By: Dr. Akshaya. S1, Postgraduate, Department of Respiratory Medicine, Dr. Harish Ram Abilesh KR2, Senior Resident of Pharmacology, Dr. S. Brigida1, Associate Professor, Pharmacology, Dr Tanuja Lella1, Associate Professor, Pharmacology, G. Vishnu Priya1, Associate Professor, Pharmacology, Dr. Arul Amutha Elizabeth. L1, Professor & Head of Department of Pharmacology, Corresponding Author.
1Sree Balaji Medical College and Hospital, Chrompet Chennai Tamilnadu India, 2Bharath Medical College
Abstract
Introduction: Chronic obstructive pulmonary disease (COPD) is a progressive and severe respiratory disorder marked by airflow restriction and persistent symptoms, which considerably diminishes quality of life and lung function. Long-acting muscarinic antagonists (LAMAs), such as glycopyrronium and tiotropium, are often used in conjunction with long-acting β2-agonists (LABAs), including formoterol. This research evaluates the efficacy of glycopyrronium and formoterol in enhancing lung function and overall health status.
Methods: A prospective, open-label comparison research was performed with 100 individuals diagnosed with moderate to severe COPD. Patients received either GFF or TFF for a duration of 24 weeks. Evaluations were performed at baseline, 12 weeks, and 24 weeks.
Results: GFF treatment demonstrated a substantial improvement in FEV1% and FEV1/FVC ratios over 24 weeks relative to baseline, accompanied by improved symptom management as shown by decreased CAT scores. The GFF group had more fast and consistent improvements in lung function and patient-reported outcomes than the TFF group. Both therapies were well tolerated, with minor sideeffects.
Conclusion: Glycopyrronium-formoterol shown greater clinical efficacy in enhancing pulmonary function and quality of life in COPD patients compared to tiotropium-formoterol. These data corroborate the clinical efficacy of GFF as a valuable adjunct treatment in the management of COPD.
Keywords: Chronic obstructive pulmonary disease, COPD assessment test, Formoterol, Glycopyrronium, Tiotropium
Introduction
Chronic obstructive pulmonary disease (COPD) describes several conditions that irreversibly compromise lung function. These illnesses comprise emphysema, characterized by the destruction of the alveolar walls of the lungs, and prolonged bronchitis (WHO, 2022). The World Health Organization states that COPD is the third foremost cause of mortality around the globe, affecting 65 million individuals and resulting in over 3 million deaths annually. Around 90 percent of the death rate is predicted to occur in low – to middle-income countries (WHO, 2021). This illness ranks as the second foremost cause of mortality and disability-adjusted life-years in India (Salvi et al., 2018), with 55.23 million recorded cases of COPD and a prevalence of 3.63%, as per the 2017 Global Burden of Illness Report (Celli et al., 2022; Huang et al., 2019).
India has a significant population of symptomatic COPD patients, with low survival rates among those with severe COPD. The incidence and mortality of this illness are anticipated to rise further in the next decades (Koul et al., 2019; Koul et al., 2017). The clinical features of COPD include dyspnea on exercise, cough, and increasing impairment. Treatment approaches are mostly palliative and aimed at preventing more harm from infection (WHO, 2021). Tobacco smoking is regarded as the primary threat to the emergence of COPD. Nonetheless, just 10-20% of the smoking population gets COPD. Additional risk factors, including asthma, low socio-economic status, and lung infections in non-smokers, contribute to around 25-45% of COPD cases (Almagro et al., 2024).
Environmental variables, including occupational exposure to dust particles, biomass fuel, and gases and vapors emitted by industry, are often associated with the induction of COPD in low-income nations. Furthermore, exposure to hazardous gasses at various life stages has been shown to contribute to the development of COPD (Mirza et al., 2018; Pérez-Rubio et al., 2019). Multiple risk factors have been linked to COPD, including cigarette smoking, occupational exposures, and advancing age. The slow progression of COPD means that most exposures, including occupational hazards, biomass smoke, and cigarette smoking, need time to precipitate the disease. Significantly, intersections between the hallmarks of aging and the cellular mechanisms of COPD have been documented, suggesting that normal aging may act as a facilitator of COPD (Kukrety et al., 2018; Alfahad et al., 2021).
The therapy of COPD seeks to mitigate symptoms, boost pulmonary function, decrease exacerbation frequency, and improve patients’ overall quality of life. Bronchodilators, including long-acting muscarinic antagonists (LAMAs) and long-acting beta-2 agonists (LABAs), are fundamental in the treatment of COPD; their combination can yield synergistic effects by addressing distinct pathways related to bronchoconstriction and airflow restriction (Prada et al., 2024). The justification for combination treatment is based on its ability to provide superior bronchodilation, better symptom management, and decreased risk of exacerbations relative to monotherapy. Glycopyrronium is a muscarinic antagonist with a significant affinity for M1 receptors, subsequently for M3, M2/M4, and M5 receptors (Khan et al., 2023).
Glycopyrronium causes bronchodilation and reduces secretions from salivary and sweat glands by obstructing acetylcholine’s action on muscarinic receptors in the airway smooth muscle. This method is advantageous in controlling illnesses such as COPD since it lowers airway resistance and improves lung function (Drug Bank, 2024). In contrast, formoterol acts as a long-acting beta-agonist (LABA) with a fast onset, activating intracellular adenyl cyclase to transform adenosine triphosphate (ATP) into cyclic adenosine monophosphate (cAMP). Increased cyclic AMP levels induce the relaxation of bronchial smooth muscle, promoting bronchodilation and enhancing airflow in diseases including asthma and COPD (Prada et al., 2024).
The combination of glycopyrronium and formoterol synergistically enhances their effects, providing an effective strategy for controlling respiratory disorders. The anticholinergic effects of the glycopyrronium specifically target receptors associated with bronchoconstriction and secretions, while the beta-2 agonist action of formoterol promotes bronchodilation by increasing cyclic AMP generation (Salvi et al., 2022). This combined medication offers a successful approach to managing moderate-to-severe COPD by simultaneously targeting bronchoconstriction and airway inflammation (Jayanthi et al., 2022).
The pharmacotherapy for COPD comprises three primary categories of medications: anticholinergic agents, inhaled beta-2 agonists, and inhaled corticosteroids. The Global Initiative for COPD now recommends the combination of long-acting beta-agonists (LABAs) and long-acting muscarinic antagonists (LAMAs) for patients with COPD (Montuschi and Ciabattoni, 2015). The combination of LABA and inhaled corticosteroids has shown its efficacy in individuals with bronchial asthma (Shameem et al., 2014). COPD-specific HRQoL (Health-related quality of life) evaluations exist, including the St. George’s Respiratory Questionnaire (SGRQ) and the Chronic Respiratory Questionnaire (CRQ), however, some need excessive time for clinical administration.
Consequently, GOLD recommends the use of the COPD assessment test (CAT) or the modified British Medical Research Council (mMRC) dyspnea scale. The CAT is preferred above others since it provides a thorough assessment of the impact of COPD on well-being (Burkhardt and Pankow, 2014). The CAT is extensively used to evaluate respiratory symptoms and health-related quality of life in individuals with COPD. This questionnaire comprises eight items: the initial four relate to respiratory symptoms, specifically cough, sputum production, chest tightness, and dyspnea, while the subsequent four examine the disease’s influence on daily life, including activities of daily living, confidence in leaving the house, sleep quality, and energy levels (Koul et al., 2019).
The CAT is often provided to patients in the stable phase (Gupta et al., 2014); however, it has also been used during exacerbations in a few trials (Rassouli et al., 2017; Correa-Gutiérrez et al., 2024). Comparing CAT scores during stable phases and exacerbations allows for the assessment of deterioration in each patient for every exacerbation. Exacerbations serve as a prognostic indicator in COPD patients, as those with a history of previous exacerbations often have reduced survival compared to those without such a history (Soler-Cataluña et al., 2022). This study aims to analyze the comparative effectiveness of Glycopyrronium against Tiotropium as an adjunct to Formoterol treatment in COPD patients at a tertiary care hospital, with patient health status evaluated using the CAT score from baseline to 24 weeks.
Materials and Methods:
Study Design and Participants:
This is an open-label, randomized, prospective study and its aims of the COPD evaluation are to ascertain the extent of airflow limitation, its impact on the individual’s health, and the probability of future episodes, which will eventually inform treatment decisions.
| GOLD 1 | Mild | FEV1 ≥ 80% predicted |
| GOLD 2 | Moderate | 50% ≤ FEV1 < 80% predicted |
| GOLD 3 | Severe | 30% ≤ FEV1 < 50% predicted |
| GOLD 4 | Very Severe | FEV1 < 30% predicted |
The research included newly diagnosed patients with Chronic Obstructive Pulmonary Disease (COPD) aged 35 and older, categorized into groups with mild to severe COPD according to the GOLD standards. Patients were not included if they were pregnant or lactating, had been diagnosed with heart defects (including heart rhythm disorders, cardiac arrest, or coronary artery disease), impaired kidney function, a history of pulmonary surgeries or a history of allergic reactions to any one of the study medications. Participants might be withdrawn from the research if the experimental treatment failed to produce anticipated outcomes, in cases of adverse drug responses, non-compliance, or if the individual opted to withdraw for personal reasons.
Subsequent to the endorsement from the Institutional Ethics Committee (Ref No: 002/SBMCH/IHEC/2022/1794), the research was executed in compliance with the sanctioned protocol, informed consent mandates, and the ICH-GCP standards at Sree Balaji Medical College and Hospital. Eligible patients were randomly allocated into two equal groups of 50 by a simple block randomization technique. Group 1 was administered with 9 mcg of glycopyrronium and 4.8 mcg of formoterol at a dosage of two puffs twice daily for 24 weeks, while Group 2 got 9 mcg of tiotropium and 6 mcg of formoterol following the same dosing regimen. Subsequent to group allocation, the treatment protocol was started and maintained for a duration of four weeks. Patients were thereafter monitored at the 12th and 24th weeks for physical, general, and systemic examinations to determine clinical improvement and therapeutic response.
Sample size:
The total sample size of the study was 100 patients, determined by prior research and the prevalence of COPD. The sample size was computed using the formula:
n = 2[Zσ/E]²,
where n represents the sample size in each group, Z signifies 1.96 (for a 95% confidence interval), σ indicates the sample standard deviation, and E denotes the permissible error rate.
Screening and Procedures:
The screening procedure was conducted according to protocol, including a thorough clinical examination, an extensive medical and pharmaceutical history, and laboratory assessments including ECHO, chest X-ray, ECG, liver function test (LFT), and renal function test (RFT). Following the evaluation of 160 patients, 100 individuals were selected according to the inclusion criteria. They were thereafter provided with comprehensive information on the research design, possible risks, and benefits of the study drugs. Prior to the inclusion of each patient in the investigation, the protocol was elucidated to them, and their informed permission was acquired in writing in their native language. They were assured that their care at this facility would remain unchanged should they decide to withdraw from the study. Prior to their enrolment in the study endeavour, patients were mandated to complete baseline examinations.
Conduct of Spirometry:
Pulmonary function was evaluated using centralized spirometry. The device was pre-configured with anticipated reference values in compliance with the research protocol and the standards established by the American Thoracic Society (ATS) and European Respiratory Society (ERS). To reduce variability, the same spirometry apparatus was used continuously throughout the investigation. Whenever feasible, the same staff member administered and oversaw the evaluations during each patient visit. The spirometer was calibrated daily before use to guarantee measurement accuracy and dependability. Subsequent to screening, all patient data was documented on Case Record forms and preserved by the investigator.
Statistical Analysis
This research grouped patients receiving Glycopyrronium + Formoterol (GFF – MDI, 9 mcg/4.8 mcg) at two puffs twice daily as Group 1, whereas those administered Tiotropium + Formoterol (TFF – MDI, 9 mcg/6 mcg) at two puffs twice daily were classified as Group 2. Continuous variables were summarized with mean and standard deviation (SD), and comparisons among the two groups were conducted by the independent Student’s t-test. Categorical variables were represented as percentages and examined using the Chi-square test. A p-value below 0.05 was considered to be statistically significant.
Result and Discussion
Demographic Characteristics Age Distribution
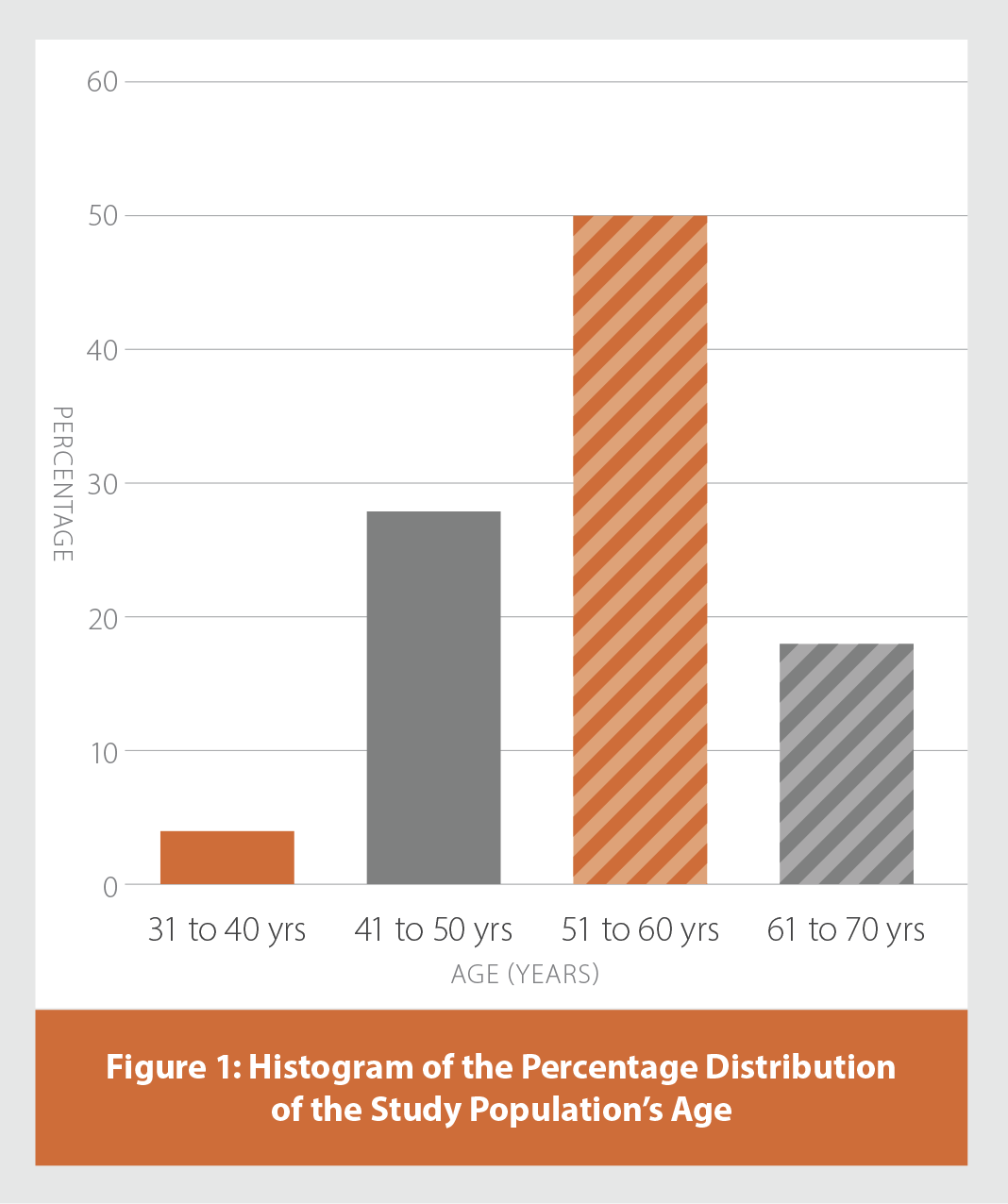
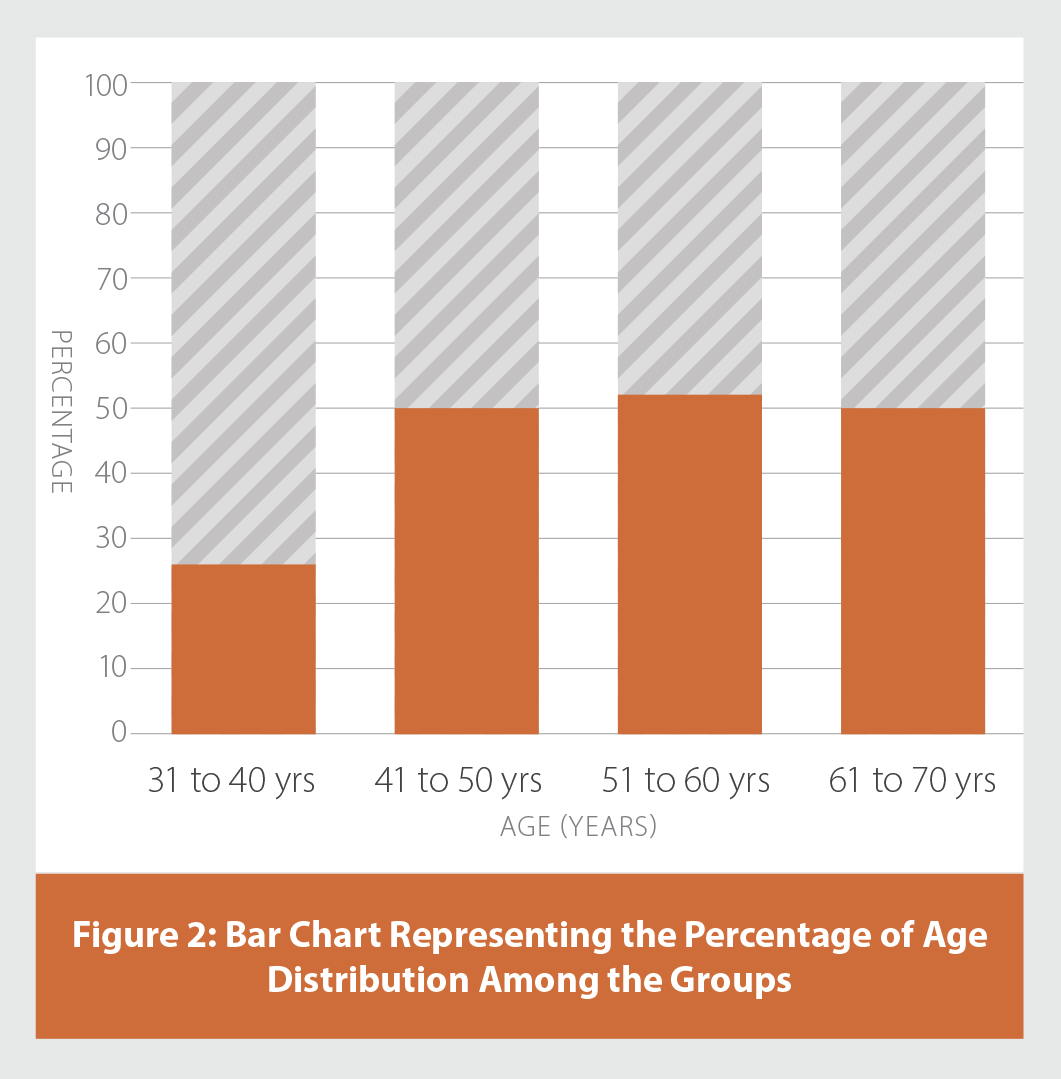
The study population (n=100) comprised both male and female participants, ranging in age from 38 to 65 years. Age distribution analysis revealed that the predominant segment of participants (50%) was within the 51–60 years age group. The age range of 41–50 years included 28% of participants. Individuals aged 61–70 constituted 18% of the sample, while just 4% belonged to the youngest age group of 31–40 years as shown in Figure 1. The mean age of participants in the GFF group was 54.24 ± 6.27 years, while that in the TFF group was 53.12 ± 6.71 years. Pearson’s Chi-square test showed no statistically significant difference in age distribution between the groups (p = 0.77), confirming that randomization effectively achieved demographic balance (Table 1 and Figure 2).
| Table 1: Comparison of Age Between the Groups by Pearson's Chi-Square Table |
|---|
| AGE | | GROUPS | TOTAL | X2 VALUE | P-VALUE |
|---|
| GFF | TFF |
|---|
| 31-40 yrs | Count | 1 | 3 | 4 | 1.08 | 0.78 |
| % | 2% | 6% | 4% |
| 41-50 yrs | Count | 14 | 14 | 28 |
| % | 28% | 28% | 28% |
| 51-60 yrs | Count | 26 | 24 | 50 |
| % | 52% | 48% | 50% |
| 61-70 yrs | Count | 9 | 9 | 18 |
| % | 18% | 18% | 18% |
| Total | Count | 50 | 50 | 100 | | |
| % | 100% | 100% | 100% | | |
| # No statistical significance at p > 0.05 level |
Gender Distribution
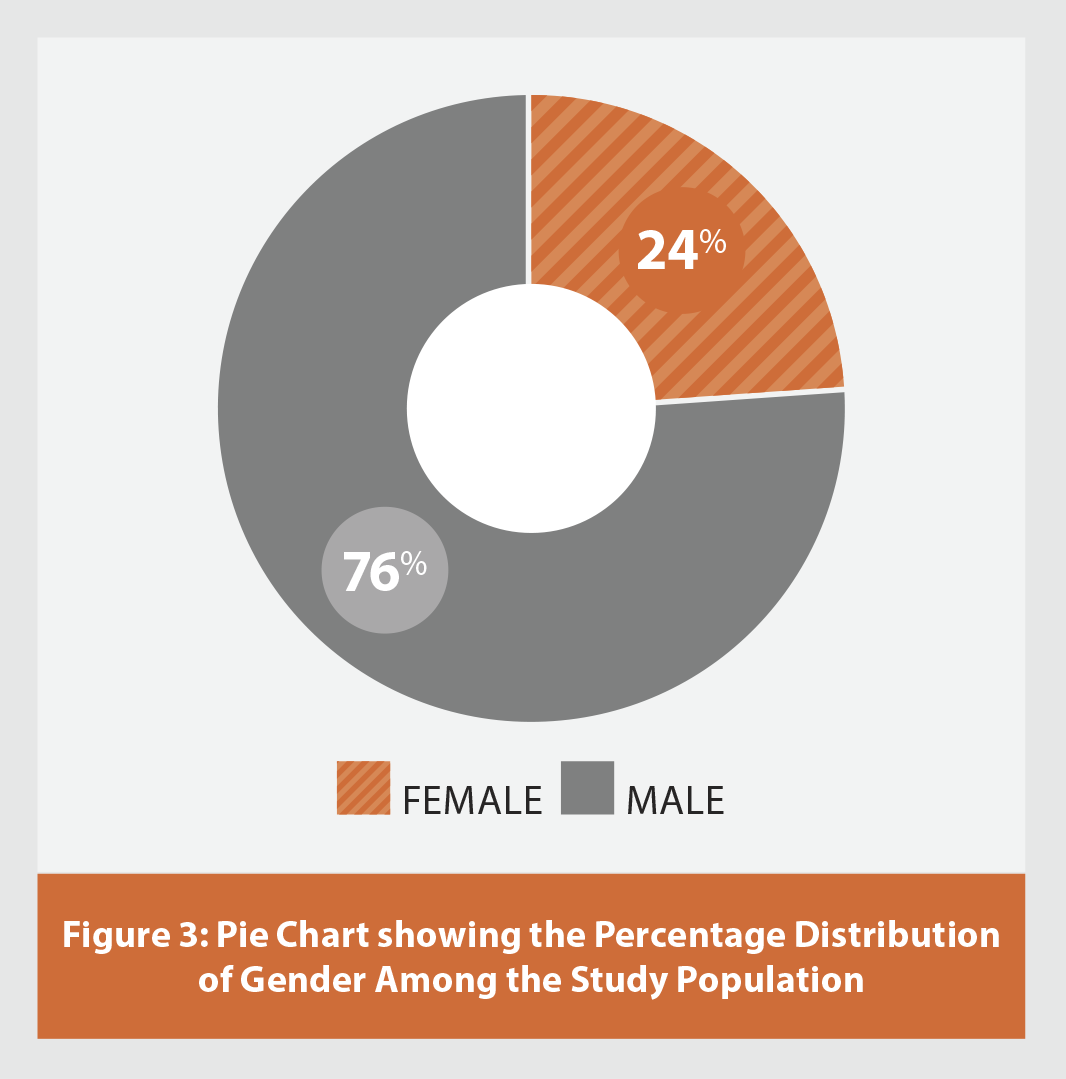
Among the 100 patients, 76% were male and 24% were female as illustrated in Table 2 and Figure 3. The gender distribution was comparable across the GFF and TFF groups, with no statistically significant difference shown by Pearson’s Chi-square test (Table 3). This reinforces the internal coherence of the research design. In all categories, the number of male participants exceeded that of female ones. No statistically significant difference was seen between the groups.
| Table 2. Gender Distribution Among the Study Population |
|---|
| GENDER | FREQUENCY | PERCENTAGE |
|---|
| Female | 24 | 24 |
| Male | 76 | 76 |
| Total | 100 | 100 |
Spirometry
Pulmonary function was evaluated using spirometry at baseline, 12 weeks, and 24 weeks in the Glycopyrronium/Formoterol (GFF-MDI) therapy cohort. The main spirometric metrics examined were FEV₁% (Forced Expiratory Volume in 1 second, % anticipated) and the FEV₁/FVC (Forced Vital Capacity) ratio, both essential for diagnosing and assessing the severity of COPD. Initially, the GFF group had a mean FEV₁% of 51% ± 10.06, which rose to 58% ± 11.46 at 12 weeks and subsequently to 66% ± 11.46 at 24 weeks as shown in Table 4. This indicates a consistent and clinically significant improvement in pulmonary function across the 24-week duration. The mean FEV₁/FVC ratio increased from 0.47 ± 0.06 at baseline to 0.52 ± 0.06 at 12 weeks, ultimately reaching 0.62 ± 0.05 at the conclusion of the study (Table 4).
The spirometric enhancements indicate a favorable bronchodilator response and enhanced airway mechanics in individuals administered GFF. Despite the research failing to show a statistically significant difference in FEV₁% or FEV₁/FVC relative to the TFF group, the numerical enhancement seen in the GFF group substantiates its therapeutic advantage. Salvi et al., (2022) indicated that glycopyrronium/formoterol inhalation treatment improved both spirometric measurements and patient-reported outcomes in Indian individuals with moderate-to-severe COPD. The fast effect and prolonged bronchodilation associated with glycopyrronium are ascribed to its superior receptor binding affinity and expedited pulmonary distribution, in contrast to tiotropium (Ahmad et al., 2024).
| Table 3: Comparison of Gender among the study population by Pearson's Chi-Square test |
|---|
| GENDER | | GROUPS | TOTAL | X2 VALUE | P-VALUE |
|---|
| GFF | TFF |
|---|
| Female | Count | 11 | 13 | 24 | 0.218 | 0.64 # |
| % | 22.00% | 26.00% | 24.00% |
| Male | Count | 39 | 37 | 76 |
| % | 78.00% | 74.00% | 76.00% |
| Total | Count | 50 | 50 | 100 | | |
| % | 100% | 100% | 100% | | |
| # No statistical significance at p > 0.05 level |
The observed enhancements in the FEV₁/FVC ratio align with prior studies, including the PINNACLE and GLOW trials (Miravitlles et al., 2014), which similarly indicated that glycopyrronium-based dual bronchodilators can provide effective airflow reversal and sustained symptom management (Martinez et al., 2017).
| Table 4: Mean And SD Changes of FEV1 and FEV1/FVC Ratio |
|---|
| TREATMENT | GROUPS | N | FEV1 | FEV1/FVC RATIO |
|---|
| MEAN | SD | MEAN | SD |
|---|
| Baseline | GFF | 50 | 51 | 10.06 | 0.47 | 0.05 |
| TFF | 50 | 51 | 9.85 | 0.4 | 0.06 |
| 12 weeks | GFF | 50 | 58 | 20.29 | 0.5 | 0.05 |
| TFF | 50 | 56 | 18.11 | 0.5 | 0.05 |
| 24 weeks | GFF | 50 | 66 | 11.46 | 0.6 | 0.04 |
| TFF | 50 | 63 | 10.92 | 0.59 | 0.05 |
COPD Assessment Test Score
The CAT score was used to assess quality of life and symptom load. Initially, the GFF group had a mean CAT score of 28.54 ± 3.59, which drastically decreased to 16.73 ± 3.31 by week 24. The TFF group had a baseline score of 26.86 ± 3.71, which declined to 19.22 ± 4.37 by week 24 (Table 5). The disparity between groups was statistically significant (p < 0.05), indicating enhanced symptom management and improved health status in the GFF group. The findings align with Cazzola et al., (2022), who indicated enhanced patient-reported outcomes with glycopyrronium-based regimens. This discovery reinforces the larger comprehension that dual bronchodilation enhances patient-reported outcomes more effectively than monotherapy.
The GFF combination has shown enhanced amplitude and rapidity of symptom alleviation, presumably because to glycopyrronium’s more rapid beginning of action relative to tiotropium (Salvi et al., 2022). The decrease in CAT scores within our GFF group surpassed the clinically significant threshold of ≥2 points as per the GOLD recommendations, underscoring the tangible advantages of this combination in enhancing health-related quality of life. Furthermore, Jayanthi et al., (2023) shown that patients administered glycopyrronium-formoterol saw more significant enhancements in lung function and health status ratings than those treated with tiotropium-formoterol, hence supporting our results.
Although both treatments were well-tolerated, the numerically superior improvement in the GFF group may indicate enhanced patient adherence, attributed to a lower incidence of bothersome side effects such as dry mouth and urinary retention, which are more commonly associated with tiotropium (Ahmad et al., 2024). These observations underscore the need of incorporating patient-reported outcome measures, such as the CAT, into clinical assessment and treatment strategies. They further emphasize the need of personalized treatment in COPD care, prioritizing symptom profiles, tolerability, and quality of life indicators in conjunction with spirometric parameters. In conclusion, whereas both GFF and TFF therapy yielded clinical enhancements, glycopyrronium + formoterol shown more significant decreases in CAT scores and a somewhat superior safety profile, making it a potentially more advantageous choice for the long-term management of moderate-to-severe COPD.
| Table 5: Mean Differences of CAT Scores Between Groups Before and After Treatment |
|---|
| CAT SCORE | GROUPS | N | MEAN | SD | T-VALUE | P-VALUE |
|---|
| Baseline | GFF | 50 | 28.54 | 3.59 | 2.3 | 0.02 * |
| TFF | 50 | 26.86 | 3.71 |
| 24 weeks | GFF | 50 | 16.73 | 3.31 | 2.07 | 0.04 * |
| TFF | 50 | 19.21 | 4.36 |
| * Statistically significant at p < 0.05 level |
Conclusion
This open-label, prospective, randomized trial evaluated the efficacy and safety of Glycopyrronium/Formoterol (GFF) vs Tiotropium/Formoterol (TFF) as adjunct treatments in patients with moderate to severe COPD over a 24-week duration. Patients administered GFF had a much higher decrease in CAT scores by week 24, indicating superior symptom management and quality of life compared to those receiving TFF. A significant enhancement in health status, as shown by the COPD Assessment Test (CAT) score, was seen in the GFF group relative to the TFF group, implying enhanced symptom alleviation and quality-of-life advantages with GFF treatment. The results suggest that the Glycopyrronium/Formoterol combination is at least as efficacious as the Tiotropium/Formoterol regimen and may be more suitable for those who are sensitive to the adverse effects linked to tiotropium. Due to its clinical performance, safety, and improvements in patient-reported outcomes, the GFF combination may be regarded as a feasible and perhaps superior option for the long-term therapy of moderate to severe COPD. These results underscore the use of the CAT questionnaire as a sensitive and pragmatic instrument for evaluating patient-reported outcomes and indicate that the GFF regimen may provide enhanced symptom alleviation and tolerability in the therapy of COPD.
References
- Ahmad J, Ahmad S, Ahmad F, Ahmad Z, Khan DI, Pandey V. SAFETY AND EFFICACY OF FORMOTEROL/TIOTROPIUM BROMIDE AND FORMOTEROL/GLYCOPYRRONIUM COMBINATION IN COPD WITH GOLD GRADE 3 PATIENTS. 2024.
- Alfahad AJ, Alzaydi MM, Aldossary AM, Alshehri AA, Almughem FA, Zaidan NM, Tawfik EA. Current views in chronic obstructive pulmonary disease pathogenesis and management. Saudi Pharmaceutical Journal. 2021 Dec 1;29(12):1361-73.
- Almagro P, Soler-Cataluña JJ, Huerta A, González-Segura D, Cosío BG, CLAVE Study Investigators. Impact of comorbidities in COPD clinical control criteria. The CLAVE study. BMC pulmonary medicine. 2024 Jan 2;24(1):6.
- Burkhardt R, Pankow W. The diagnosis of chronic obstructive pulmonary disease. Deutsches Ärzteblatt International. 2014 Dec 5;111(49):834.
- Cazzola M, Page C, Rogliani P, Calzetta L, Matera MG. Dual bronchodilation for the treatment of COPD: from bench to bedside. British Journal of Clinical Pharmacology. 2022 Aug;88(8):3657-73.
- Celli B, Fabbri L, Criner G, Martinez FJ, Mannino D, Vogelmeier C, Montes de Oca M, Papi A, Sin DD, Han MK, Agusti A. Definition and nomenclature of chronic obstructive pulmonary disease: time for its revision. American journal of respiratory and critical care medicine. 2022 Dec 1;206(11):1317-25.
- Correa-Gutiérrez CA, Ji Z, Domínguez-Zabaleta IM, Plaza-Hoz J, Gorrochategui-Mendigain I, López-de-Andrés A, Jiménez-García R, Zamorano-León JJ, Puente-Maestu L, de Miguel-Díez J. Deterioration Patterns in Patients Admitted for Severe COPD Exacerbation. Diseases. 2024 Nov 7;12(11):283.
- Gupta N, Pinto LM, Morogan A, Bourbeau J. The COPD assessment test: a systematic review. European Respiratory Journal. 2014 Sep 30;44(4):873-84.
- https://go.drugbank.com/drugs/DB00983
- Huang X, Mu X, Deng L, Fu A, Pu E, Tang T, Kong X. The etiologic origins for chronic obstructive pulmonary disease. International journal of chronic obstructive pulmonary disease. 2019 May 27:1139-58.
- Jayanthi N, Krishnan K, Sudhir M, Girija S, PA N. Comparative study on the effectiveness of glycopyrrolate/formoterol versus tiotropium/formoterol in patients with chronic obstructive pulmonary disease. Contemporary Clinical Trials Communications. 2022 Aug 1;28:100931.
- Khan KS, Jawaid S, Memon UA, Perera T, Khan U, Farwa UE, Jindal U, Afzal MS, Razzaq W, Abdin ZU, Khawaja UA. Management of chronic obstructive pulmonary disease (COPD) exacerbations in hospitalized patients from admission to discharge: a comprehensive review of therapeutic interventions. Cureus. 2023 Aug 18;15(8).
- Koul PA, Dar HA, Jan RA, Shah S, Khan UH. Two-year mortality in survivors of acute exacerbations of chronic obstructive pulmonary disease: a North Indian study. Lung India. 2017 Nov 1;34(6):511-6.
- Koul PA, Nowshehri AA, Khan UH, Jan RA, Shah SU. Cost of severe chronic obstructive pulmonary disease exacerbations in a high burden region in North India. Annals of global health. 2019 Jan 22;85(1):13.
- Kukrety, S.P., Parekh, J.D., Bailey, K.L., 2018. Chronic obstructive pulmonary disease and the hallmarks of aging. Lung India: Official Organ of Indian Chest Soc. 35, 321–327.
- Martinez FJ, Fabbri LM, Ferguson GT, Orevillo C, Darken P, Martin UJ, Reisner C. Baseline symptom score impact on benefits of glycopyrrolate/formoterol metered dose inhaler in COPD. Chest. 2017 Dec 1;152(6):1169-78.
- Miravitlles M, Beeh KM, Altman P. Glycopyrronium for chronic obstructive pulmonary disease: evidence and rationale for use from the GLOW trials.: 1095-1111.
- Mirza S, Clay RD, Koslow MA, Scanlon PD. COPD guidelines: a review of the 2018 GOLD report. InMayo Clinic Proceedings 2018 Oct 1 (Vol. 93, No. 10, pp. 1488-1502). Elsevier.
- Montuschi P, Ciabattoni G. Bronchodilating drugs for chronic obstructive pulmonary disease: current status and future trends. Journal of medicinal chemistry. 2015 May 28;58(10):4131-64.
- Pérez-Rubio G, Córdoba-Lanús E, Cupertino P, Cartujano-Barrera F, Campos MA, Falfán-Valencia R. Role of genetic susceptibility in nicotine addiction and chronic obstructive pulmonary disease. Revista de investigación clínica. 2019 Feb;71(1):36-54.
- Prada BS, Jadhav U, Ghewade B, Wagh P, Karnan A, Ledwani A, PRADA Jr BS, JADHAV U. Comparing Glycopyrronium/Formoterol Combination Therapy With Monotherapy in Moderate-to-Severe Chronic Obstructive Pulmonary Disease (COPD): A Narrative Review. Cureus. 2024 Apr 20;16(4).
- Rassouli F, Baty F, Stolz D, Albrich WC, Tamm M, Widmer S, Brutsche MH. Longitudinal change of COPD assessment test (CAT) in a tele healthcare cohort is associated with exacerbation risk. International journal of chronic obstructive pulmonary disease. 2017 Oct 24:3103-9.
- Salvi S, Kumar A, Agrawal S, Leuva A, Shukla VK, Deshpande SV, Balamurugan S, Singh A, Tikkiwal S, Gupta SK, Singh BP. Efficacy and safety of glycopyrronium/formoterol delivered via a dry powder inhaler in patients with moderate to severe chronic obstructive pulmonary disease: results from a multi-centre, open-label, randomised study. Lung India. 2022 Sep 1;39(5):408-16.
- Salvi S, Kumar GA, Dhaliwal RS, Paulson K, Agrawal A, Koul PA, Mahesh PA, Nair S, Singh V, Aggarwal AN, Christopher DJ. India State-Level Disease Burden Initiative CRD Collaborators. The burden of chronic respiratory diseases and their heterogeneity across the states of India: The Global Burden of Disease Study 1990–2016. Lancet Glob Health. 2018;6(12):e1363-74.
- Shameem M, Akhtar J, Ahmad A, Ahmad J. Efficacy of Fixed dose combination of Formoterol and Fluticasone propionate dry powder inhaler (DPI), in management of Partly controlled & Uncontrolled asthma in 5-17 yr Group. Int J Sci Res. 2014;3(5):415-8.
- Soler-Cataluña JJ, Piñera P, Trigueros JA, Calle M, Casanova C, Cosío BG, López-Campos JL, Molina J, Almagro P, Gómez JT, Riesco JA. [Translated article] Spanish COPD guidelines (GesEPOC) 2021 update. Diagnosis and treatment of COPD exacerbation syndrome. Archivos de bronconeumologia. 2022 Feb 1;58(2):T159-70.
- World Health Organization (WHO). Chronic obstructive pulmonary disease (COPD) world health organization. Geneva, Switzerland. 2022.
Subscribe to our e-Newsletters
Stay up to date with the latest news, articles, and events. Plus, get special
offers from American Pharmaceutical Review delivered to your inbox!
Sign up now!