Abstract
Background
Clinical research continues to have unmet needs specific to the enrollment of diverse patient populations that match real-world populations. Current research is unclear about whether offering clinical research remotely, meaning participants do not have to travel to a study center, would increase the willingness of minority groups to participate in such research. The objective of this study was to determine if potential participants from Black or African American communities or rural areas would be more willing to participate in clinical research if it were conducted remotely.
Methods
A cross-sectional, observational study was conducted utilizing an electronic self-administered survey with data from adult patients in the United States from a company-proprietary database to assess their willingness to participate in a clinical trial if it was offered remotely. Data collected included demographics, questions with Likert-type responses specific to remote clinical trial design, and participants' perceived benefits and challenges of remote clinical trials. The survey was available for 10 days from August 22, 2023, through August 31, 2023, via a secure online link available to invited participants only.
Results
The survey yielded 757 completed surveys. The mean age of participants was 61 years (SD: 13 years), 53% (n=404) were female, 80% (n=603) were White, and 37% (n=279) lived in an urban setting. Most participants, 65% (n=491) never participated in a clinical trial. The Black or African American participant population had the highest percentage, 80% (n=31) of respondents who were much more willing to participate in a clinical trial if offered remotely. A Kruskal-Wallis rank sum test yielded a statistically significant difference between race and willingness to participate in a clinical trial if offered remotely. A further pairwise test was run to observe differences between races and yielded statistically significant results. The statistically significant observed difference was between white or Caucasian and Black or African American respondents. There were no statistically significant differences across groups when analyzed by living setting.
Conclusion
Overall, patients are much more willing to participate in a clinical trial if it is offered remotely. The primary research hypothesis that Black or African American respondents are more willing to participate in decentralized/remote clinical trials than white or Caucasians is supported. However, the secondary research hypothesis that respondents living in a rural setting would be more willing to participate in a decentralized/remote clinical trial than those in a city or urban setting is not supported. Researchers should leverage remote clinical trials further to increase participation rates and diversity in clinical research.
Introduction
Clinical research benefits the global population through health advancements, yet less than 5% of the world’s population has ever participated in a clinical trial.1 This type of research is critical to providing new therapies and improving the standard of care for patients across the world. Clinical trial enrollment rates have historically been low, suggesting there are barriers to entry for the patient population. The data collected in these trials do not typically reflect actual data from real-world populations and reflect an underrepresentation of racial/ethnic minorities, rural areas, and elderly populations.2
For example, the United States (U.S.) makes up a little more than 4% of the world population, but it contains 35% of global clinical trial participants.1 The racial distribution of U.S. research participation does not match the existing U.S. racial population distribution, which is 58% White, 19% Hispanic, and 12% African American.3 However, U.S. research race distribution reflects 76% of all clinical trial participants being White, followed by 11% Asian, 7% Black, and the remaining 6% Other or American Indian.1
The data demonstrates the lack of a diverse clinical trial population that matches real-world populations, a deficiency that exists in clinical research. Proper research conduct requires representative participation that emulates the diversity of the world population to prevent bias in the research, maximize the validity of statistical data, and exploit the public health impact for affected populations of the disease being studied.
Why Diversity in Clinical Trials is Important and Increases Patient Confidence in Research
Disease and illness may impact diverse patient populations in separate ways. Ethnicity, age, and environmental factors may be correlated to disease risk, activity, or outcomes. For example, Black or African American populations are twice as likely to die from heart disease than white or Caucasian populations, heart disease risk also increases with age, and environmental factors, such as smoking, may also increase the risk of heart disease.4 This research data is an example of how heart disease risk may be influenced by diverse reasons such as race, age, or environmental effects. Therefore, to fully understand the impact of varied influences, research populations must reflect the diverse demographics of race, age, and geographical location where research occurs since these factors influence the disease outcomes.5
Diverse research populations allow drug examination across all subgroups of patients which results in the ability to assess differences in the disease outcomes for specific groups.6 Researchers may examine subgroups to provide the ability to compare incidence, prevalence, and mortality statistics across similar populations (age, race, gender) or geographical locations for the therapy being studied. As a result, study data will more closely reflect the population, making the results generalizable to identify correlations between subgroups, and more accurately predict outcomes by group. Establishing stronger statistical study data by increasing diversity in research may result in rising patient confidence in both the safety and efficacy of the drug being studied.7 Increased patient confidence in clinical research is a positive outcome that could increase a patient’s willingness to participate (WTP) in future clinical research. Therefore, clinical trial diversity is critical to advancing health and health equity across the world.
Clinical Trials Recruitment Gap
Existing research suggests that recruitment challenges are the direct result of clinical trial complexity and perceived patient burden which lead to scarce participation, limited participant pools, and minimal diversity in clinical research.8 Patient recruitment in clinical research is a continued challenge across the world. Under-enrollment, resulting from a lack of willingness for patients to participate in research and a lack of knowledge of clinical research being conducted, is the major reason for early termination of clinical trials with 19% of trials terminated because of not meeting enrollment requirements.9,10 If a study is unable to meet sample size requirements for recruitment, the study data will be unreliable and considered invalid.
Clinical trial participation demand is at an all-time high and has been growing exponentially over the last century due to the incorporation of research controls, regulatory requirements, and protection of study participants.9 Despite the increased demand, participation rates are not improving, creating a continued recruitment gap for active research.
There have been studies conducted to analyze why patients are not participating in clinical research and to determine the barriers of entry that may be preventing greater clinical trial participation. The primary barriers to participation across studies include common themes such as distrust of researchers, participation obstacles or resource constraints (time, cost, inconvenience), lack of clinical trial knowledge/awareness, complex clinical trial process (uncomfortable, limited information), or individual participant characteristics (age, race, beliefs).9,11
Patient trust is essential when it comes to health research participation. Patients must feel comfortable about decisions being made about their health and sharing information about their health. Unfortunately, patient distrust in the pharmaceutical industry has increased over the last decade and is contributing to lower participation in clinical research with only 48% of research participants declaring they trust pharmaceutical companies.12
Clinical research awareness is also limited. Patient communities are unaware of the research opportunities with only 59% of Americans reporting having knowledge or awareness of clinical trials.2 Clinicaltrials.gov has study information, but it often does not reach patient advocacy groups or the community due to the lack of knowledge that the information exists. Recent data from the NCIS Health Information National Trends Survey (HINTS) finds that only 9% of Americans have been invited to participate in a clinical trial, and of those invited, African Americans and individuals in rural areas had lower odds of being invited to participate in the research.2 To de-risk clinical trial recruitment to meet research targets, researchers must find successful ways to address these themes to increase both participation and diversity across clinical trials in a shorter timeline.
Reducing Patient Burden by Leveraging Technology to Increase Trial Participation
Researchers can make trial participation less burdensome by reducing the number of onsite visits required in a study, leveraging digital health tools to replace onsite visits, and leveraging home health nurses to visit participants in their homes.8 Reducing this burden may enhance research participation and accelerate recruitment by attracting more participants. Technology drives efficiency and productivity by reducing burdens in our daily lives and may also be used to reduce patient burdens in conducting research by replacing the need for onsite study visits.
Technology is already being leveraged to conduct electronic consent in patient trials, perform telehealth visits, and complete electronic clinical outcome assessments for both sites and patients which makes the research process more efficient for both investigators and patients.8 Technology enables researchers to put the patient at the center of the research and engage directly with the patient through technology utilizing mobile apps to communicate with the patient and collect patient data remotely. Studies show that direct-to-patient solutions resonate among racial and ethnic minority patients because they feel more comfortable with the direct engagement of healthcare providers.11 Mobile devices and wearables are tools that may be used to provide direct-to-patient solutions. Researchers may provide a mobile device to a patient who currently does not have one. Researchers may create mobile applications to conduct a trial virtually, provide education and training materials to patients electronically, and use the device to communicate with the patients more easily about the trial.
Digital health technology decreases the patient barriers to accessibility of research with more frequent communication and mobile technology reduces or eliminates travel to sites for research through virtual visits, in turn reducing patient burden.9,13 Leveraging technology in clinical research is a way to provide participants with more flexibility to reduce both the time and cost of trial participation while providing a tool to directly engage with patients.
Developing Decentralized Clinical Trials Technology that Provides Patient Value
Decentralized Clinical Trials (DCTs) are one way researchers may address the enrollment and diversity challenges in clinical research. DCTs leverage technology to conduct the clinical trial process and reduce the patient burden in clinical research. Studies reveal that 75% of patients prefer a DCT over traditional clinical trials and 80% of patients are more likely to participate in research if mobile technology is utilized.14
DCTs are a modern way to conduct clinical research using mobile technology and home health care providers by reducing or eliminating the need for study participants to visit a clinical site for study data collection. DCTs utilize technology to remotely collect the study data and directly engage with patients from any geographic location. This technology provides study participants increased flexibility with the ability to participate in a trial from the convenience of their own homes. A well-developed DCT solution or tool has proven to increase patient engagement and improve enrollment, retention, quality, and adherence in clinical trials.15 Improving enrollment and retention of clinical trials will reduce both the cost and time to market of developing an investigational product.16
Technology and biotech companies continue to develop DCT technology and digital tools to assist researchers in conducting clinical research remotely. Technology product success, including DCT technology, requires a value proposition for the end-user. Any technology development should incorporate the Technology Acceptance Model that a user’s perception of usefulness and ease of use does drive user participation of the product.17,18 For participants to adopt DCT technology, they must share the belief that the DCT they are participating in is useful and that the technology they use to participate in the DCT is easy to use. A survey is one way to capture the perception of technology, such as DCTs, to incorporate the feedback into the development of future DCT design. Including consumers and their perceptions in new product design offers numerous benefits.19 Involving patients in the design of DCTs is crucial to ensure that the study is convenient and reduces the time burden for the study participant. Patient input is believed to inform successful participant engagement in DCTs by aligning trial design to participant values and circumstances.20
Leveraging Decentralized Clinical Trials to Increase Diversity and Reduce Clinical Trial Enrollment Gap
Researchers may leverage DCT technology to directly address the existing enrollment gap and increase diversity across clinical trials. DCTs use technology to virtually enroll patients in clinical trials. Virtual enrollment can expand the pool of potential research participants asked to enroll, it may also increase enrollment by lowering the burden of participation and empowering more individuals to participate in clinical trials, thereby potentially improving diversity among research participants; virtual enrollment also enhances efficiency.21
DCTs represent better real-world data which also increases patient confidence regarding the safety and efficacy of the drug once approved.21 The use of telehealth technology in DCTs enables real-time video conferencing with patients and providers. Telehealth technology is proven to enhance communication and engagement with patients.21 Evidence suggests that telehealth technology improves access for patients residing in rural and remote areas, where distance to participate in trials acts as a barrier to their involvement.21 DCTs enable enrollment of these underserved and underrepresented populations in clinical research.22 Therefore, by leveraging DCTs, researchers can enrich patient engagement, and improve diversity and enrollment participation in clinical trials.
Study Objective
Researchers may leverage DCTs to address participation and diversity challenges. A barrier to entry specifically for DCTs is the lack of patient WTP in a DCT because of perceived burdens. Prior research evaluated a patient’s WTP in traditional clinical trials based on participant characteristics, which included gender, race, sex, and age. Existing studies have shown how DCTs can reduce the patient burden of clinical research. However, the research provides little evidence about which factors of a DCT influence the patients’ WTP and how these factors vary by participant characteristics.
The purpose of this study is to analyze patient perspectives on DCTs through a patient engagement survey for the company’s [name removed for confidentiality] clinical research group. The primary hypothesis is that Black or African American respondents are more willing to participate in decentralized/remote clinical trials than white or Caucasians. The secondary hypothesis is that respondents living in a rural setting would be more willing to participate in a decentralized/ remote clinical trial than those in a city or urban setting. The company [name removed for confidentiality] has confirmed a need to compare patient perceptions, barriers, and needs specific to DCTs. The company [name removed for privacy] will apply the study findings to improve existing enrollment and diversity deficiencies in clinical trials in their future DCT design.
Study Design
A cross-sectional, observational study design utilizing a survey was developed to collect data over 10 days to examine the relationship between WTP in a clinical trial if offered remotely, race, and living setting. The study aimed to provide researchers with valuable insights into the characteristics and associations of a sample patient population which may be used to inform future DCT design. The study was submitted to the Advarra Internal Review Board for approval and was deemed exempt as a market research survey.
A collaborative survey design session was conducted during the preliminary stages of the survey development. This session involved various business functions and incorporated insights from DCT leaders to ensure the survey design aligned with their needs. The session also focused on prioritizing research goals and conducting user testing to maximize the value of the survey. The design session included survey adjustments.
Study Population
A survey was used because the study required a large sample size and may be given to a diverse population of participants. To ensure the results are representative of the real-world population, the participants were randomly selected from a proprietary company patient screener database (approval received) based on statistical considerations to achieve the correct level of confidence in the results. The participants in the proprietary company database are individuals who opted in for potential clinical research participation across the U.S. with varying degrees of clinical research knowledge. The proprietary company screener application has a built-in survey tool to facilitate patient-based surveys and leverages the proprietary company patient database. The proprietary database contains a diverse population with demographic data that the patients shared during a previous screening process. This data enabled solicitation to a diverse participation pool. Survey eligibility for members of this proprietary panel included age ≥ 18 years and ability to read and understand English.
Participant Recruitment
Participants were invited to join the study via an email notification directly from the company’s built-in survey tool. The email contained the proprietary company logo so participants would know the email solicitation was valid and not a phishing email. The email was generically worded to prevent bias in the survey responses. The email contained a secured and proprietary link with access to the survey eligibility screen. Eligible respondents were then directed to an electronic informed consent. The survey was designed to take only five minutes to complete; participants were told in advance the time required to complete the survey. A survey link with a request to participate was emailed to 40,000 potential participants, and a follow-up reminder was sent a week later to non-responders.
The survey was self-administered and available for a 10-day period from August 22, 2023, through August 31, 2023, for participants to complete. Participation was voluntary and an incentive was given to encourage survey participation. The incentive was awarded to the first 25 survey participants as a $10 Amazon gift card which was distributed seven days after the initial launch of the survey.
Measures
The living setting was measured in the survey by city, urban, rural, or other option. Rural-Urban Continuum Codes (RUCC) were used to categorize survey participants’ area of residence using a three-level categorization. The first category, city, was defined as an area where the population is at least 50,000 people. This would include RUCC classifications of 1-3.23. The second category, urban, was defined as an area where the population is at least 2,500 but less than 50,000 people. The inclusion criteria incorporated RUCC for non-metropolitan classifications ranging from 4 to 7, regardless of their adjacency to a metropolitan area. The last category, rural, was defined as an area where the population is less than 2,500 people. The inclusion criteria incorporated RUCC for non-metropolitan classifications ranging from 8 to 9, regardless of their adjacency to a metropolitan area.
The survey was designed to measure the willingness of a patient to participate in a DCT and their attitude toward specific DCT components. The survey contained 16 total questions which included five nominal variables (gender, race, age, living setting, and previous clinical trial participation), nine ordinal variables (highest level of education and eight items to assess WTP in a clinical trial, using 5-point Likert-type response options ranging from 1-Much Less Willing, 2-Less Willing, 3-Neither, 4-More Willing, and 5-Much More Willing, and two items with an open-ended response on participant’s perceived benefits and challenges of remote clinical trials.
Pilot Survey
Prior to survey administration, a test was conducted by a team of diverse individuals on a small internal population to identify any potential issues with the survey and format. The testers identified areas where there could be ambiguity or confusion and adjustments were made. The pilot team validated that the survey was easy to understand to ensure it was interpreted correctly across the diverse population of participants.
The survey was administered ethically by providing participant consent before beginning the survey and the company ensured anonymity and confidentiality of all results. The survey provided an overview of the purpose of the study being conducted and provided participants with an option to receive summary survey results once the survey closed. The study team were the only individuals to have access to the survey data which was stored securely in the company's proprietary database and extracted only for statistical analysis purposes. The survey was closed ten days after the initial survey email was sent.
Statistical Analysis
The quantitative survey data was analyzed using descriptive statistics. The categorical variables were reported as mean frequencies and the scale variables were reported as mean and standard deviation (SD). Descriptive statistics were utilized with a split variable of race or living setting to investigate the associations between different variables. The inclusion of a split variable allowed for the examination of relationships between the WTP in a remote trial (scale variable) and race or living setting (categorical variable) that consists of more than two levels, by utilizing contingency tables.
The primary outcome of this research was evaluating the overall willingness of individuals to participate in a clinical trial when offered remotely. Survey items related to the participants’ WTP were analyzed, along with the seven items associated with the design of the remotely offered trial. The distribution of these eight items was assessed for the degree of missing data, skewness, kurtosis, and adherence to the assumptions of normality.
In cases where the data satisfy the underlying assumptions of normality, an Analysis of Variance (ANOVA) test was employed for the analysis. The ANOVA statistical method was chosen to test the hypothesis, as it allows for the comparison of means between distinct groups. This method provides valuable insights into any differences that may exist among the groups being compared, thereby determining the presence or absence of statistical significance.
However, in cases where the data failed to meet the underlying assumptions of normality, non-parametric statistical tests were utilized for the analysis. In such instances, the Kruskal-Wallis statistical method was employed to test the hypothesis. The Kruskal-Wallis method is a non-parametric test specifically designed to ascertain whether there are statistically significant differences between the medians of two or more independent groups.
Data is reported using a 95% confidence interval with a p-value of 0.05 for statistical significance. The historical completion rate, leveraging the company's proprietary survey tool, was 1%. The minimum target sample size, calculated with a power of 80% and a significance level (alpha) of .05 required for the Kruskal-Wallis, was N=385. Therefore, 40,000 survey invitations were sent to meet the enrollment goal. Descriptive statistics were evaluated and reported using JMP Pro version 17.0 (SAS Institute Inc.) and all non-parametric tests were conducted in Intellectus Statistics (Intellectus Statistics Inc.).
The open-ended questions regarding the perceived benefits and challenges expressed by the respondents were meticulously categorized using Microsoft Excel. The resulting themes were prioritized based on their frequencies and presented in descending order, from the most frequent to the least frequent. Additionally, an in-house AI tool was employed to analyze the open-ended responses and extract any relevant themes. This AI tool also generated a report on the frequencies of the identified themes, ranking them in descending order of occurrence.
Survey Participation
A total of 40,000 unique patients were invited to participate in the survey. Of the invited participants, 2,183 participants clicked on the link to the survey. Among those who clicked on the survey, 873 opted out, 553 provided partial data, and 757 completed the survey yielding a participation rate (n invitation/n clicked) of 5% and a completion rate (n completers/n of participants clicked) of 35% respectively (Figure 1).
Survey Participant Characteristics
Among the 757 survey completers (Table 1), the mean age of participants was 61 years (SD: 13 years); 404 (53%) were female, 603 (80%) were white or Caucasian, 279 (37%) live in an urban setting, and 224 (30%) have some college education with no degree. Most participants, 491 (65%) report never participating in a clinical trial.
The overall WTP in a clinical trial if offered remotely was 638 (84%). Respondents’ WTP in a clinical trial if offered remotely is presented in Table 2 by both race or living setting which excludes data responses of those less willing or much less willing to participate given there were 0 values for most of these selections. Black or African Americans had the highest percentage by race of reported WTP, 31 (79.5%), in a clinical trial if offered remotely. Patients living in a city had the highest population by living setting, 136 (58.9%), who were much more willing to participate in a clinical trial if offered remotely.
Survey Participants’ Overall Willingness to Participate in a Remote Clinical Trial
The study examined data by groups based on race and living setting. The data was ordinal and did not satisfy the underlying assumptions of normality; therefore, a non-parametric statistical test was conducted to compare different racial groups and determine which group was more willing to participate in a clinical trial if offered remotely. Also, the same test was run to compare living setting groups and determine which group was more willing to participate in a clinical trial if offered remotely. The distribution of survey participants completing the survey by race was not normally distributed. The majority of completed surveys were from white or Caucasian participants (Table 1). Several race categories weree significantly small samples, therefore, these were combined into a category called ‘other’ to ensure an adequate sample size for statistical analysis.
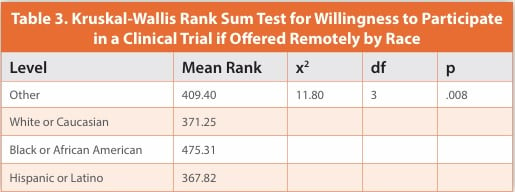
A Kruskal-Wallis rank sum statistical test was conducted to assess if there were statistically significant differences across racial groups and their WTP in a clinical trial if offered remotely. The results looking across racial groups demonstrated statistically significant differences (Table 3) between the racial groups based on an alpha value of .05.
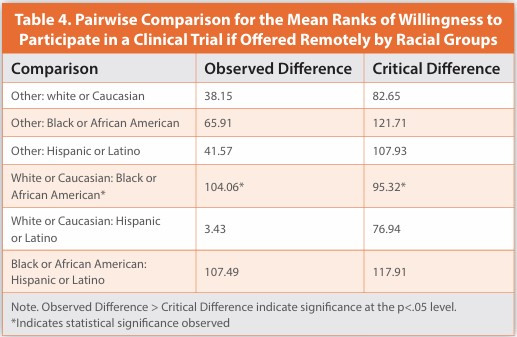
Additional examination was conducted by utilizing a pairwise comparison approach to further analyze the outcome. An exhaustive enumeration method was used by comparing all possible racial group combinations. The pairwise results again demonstrated statistically significant differences between the racial groups (Table 4) on WTP in a clinical trial if offered remotely. The statistically significant observed difference was between white or Caucasian participants compared to Black or African American participants. Therefore, the hypothesis that Black or African American (minority population) would be more willing to participate in a clinical trial if offered remotely than white or Caucasian (non-minority population) is accepted.
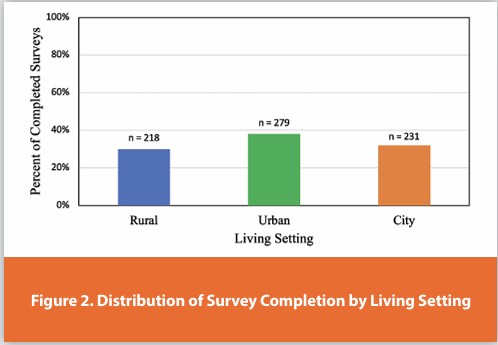
The distribution of survey participants who completed the survey by living setting were equally distributed. The majority of completed surveys were from participants living in an urban setting (Figure 2). Other living setting categories had a small sample size and were dropped from the analysis so it would not compromise the statistical results due to insufficient data.
A Kruskal-Wallis statistical test was conducted to assess if there were statistically significant differences across living setting groups and their WTP in a clinical trial if it was offered remotely. The results of the Kruskal-Wallis test looking across living setting groups demonstrated no statistically significant differences between the living setting groups and their WTP in a clinical trial if offered remotely. The results were based on an alpha value of .05, X2(2) = 2.46, p = .293, which indicates that the mean rank of WTP in a clinical trial if offered remotely was similar for each living setting. Therefore, the secondary hypothesis that respondents living in a rural setting would be more willing to participate in a decentralized/remote clinical trial than those in a city or urban setting is rejected.
Secondary Findings
The distribution of survey participants that completed the survey by gender had well-distributed participation. The majority of completed surveys were from female participants (Figure 3). The other gender category was dropped due to the small sample size (n = 2) to not compromise statistical analysis and focus on the two gender categories that are more relevant to this study.
A Kruskal-Wallis rank sum statistical test was conducted to assess if there were statistically significant differences across gender and their WTP in a clinical trial if it was offered remotely. The results of the Kruskal-Wallis rank sum test looking across gender groups demonstrated statistically significant differences (Table 5) between the gender groups based on an alpha value of .05.
Additional examination was conducted by utilizing a pairwise comparison approach to further analyze the outcome. An exhaustive enumeration was not necessary, as there was only one combination for comparing the two genders. The pairwise results again demonstrated statistically significant differences between the genders (Table 6) on WTP in a clinical trial if it was offered remotely. The statistically significant observed difference was between female participants compared to male participants.

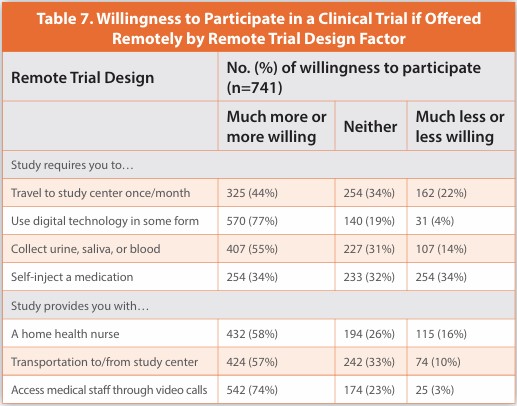
There were seven design factors on the WTP as a part of the survey (Table 7). The study requirements that influenced participants to be much more or more willing to participate in a remote clinical trial were studies that leverage the use of digital technology, 570 (77%), and when the study provides access to medical staff through video calls, 542 (74%). The study requirements that influenced participants to be much less or less willing to participate in a remote clinical trial were studies that required the participant to self-inject a medicine 254 (34%), followed by studies that required the participant to travel to a study center at least once a month, 162 (22%). These findings could be further analyzed to make predictions about future DCT participation behaviors by participant characteristics. This would provide further insight into DCT design and recommendations based on the predictive factors that may be identified through deeper analysis.
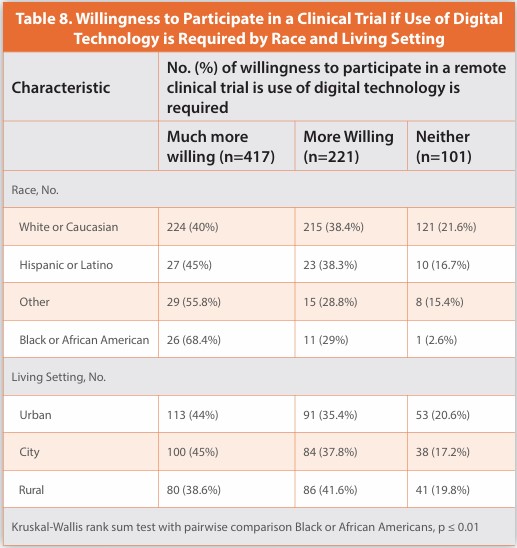
The remote trial design factors were then assessed by both race and living setting. Respondents’ WTP in a clinical trial if the study requires the use of digital technology in some form is presented in Table 8 by both race and living setting. Black or African Americans had the highest percentage by race of reported WTP, 26 (68%), in a clinical trial if the use of digital technology is required. Patients living in a city had the highest population by living setting, 100 (45%), who were much more willing to participate in a clinical trial if the use of digital technology was required.
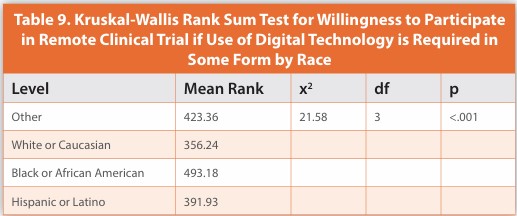
A Kruskal-Wallis rank sum statistical test was conducted to assess if there were statistically significant differences across race and WTP in a remote clinical trial and if it required the use of digital technology in some form to take part. The results of the Kruskal-Wallis rank sum test looking across race groups demonstrated statistically significant differences (Table 9) between the racial groups and their WTP in a remote clinical trial, based on an alpha value of .05 if digital technology use was required in some form as a part of the trial design.
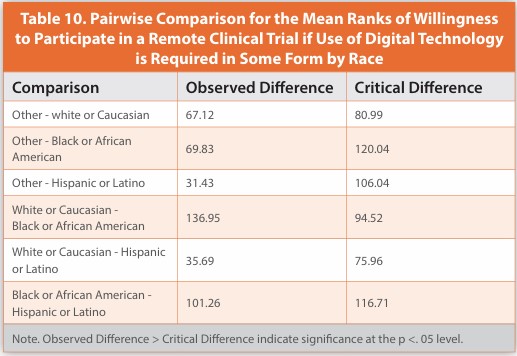
The additional examination was conducted by utilizing a pairwise comparison approach to further analyze the outcome. An exhaustive enumeration method was used by comparing all possible racial group combinations. The pairwise results again demonstrated statistically significant differences between the racial groups (Table 10) on WTP in a clinical trial if digital technology use was required in some form. The statistically significant observed difference was again between white or Caucasian participants compared to Black or African American participants.
A Kruskal-Wallis statistical test was conducted to assess if there were statistically significant differences across living setting groups and their WTP in a clinical trial if the use of digital technology is required. The results of the Kruskal-Wallis test looking across the living setting groups demonstrated no statistically significant differences between the living setting groups and their WTP in a clinical trial if the use of digital technology was required. The results were based on an alpha value of .05, x2(2) = 2.89, p = .236, which indicates that the mean rank of WTP in a clinical trial if the use of digital technology is required was similar for each living setting.
Overall Perceived Benefits of Participating in a Remote Clinical Trial
The open-ended portion of the survey on top perceived benefits of participating in a clinical trial was manually analyzed leveraging Excel. The result of the manual compilation revealed 6 emerging themes. The themes were analyzed by frequency by the top perceived benefits of a remote clinical trial. The emerging themes in order of frequency were societal or research benefit, time savings, convenience, personal health benefit, monetary benefit or cost savings, and further health educational benefit. There were a few individuals who noted that less stress, technology, fun, or free medication were a perceived benefit but were not as frequent.
In addition, data from the open-ended perceived benefit of a remote clinical trial was ingested into the company's proprietary platform that leverages artificial Intelligence (AI) technology, which can understand human-like text. The platform then processes the data to generate thematic results leveraging natural language processing (NLP), which allows the computer to make sense of the words it is ingesting and translate them into understandable human language. The results were very similar to the manual analysis but had some differences in the order of frequency and naming of the categories. The top 6 thematic data produced from the company's proprietary AI platform, in order of frequency, were improving health and finding cures, travel convenience and efficiency, benefits of remote clinical trials in the comfort of your home, helping others or self for future, benefit ts of new medication and better health, and convenience and timesaving in future trials.
Overall Perceived Challenges of Participating in a Remote Clinical Trial
The open-ended portion of the survey on top perceived challenges of participating in a clinical trial had eight emerging themes. The themes were analyzed by frequency by the top perceived challenges of a remote clinical trial. The emerging themes in order of frequency were time, limited support or face-to-face contact, quality/compliance, technology issues, side effects/adverse events, availability, cost, and self-collection of specimens. A few individuals noted that data security, receiving a placebo, or not meeting inclusion criteria were perceived challenges but were not as frequent.
The top challenges were also analyzed by leveraging the company's proprietary AI platform. The results were similar but had variances in topic title and order of frequency. The top eight themes emerging as analyzed from the company's proprietary AI platform, in order of frequency, were time/travel/scheduling, not knowing the outcome, internet/technology challenges, side effects, disqualification, challenges with remote participation compliance, challenges of being remote, and lack of involvement.
Discussion
The study findings support the hypothesis that the inclusion of a remote participation option in clinical trials will increase potential research participants' WTP. According to this study, which involved 757 participants, it has been revealed that most participants (84%) would be either much more willing or more willing to partake in a clinical trial if offered remotely. The finding is consistent with existing research that has shown that 75% of patients favor DCTs over traditional clinical trials.14 DCTs may provide a means to resolving some of the enrollment challenges by designing remote clinical trials that incorporate participant preferences. Understanding the factors that influence a participant’s WTP in a clinical trial is the first step to improving these patient enrollment challenges. Additionally, understanding that these preferences differ by both race and sex will enable researchers to customize future trial designs to improve the diversity of clinical trial participation.
The primary findings of the study show that there are statistically significant differences across races, specifically between Black or African American patients and white or Caucasian patients, WTP in a clinical trial if it is offered remotely. Given that the Black or African American population has been historically underrepresented in clinical research this is a meaningful finding. Overall, it is difficult to recruit for clinical research, but the ability to enroll Black or African American populations is more significant or attention-grabbing. So, while DTC technology can improve overall WTP, it also may specifically increase WTP in the Black or African American population that has been historically underrepresented due to lack of WTP. Furthermore, incorporating greater participation of diverse populations, including Black or African Americans, in clinical research endeavors has been empirically demonstrated to enhance comprehension and therapeutic approaches towards diseases, particularly when said diseases exhibit higher prevalence among diverse populations.6
There were no statistically significant differences observed between other racial groups. Clinical research has an underrepresentation of Hispanic or Latino populations as well. Further research would need to be conducted, through focus groups, specific to the Hispanic or Latino population to determine specific DCT design factors that may better appeal to that group and could potentially increase enrollment for these populations.
Enhancing statistical study data by augmenting diversity in research can lead to a boost in patient confidence in both the safety and efficacy of the drug being examined.7 Moreover, for diverse patients who have demonstrated low confidence in drug treatments due to insufficient data or lack of evidence of drug efficacy in specific populations, this strategy may enhance their confidence and potentially increase and improve treatment adherence for patients in diverse populations.
Existing research suggests that the complexity of the trial and perceived burden on the patient, contribute to enrollment challenges in clinical trials. This leads to limited participation, small participant pools, and a lack of diversity in clinical research.8 Although identifying a diverse patient population poses its challenges, even when these patients are identified, they may be hesitant to enroll due to the perceived burden and lack of trust. Therefore, given the survey results demonstrate patients perceive a lower burden when a DCT is utilized, it is expected that their WTP and enrollment rates will increase when a clinical trial is conducted remotely.
The study also found that there are no statistically significant differences based on a participant’s living setting and their WTP in a clinical trial if it is offered remotely. While we did not see a difference across living setting groups for their WTP in a clinical trial, it was observed that there was a diverse distribution of participants by living setting. The survey was leveraged utilizing digital technology. Other research indicates that recruitment of diverse populations across living settings is a challenge but given the use of digital technology was able to recruit a diverse population by living setting for survey participation, and there were no differences in WTP. The data indicate that remote clinical trials have the potential to enroll a population that is equally distributed across different living settings. Further research could be conducted to determine if there is a greater ability to recruit and reach more diverse populations by living settings using digital technology in clinical trials if offered remotely.
There were several secondary findings of the study. Prior research indicates that 80 clinical trial participants were more likely to participate if technology was utilized.14 In this study, 77 participants stated they are much more or more willing to participate in the remote trial if the use of digital technology is required in some form.
More specifically, the findings revealed statistically significant results that Black or African Americans are more willing to participate in a DCT than white or Caucasian if the DCT requires the use of digital technology in some form.
The technology acceptance model,18 The model helped identify the specific characteristics of DCTs, such as requiring the use of digital technology, video calls, and home health nurses. The technology acceptance model has been used to provide support and verification, and the results of this study will help the company’s DCT team operationalize this model efficiently into a direct-to-patient trial design. Time, money, and effort go into trial design, and designing trials to succeed is a key driver to promote and ensure enrollment targets are met quickly. Trials that are poorly designed and do not reach enrollment targets may end up being terminated prematurely.10
Prior research findings show associations between race and technology and attribute the association to increased study participant comfort when technology is employed.11 This study provides empirical evidence that the use of digital technology does increase the willingness of Black or African Americans to participate in clinical trials if offered remotely. The findings also confirmed that women are statistically more willing to participate in a clinical trial offered remotely than men. The secondary results will help researchers design future DCTs with digital technology requirements if their recruitment goal is to increase Black or African American participation. Researchers should also consider a DCT offering for clinical trials where the protocol requires a higher level of female participation.
Our survey demonstrates that participants do believe a remote clinical trial saves time, is more convenient, and has a monetary or cost savings benefit. Other research studies show existing barriers that are impacting enrollment in clinical trials and potential patients are unwilling to enroll due to time, cost, and inconvenience.9,11 DCTs are perceived to remove these barriers and in turn, would increase the ability to improve clinical trial enrollment. Additional research would need to be conducted to statistically prove the observed correlations. The ability to overcome participant-perceived barriers would improve the WTP, subsequently increasing the enrollment of these diverse populations in clinical trials.
Study Limitations
This study sought to investigate patient perceptions and attitudes towards DCTs using a cross-sectional survey design and a sample of participants recruited through a company-proprietary database. Despite efforts to increase response rates, such as random sampling of participants, selection criteria to target a diverse population, and monetary incentives, there were several limitations of this study and its design that should be considered when interpreting the results.
One of the main limitations of this study was the potential for sample bias due to the cross-sectional survey design. As such, the respondent population was not representative of the real-world population, with an overrepresentation of women (53%), white or Caucasian participants (80%), and elderly (mean age = 61). There was an underrepresentation of men (47%), Black or African Americans (5%), and young adults under 40 (7%). Given the low representation of Black or African Americans and the high representation of white or Caucasian respondents, this may have impacted the statistically significant finding between these two race groups on the WTP in a remote clinical trial. Future studies could employ sampling techniques, such as the oversampling of targeted populations, to increase response rates and participation from underrepresented groups.
Another limitation of this study was the potential for selection bias due to the use of a company-proprietary database to recruit participants. Respondents may have been previously screened for or educated about clinical trials, leading to a more positive attitude towards clinical trials and potentially producing more favorable survey results. Additionally, the survey had a limited scope that contained a narrow range of information specific to DCTs. This lack of a comprehensive scope could limit the understanding of DCTs for many participants.
Response bias was also a potential limitation of this study due to the differing levels of knowledge on what a clinical trial is and how remote clinical trials are conducted. This could lead to inaccurate responses that may be intentional or unintentional. To minimize information bias, additional research could be conducted using focus groups that provide a more comprehensive overview and education on DCTs.
Additionally, a monetary incentive was offered for the first 25 participants to complete the survey. While the incentive was only $10.00, it could still produce additional response bias by attracting a participant population with lower socioeconomic statuses. Future studies could consider alternative forms of incentives or none to minimize this potential limitation.
Lastly, given that a survey tool was leveraged for the survey, the study measured intent, not actual behavior. The assumption is that there is a direct connection between intent (responses on the survey) and actual behavior. This introduces a limitation given that there is not always a correlation between intent and behavior. So, just because a participant implies, they would be WTP in a DCT, does not imply they will participate in the DCT.
While this study provides valuable insights into patient perceptions and attitudes toward DCTs, it is important to consider the limitations of the study design and potential biases when interpreting the results. Future research should aim to address these limitations to provide a more comprehensive understanding of patient perceptions and attitudes toward DCTs.
Summary and Conclusion
DCTs have the potential to improve patient enrollment and diversity through patient-centric study design leveraging digital technology. DCTs can bridge the recruitment gap in researchers’ ability to quickly enroll a diverse research population and improve clinical trial design. Clinical trial participants are more willing to take part in a clinical trial if offered remotely. Remote clinical trials that require the use of digital technology or leverage video calls for study appointments have garnered significant interest.
Black or African American populations are more likely than the white or Caucasian populations to show more interest in a DCT if the use of digital technology is utilized. Women are also more likely than men to participate in a DCT. These considerations should be considered when developing study protocols with DCT designs to improve enrollment and diversity in trials. A more patient-centric approach in DCT design is only one factor for improving enrollment and diversity in clinical trials. More research should be conducted on a broader global population to better understand remote clinical trial preferences by region, race, sex, and even therapeutic area.
References
- 2015-2019 Drug Trials Snapshots Summary Report Five-Year Summary and Analysis of Clinical Trial Participation and Demographics. U.S. Food and Drug Administration. https:// www.fda.gov/media/143592/download. Published November 2020. Accessed April 30, 2024.
- Hints Brief 48: Clinical Trial Participation Among U.S. Adults. National Cancer Institute. https://hints.cancer.gov/docs/Briefs/HINTS_Brief_48.pdf. Published March Accessed April 30, 2024. 2022.
- Census: Racial and Ethnic Diversity in the United States: 2020 and 2010 Census. United States Census Bureau. https://www.census.gov/library/visualizations/interactive/racial and-ethnic-diversity-in-the-united-states-2010-and-2020-census.html. Published August 2021. Accessed April 30, 2024.
- African American Health. National Center for Chronic Disease Prevention and Health Promotion. Centers for Disease Control and Prevention. https://archive.cdc.gov/#/ details?url=https://www.cdc.gov/vitalsigns/aahealth/index.html. Published July 2017. Accessed April 30, 2024.
- Walker DM, Swoboda CM, Shiu-Yee K. et al. Diversity of Participation in Clinical Trials and Influencing Factors: Findings from the Health Information National Trends Survey 2020. J Gen Intern Med 2022. doi:10.1007/s11606-022-07780-2.
- Enhancing the Diversity of Clinical Trial Populations — Eligibility Criteria, Enrollment Practices, and Trial Designs Guidance for Industry. Regulations.gov. https://www. regulations.gov/document/FDA-2019-D-1264-0094. Published November 2020. Accessed April 30, 2024.
- Masters JC, Cook JA, Anderson G, et al. Ensuring diversity in clinical trials: The role of Clinical Pharmacology. Contemporary Clinical Trials. 2022;118:106807.
- Thakur S, Lahiry S. Digital clinical trial: A new norm in clinical research. Perspect Clin Res. 2021;12(4):184-8.
- Rodríguez-Torres E, González-Pérez MM, Díaz-Pérez C. Barriers and facilitators to the participation of subjects in clinical trials: An overview of reviews. Contemp Clin Trials Commun. 2021;23:100829.
- Carlisle B, Kimmelman J, Ramsay T, MacKinnon N. Unsuccessful trial accrual and human subjects protections: an empirical analysis of recently closed trials. Clin Trials. 2015;12(1):77–83.
- Clark LT, Watkins L, Piña IL, et al. Increasing Diversity in Clinical Trials: Overcoming Critical Barriers. Curr Probl Cardiol. 2019;44(5):148-72.
- Pahus L, Suehs CM, Halimi L, et al. Patient distrust in pharmaceutical companies: an explanation for women under-representation in respiratory clinical trials. BMC Med Ethics. 2020;21(1):72.
- Borno HT, Zhang L, Siegel A, Chang E, Ryan CJ. At What Cost to Clinical Trial Enrollment? A Retrospective Study of Patient Travel Burden in Cancer Clinical Trials. Oncologist. 2018;23(10):1242-9.
- Virtual Clinical Trials Market Size, Share & Trends Analysis Report by Study Design (Interventional, Observational, Expanded Access), by Indication (Oncology, Cardiovascular), by Region, and Segment Forecasts, 2022-2030. Research and Markets. https://www. researchandmarkets.com/reports/5415490. Published January 2022. Accessed April 30, 2024.
- Coyle J, Rogers A, Copland R, De Paoli G, MacDonald TM, Mackenzie IS. A secondary qualitative analysis of stakeholder views about participant recruitment, retention, and adherence in Decentralized Clinical Trials (DCTs). Trials. 2022;23(1):614.
- DiMasi JA, Smith Z, Oakley-Girvan I, et al. Assessing the Financial Value of Decentralized Clinical Trials. Ther Innov Regul Sci. doi:10.1007/s43441-022-00454-5.
- Walczak R, Kludacz-Alessandri M, Hawrysz L. Use of Telemedicine Technology among General Practitioners during COVID-19: A Modified Technology Acceptance Model Study in Poland. Int J Environ Res Public Health. 2022;19(17):10937
- Davis FD. Perceived Usefulness, Perceived Ease of Use, and User Acceptance Information Technology. MIS Quarterly. 1989;13(3):319-40.
- Costa C, Vale R. To tell or not to tell? The impact of communicating consumer participation in new product development. Journal of Product & Brand Management. 2018;27. doi:10.1108/JPBM-07-2016-1276.
- de Jong AJ, van Rijssel TI, Zuidgeest MGP, et al. Opportunities and Challenges for Decentralized Clinical Trials: European Regulators’ Perspective. Clin Pharmacol Ther. 2022;112(2):344-52.
- Orlando JF, Beard M, Kumar S. Systematic review of patient and caregivers’ satisfaction with telehealth videoconferencing as a mode of service delivery in managing patients’ health. PLoS One. 2019;14(8):e0221848.
- Moseson H, Kumar S, Juusola JL. Comparison of study samples recruited with virtual versus traditional recruitment methods. Contemp Clin Trials Commun. 2020;19:100590.
- Cromartie, John. Rural-Urban Continuum Codes. USDA Economic Research Service U.S. Department of Agriculture. https://www.ers.usda.gov/data-products/rural-urban continuum-codes/. Published 2013. Updated December 2020. Accessed April 30, 2024.
Author Details
Keri Henderson, Vice President, Information Technology, PPD Clinical Research Business - Thermo Fisher Scientific
Publication Details
This article appeared in American Pharmaceutical Review: Vol. 27, No. 4May/June 2024Pages: 82-93
Subscribe to our e-newsletters
Stay up to date with the latest news, articles, and events. Plus, get special
offers from American Pharmaceutical Review delivered to your inbox!
Sign up now!