Hibreniguss Terefe- Director, Product Development, Ardena; Stephen Csernica- Manager, Product Development, Ardena
Oral drug delivery remains the most preferred route of administration due to its convenience, cost-effectiveness, and high patient compliance. However, conventional immediate-release (IR) formulations often result in fluctuations in plasma drug concentrations, necessitating frequent dosing and potentially causing side effects due to peak-to-trough variations. Modified release (MR) formulations have been developed to address these challenges by controlling the rate and/ or site of drug release, thereby enhancing therapeutic efficacy and patient adherence.1
MR systems are a cornerstone of modern pharmaceutical development, offering sophisticated solutions to complex therapeutic challenges. They can be broadly categorized into delayed-release and extended-release formulations. Delayed-release systems release the drug at a time other than immediately after administration, often targeting specific regions of the gastrointestinal (GI) tract to protect the drug from degradation, protect the stomach from the drug, or deliver the drug to a local site of action. Extended-release systems, on the other hand, allow for a gradual, slow release of the drug over an extended period, which maintains therapeutic drug levels while reducing dosing frequency.2 This article provides a comprehensive overview of the design rationale, core technologies, development challenges, and regulatory considerations for solid oral MR systems. It highlights the integration of physiologically based pharmacokinetic (PBPK) modeling as a transformative tool and explores the critical role of MR formulations in advancing patient-centric therapy and life cycle management.
The Rationale for MR Formulations
The primary clinical benefit of MR systems is their ability to smooth out the sharp peaks and troughs in plasma concentration seen with IR drugs. This precise control leads to several therapeutic improvements, including reduced dosing frequency, minimized dose-related side effects, and enhanced efficacy by maintaining drug levels within the optimal therapeutic window.3-5 For example, metoprolol succinate extended-release tablets provide consistent 24-hour blood pressure control with a single daily dose, improving both therapeutic outcomes and patient compliance compared to its IR counterpart.6
These clinical improvements translate directly into a better patient experience. A simplified once-daily regimen significantly enhances convenience, making it easier for patients, particularly those with chronic conditions or complex medication schedules, to adhere to their treatment. This improved adherence leads to better disease management and, consequently, a higher quality of life.
Beyond the patient benefits, MR formulations are a vital tool for managing the pharmaceutical life cycle. Developing an MR version of an existing drug can secure new patent protection, extending market exclusivity long after the original compound’s patent has expired.7 This strategy also serves to differentiate a product in a competitive marketplace.8 The development of once-daily venlafaxine ER, for instance, provided a distinct advantage over the twice- or thrice-daily IR formulation, preserving market share against generic competition.9
Development Considerations
Designing a successful MR formulation requires a deep, integrated understanding of the drug’s intrinsic properties and the intended therapeutic profile. These factors dictate the technological approach and ultimate viability of the product.
The journey begins with the active pharmaceutical ingredient (API). The Biopharmaceutics Classification System (BCS) is a critical framework, with Class I (high solubility, high permeability) and Class II (low solubility, high permeability) drugs being the most suitable candidates. For Class II drugs, controlling the release rate can ensure that dissolution does not become a bottleneck for absorption. Furthermore, the API’s stability across the varying pH environments of the GI tract is paramount; unstable compounds may need protective enteric coatings to prevent degradation10,11
A drug’s pharmacokinetic profile determines if it can benefit from an MR system. Drugs with short biological half-lives (2-8 hours) are ideal, as an MR formulation can extend their therapeutic duration and reduce dosing frequency.12 Conversely, drugs with an inherently long half-life may not need it. Equally important is the site of the drug’s absorption. An API with a “narrow absorption window,” meaning it is only absorbed in the upper GI tract, requires specialized platforms like gastroretentive systems to prolong contact time at the site of absorption.13
Designing the desired release profile is a fundamental aspect of MR formulation. Different therapeutic goals require distinct release patterns:
- Zero-Order Release: This ideal release profile delivers the drug at a constant rate, maintaining steady plasma concentrations over the dosing interval. This is particularly desirable for medications with narrow therapeutic indices, where maintaining consistent drug levels is critical to maximize efficacy and minimize toxicity.14
- First-Order Release: In this pattern, the drug release rate decreases over time, often aligning with the natural elimination rate of the medication. This profile is suitable for drugs where a gradual decrease in plasma concentrations over time is acceptable or even beneficial.15
- Biphasic Release: This sophisticated release profile combines an IR phase, providing a rapid onset of therapeutic effect, followed by an extended-release phase for sustained action. This combination is highly beneficial for conditions requiring both quick relief and prolonged therapeutic maintenance (such as sickle cell disease, severe mental illnesses, or inflammatory bowel disease), allowing for a more nuanced approach to drug delivery.16
Classification of Solid Oral MR Systems
Solid oral MR systems are categorized by their distinct mechanisms for controlling drug release within the GI tract. The optimal system selection depends on the properties of the drug, the desired pharmacokinetics, and the therapeutic objectives.
Matrix Tablets
Matrix tablets are simple, widely used MR systems where the drug is dispersed within a polymer matrix. Release occurs either through the diffusion of the dissolved drug within the matrix or by the erosion of the matrix itself. Types include hydrophilic matrices (e.g., HPMC) that swell to form a gel, controlling diffusion, and hydrophobic matrices (e.g., ethylcellulose) where the drug dissolves and diffuses through insoluble polymer networks.
Reservoir Systems
These systems encapsulate a drug core within a rate-controlling polymeric membrane, with drug release primarily by diffusion across this membrane. The membrane’s thickness and permeability dictate the release profile. Reservoir systems offer consistent, predictable, and often first-order release. However, a significant limitation is the risk of “dose dumping” if the membrane is compromised, resulting in rapid and uncontrolled release. Manufacturing is also more complex than matrix tablets.
Osmotic Drug Delivery Systems (ODDS)
ODDS achieves highly controlled drug release using osmosis. They consist of a drug and osmotic agent core within a semi-permeable membrane with a laser-drilled orifice. Water enters the tablet, creating pressure that pushes dissolved drug out of the orifice at a controlled, steady rate. ODDS are highly valued for achieving zero-order release, largely independent of GI pH, motility, and food, ensuring high reproducibility.
Multiparticulate Systems
Multiparticulate systems comprise numerous small, discrete units (such as pellets or beads) individually coated to control drug release, which can be encapsulated, compressed, or used as sprinkles. Each unit acts as a mini-delivery system, with release controlled by the properties of its coating (diffusion, erosion, and pH).
Ion-Exchange Resins
These systems use insoluble polymers with ionizable groups to formulate complex drugs, releasing them through ion exchange in the GI tract. The drug, typically an ionizable compound, binds electrostatically to the resin and is displaced by GI ions (e.g., H+, Na+), with release influenced by ionic strength and pH.
Gastroretentive Drug Delivery Systems (GRDDS)
GRDDS prolongs the dosage form’s residence time in the stomach, benefiting drugs with narrow upper GI absorption windows or those that are active in the stomach. Strategies include floating systems (low density), mucoadhesive systems (adhering to mucosa), and swelling systems (expanding to prevent pyloric passage).
Pulsatile Systems
Pulsatile systems release drugs in bursts after a defi ned lag time, which is valuable for chronotherapy synchronized with circadian rhythms. Approaches include time-dependent coatings, pressure-sensitive and enzymatically triggered systems, and capsule-within-capsule devices.
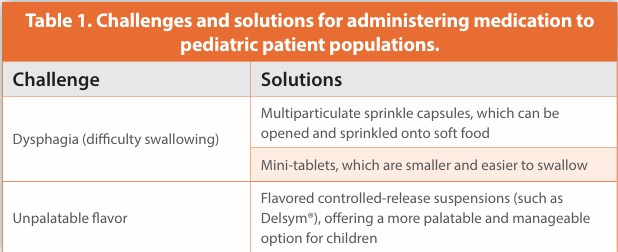
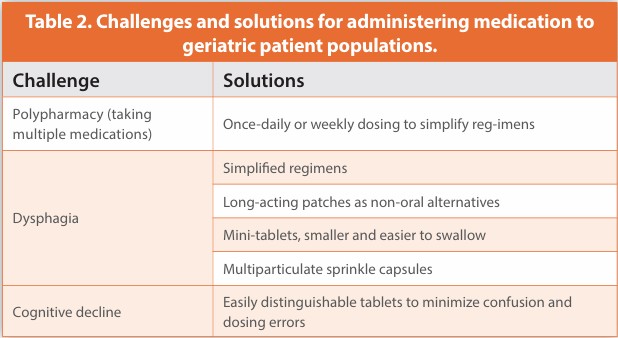
Patient Centricity Issues in Pediatrics and Geriatrics
The success of MR formulations is intrinsically linked to their usability across diverse patient populations. Designing drug delivery systems with patient needs at the forefront is crucial for optimizing adherence and therapeutic outcomes.
Prioritizing patient-centric design in MR formulation development leads to tangible benefits. These include improved adherence and persistence with prescribed therapies, which is vital for long-term disease management. Also, well-designed MR systems contribute to reduced dosing errors, ultimately promoting a better quality of life and therapeutic satisfaction for patients and enhancing their overall treatment experience.17,18
Regulatory Evaluation and Lifecycle Management
A cornerstone of regulatory approval for MR formulations is the establishment of in vitro–in vivo correlation (IVIVC). This correlation demonstrates the predictive value of dissolution data obtained from laboratory tests, showing how in vitro drug release profiles can predict in vivo pharmacokinetic behavior. Such correlations are crucial for validating the robustness of the formulation. For generic MR formulations, bioequivalence studies are typically required to demonstrate that the generic product performs comparably to the reference listed drug in terms of rate and extent of absorption. Additionally, stability testing is crucial to ensure that the drug product maintains a consistent release profile, chemical integrity, and overall quality throughout its intended shelf life under various environmental conditions.
Pharmaceutical companies strategically utilize MR formulations as a key component of product lifecycle management. By developing MR versions of existing drugs, companies can lay claims to new intellectual property, effectively extending patent protection and providing continued market exclusivity. This approach can breathe new life into established products nearing patent expiration. Furthermore, reformulations that incorporate advanced drug delivery systems can justify premium pricing, facilitate targeting niche indications, differentiate the product in a competitive market, and optimize its commercial value.
Regulatory bodies, such as the U.S. Food and Drug Administration (FDA), provide comprehensive guidance on extended-release oral dosage forms. These guidelines outline the essential data required for approval, including performance under both fed and fasted states to assess the impact of food on drug absorption.19 Special attention is also given to evaluating the effects of alcohol on dose dumping. In this critical safety concern, alcohol consumption could lead to an unintended rapid release of the entire drug dose, potentially resulting in adverse effects and toxicity. Adherence to these guidelines is paramount for navigating the complex regulatory landscape and securing market approval.
Targeted GI Delivery and Narrow Window Drugs
Tailoring drug release to specific regions of the GI tract is a sophisticated strategy employed by MR systems to optimize therapeutic outcomes, especially for drugs with unique absorption characteristics. Certain medications are absorbed primarily in specific regions of the GI tract due to localized transporters, pH-dependent solubility, or unique enzymatic conditions. For these compounds, systemic bioavailability is directly influenced by the precise site of drug release. MR technologies can be meticulously designed to deliver the API at optimal GI locations, thereby improving therapeutic performance, reducing dosing frequency, and mitigating potential systemic side effects, ensuring the drug is available where and when it is most effective.20
Drugs characterized by a narrow absorption window are typically absorbed primarily in the stomach or the upper portion of the small intestine. These include crucial medications such as levodopa, riboflavin, and gabapentin. For such drugs, controlled positioning within the GI tract is essential to ensure adequate absorption and achieve the desired therapeutic levels.
For drugs intended to act locally in the colon (e.g., for inflammatory bowel diseases such as ulcerative colitis or Crohn’s disease) or for systemic absorption primarily via the colon, pH-dependent delayed release systems are highly beneficial. These systems are designed to bypass metabolism or degradation in the upper GI tract, releasing the drug only when it reaches the higher pH environment of the ileo-colonic region. Many physiological and pathological conditions, such as asthma, hypertension, and arthritis, exhibit distinct circadian rhythms, with symptoms peaking at specific times of the day. Pulsatile delivery systems are specifically designed to align drug release with these biological rhythms, optimizing therapeutic effects when they are most needed.
Leading the New Generation of Therapeutics
MR drug delivery systems continue to redefine the landscape of solid oral formulations, offering significant advantages in therapeutic control, patient adherence, and pharmaceutical innovation. A comprehensive understanding of the drug’s physicochemical and pharmacokinetic properties is crucial for designing a successful MR formulation. When paired with robust in vitro characterization and physiologically based pharmacokinetic modeling, development efforts become more predictable, cost-efficient, and streamlined. Moreover, MR systems support patient-centric care by improving treatment tolerability and reducing pill burden, particularly in pediatric and geriatric populations. As drug development increasingly emphasizes personalization, MR systems — especially those informed by in silico modeling — are expected to lead the next generation of oral therapeutics.
References
- Lubrizol Life Science Health. The Guide to Oral Extended Release Tablets. 2023.
- Kumar V, et al. Matrix tablets: an important tool for oral controlled-release dosage forms. J Drug Deliv Ther. 2011;1(2):27–31.
- Rathbone MJ, Hadgraft J, Roberts MS. Modified-Release Drug Delivery Technology. Informa Healthcare; 2003.
- Jantzen GM, Robinson JR. Sustained- and controlled-release drug delivery systems. In: Modern Pharmaceutics. Marcel Dekker; 1995. p. 501–528.
- Torrey Pines Law Group. Pharmaceutical Lifecycle Management. 2023. https:// torreypineslaw.com
- Rowe RC, Sheskey PJ, Quinn ME. Handbook of Pharmaceutical Excipients. 6th ed. Pharmaceutical Press; 2009.
- Thombre AG, Cardinal JR. Osmotic drug delivery systems. In: Medical Applications of Controlled Release. CRC Press; 1995. p. 203–227.
- Dukić-Ott A, Vervaet C, Remon JP. Immediate and controlled drug delivery using ion exchange resins. Expert Opin Drug Deliv. 2009;6(12):1143–1155.
- Hwang SJ, Park H, Park K. Gastric retentive drug delivery systems. Crit Rev Ther Drug Carrier Syst. 1998;15(3):243–284.
- Ueda S, et al. Development of a novel oral dosage form for chronotherapy. Int J Pharm. 1994;111(1):1–8.
- Maroni A, Zema L, Cerea M, Sangalli ME. Oral pulsatile drug delivery systems. Expert Opin Drug Deliv. 2005;2(5):855–871.
- Jones HM, et al. Physiologically based pharmacokinetic modeling in drug discovery and development. Clin Pharmacokinet. 2006;45(5):511–542.
- Heimbach T, et al. Application of PBPK modeling to support drug product development: case studies and strategies. J Pharm Sci. 2019;108(9):2624–2634.
- Darwich AS, et al. The impact of gastrointestinal transit on drug absorption: PBPK modeling of complex oral drug delivery systems. Adv Drug Deliv Rev. 2017;112:3–18.
- US FDA. Guidance for Industry: Physiologically Based Pharmacokinetic Analyses — Format and Content. (“Federal Register: Physiologically Based Pharmacokinetic Analyses ...”) 2018. https://www.fda.gov
- Wagner C, et al. Predicting the effect of food on oral drug absorption: application of PBPK modeling. Mol Pharm. 2016;13(9):3301–3311.
- Agyilirah GA, Green M, Ducret R. Evaluation of gastric retention properties of a crosslinked polymer-coated tablet. Int J Pharm. 1991;75(2-3):241–247.
- Colombo P, et al. Drug release modulation by physical restrictions of matrix swelling. Int J Pharm. 2000;202(1-2):137–145.
- FDA. Guidance for Industry: Extended Release Oral Dosage Forms: Development, Evaluation, and Application of In Vitro/In Vivo Correlations. 1997.
- Dressman JB, Reppas C. In vitro–in vivo correlations for lipophilic, poorly water-soluble drugs. Eur J Pharm Sci. 2000;11:S73–S80.
Author biographies
Hibreniguss Terefe is Director of Product Development at Ardena US in Somerset, NJ, where he leads the development of solid oral dosage forms from early-stage through commercial manufacturing. He joined Ardena in 2024 after serving as Director of R&D at Catalent Pharma Solutions. With over 25 years of pharmaceutical R&D and academic experience, he has held leadership roles at ExxPharma Therapeutics and the University of Asmara. His expertise includes drug delivery systems, solubility enhancement, modified-release formulations, and hot melt extrusion. He holds a PhD in Pharmaceutical Chemistry from the University of Münster and was a Fulbright Scholar at UC Berkeley.
Stephen Csernica is Manager of Product Development at Ardena US in Somerset, NJ, where he works to provide clients with rational and scientific solutions to their drug development challenges from early-stage through commercial manufacturing. He joined Ardena (formerly Catalent Somerset) in 2021 after previous roles at Impax Laboratory and Leading Pharma. Steve has 11 years of industrial solid oral formulation development experience, including complex controlled release formulations and solubility enhancement techniques, and has experience in all stages of product development, from pre-clinical to scale-up and registration manufacturing. Steve holds a PhD in Chemical Engineering from Lehigh University.
Subscribe to our e-Newsletters.
Stay up to date with the latest news, articles, and events. Plus, get special
offers from American Pharmaceutical Review delivered to your inbox!
Sign up now!