quality Management Maturity (QMM)21 as it displays a high level of management commitment to quality, advances the existing Pharmaceutical Quality System (PQS, and effectively improves employee engagement and empowerment.
References:
- FDA (2024) Data Dashboards- Inspections, US FDA. https://datadashboard.fda.gov/ora/cd/ inspections.htm
- FDA (2024) Warning Letters, US FDA. https://www.fda.gov/inspections-complianceenforcement-and-criminal-investigations/compliance-actions-and-activities/warningletters
- Wang, F. et al. (2012) Acute intraocular inflammation caused by endotoxin after intravitreal injection of counterfeit bevacizumab in Shanghai, China. Ophthalmol.
- Yang, S., Fu, W. (2002) A numerical investigation of effects of a moving operator on airflow patterns in a cleanroom, Building and Environment 37(7):705-712.
- Sandle, T. (2023) Glove disinfection, and aseptic technique: Creating a schema for the cleanroom and laboratory EJPPS, 282.
- Deveau, I. F. (FDA) FDA Inspectional Observations and Corrective Actions, CDER.
- Larkin, D. (2012) The contamination risks posed by laundered cleanroom apparel, Kimberly-Clark Professional.
- Soper, M. (2017) How can Employees Contaminate a Clean Environment? Setra
- Friedman, R. L. (2005) Aseptic processing contamination case studies and the pharmaceutical quality system. PDA journal of pharmaceutical science and technology.
- PDA (2013) Technical Report No. 62 (TR 62) Recommended Practices for Manual Aseptic Processes, PDA.
- ISPE (2018) Baseline Guide Vol 3: Sterile Product Manufacturing Facilities 3rd Edition, ISPE.
- PDA (2015) Technical Report No. 70 (TR 70) Fundamentals of Cleaning and Disinfection Programs for Aseptic Manufacturing Facilities, PDA.
- PDA (2016) Points to Consider for Aseptic Processing, PDA.
- PDA (2011) Technical Report No. 22, Process Simulation for Aseptically Filled Products, PDA.
- PDA (2008) Technical Report No. 44, (TR 44): Quality Risk Management for Aseptic Processes, PDA.
- Michie, S., Atkins, L., & West, R. (2014). The behavior change wheel: A guide to designing interventions.
- Zheng, S, Yang, Q, Wang, X, Zhang, X, Zhou, Q. (2022) Capability, Opportunity, Motivation, and Hand Hygiene Behavior in Healthcare Workers: A Structural Equation Modeling. Psychol Res Behav Manag, 15:2219-2228.
- ICH (2008} Q8 (R2) Pharmaceutical Development, ICH.
- FDA (2011) Process Validation: General Principles and Practices, FDA.
- ICH (2019) Q12 Technical and Regulatory Considerations For Pharmaceutical Product Lifecycle Management, ICH.
- FDA (2023) CDER’s Quality Management Maturity (QMM) Program: Practice Areas and Prototype Assessment Protocol Development, FDA.
Author Details
Satish Joshi, Founder - SHJ Consulting Services; Ajay Pazhayattil, Management Consultant - cGMP World; Marzena Ingram, Sr. Pharmaceutical Consultant – Validant; Mava Fakoori, Behavioral Counselor and Therapist.
Satish Joshi is a distinguished figure and renowned consultant in the pharmaceutical industry with over 28 years of experience. He is the founder of SHJ Consulting Services, providing GMP consulting services. Having held senior leadership roles, including Senior Vice President of Quality Assurance at Hospira, Orchid Healthcare as VP of Quality, Dr. Reddy’s, and Lupin, Satish has excelled in various functions like QA, Compliance, QC, Analytical Development, and Packing Development. His expertise extends to successfully navigating regulatory inspections from agencies such as USFDA, MHRA, TGA, ANVISA, Taiwa,n, and GCC. Notably, Satish is recognized for his pivotal role in setting up Greenfield projects and establishing robust Quality procedures and systems. He is committed to excellence and strategy, contributing significantly to the industry’s adherence to compliance and quality standards.
Dr. Ajay Pazhayattil is a seasoned management consultant and an industrial pharmacist with experience in the industry’s sterile, solid oral, and API sectors. He is the founder of cGMPWorld and a founding partner at Itaan Pharma, an injectable manufacturer. He has been in leadership roles with North American pharmaceutical brands, generics, and CDMOs, including VP QA, Scientific & RA at Capcium, and Quality Director at Eurofins, Asso. Director at Apotex, etc. Ajay plays a key role in assisting organizations to navigate compliance and remediation efforts arising from FDA 483s and WL scenarios. He has been the lead author and contributor for industry guidance documents, including PDA, ISPE, AAPS, and RAPS. With a blend of technical acumen, strategic vision, and operational experience, Ajay continues to make significant industry contributions.
Marzena Ingram is an accomplished independent senior pharmaceutical consultant. She brings to the table a wealth of experience in quality and technical operations and process validation. At the forefront of her responsibilities is the critical task of addressing FDA warning letter scenarios for clients, ensuring compliance and regulatory adherence. Her strategic leadership and meticulous attention to detail have enabled her to spearhead compliance programs and initiatives meeting global regulatory requirements and to set new benchmarks in the industry. She has developed and led specialized teams at high-volume manufacturing organizations. Marzena serves as the Vice President of the International Society for Pharmaceutical Engineering (ISPE) Canada. She plays a pivotal part in shaping the industry’s future, contributing to the advancement of pharmaceutical science and fostering collaboration among professionals.
Mava Fakoori is a highly skilled psychotherapist, holding a Master of Arts in Clinical Psychology. With a deep understanding of cultural nuances shaping adherence and viewpoints, Mava’s clinical psychotherapy practice encompasses children, adults, older adults, couples, families, and the LGBTQ community. Specializing in psychoanalytic and somatic therapy, Mava brings a unique perspective to her counseling approach. She navigates the complexities of cognitive and behavioral elements to influence positive outcomes. As an experienced therapist, Mava provides comprehensive care beyond traditional modalities. Beyond her clinical work, Mava is a captivating voice in behavioral psychology. She hosts engaging shows on two radio stations and contributes insightful articles to “Today’s Women” magazine. Actively involved in the Iranian Psychological Association of America (IPAA), Mava is committed to advancing the understanding of behavioral science and psychology for the well-being of a broad spectrum of individuals.
Publication Details
This article appeared in American Pharmaceutical Review:
Vol. 27, No. 2March 2024Pages: 14-18
Subscribe to our e-newsletter
Stay up to date with the latest news, articles, and events. Plus, get special
offers from American Pharmaceutical Review delivered to your inbox!
Sign up now!