Subhash Dhawan- Senior FDA Research & Regulatory Scientist (Retired), Gaithersburg, MD.Email: [email protected]
Abstract: Translocation from cytoplasm to nucleus and integration of reverse-transcribed SARS-CoV-2 spike mRNA into the genomic DNA of COVID-19 mRNA-vaccinated individuals positive for HIV-1 or other retroviral infections raise the possibility of generation of a new type of retrovirus. Such a retrovirus expressing both HIV-1 receptor-binding domain (gp120) and SARS-CoV-2 receptor-binding domain (SARS-CoV-2-spike protein) could not only have the potential to bind and infect HIV-1 receptor CD4-positive cells but also to CD4-negative[1]SARS-CoV-2 receptor ACE2-positive cells that are widely distributed in the peripheral vascular and the central nervous system. This article details concerns arising from these realistic possibilities that need to be scientifically addressed and evaluated in COVID-19 mRNA vaccine recipients infected with retroviruses, including those who are at high risk to acquiring new retroviral infections.
Introduction
The highly contagious novel respiratory coronavirus, SARS-CoV-2, is readily transmissible to one another in proximity.1 An alarming number of COVID-19 cases continue to threaten human health and has greatly impacted us socially and economically. According to the November 2, 2022 WHO Coronavirus (COVID-19) Dashboard, 628 million COVID-19 global cases, including 6.6 million deaths, with 96 million COVID-19 cases and in excess of one million deaths in the United States are officially confirmed.2 According to a recently published report, the COVID-19 mRNA vaccination provides only moderate protection against symptomatic BA.1 and BA.2 Omicron infections and protection also wanes rapidly to negligible levels, starting four months after the second dose.3 Despite only moderate and rapidly waning protection against symptomatic infection, the mRNA vaccination reduces the severity of the COVID-19 disease, hospitalizations, and deaths.3 Nonetheless, constantly emerging SARS-CoV-2 mutants and variant strains continue to pose difficult challenges for the development of effective vaccines in real-time.
The mRNA vaccines are thought as a game-changer against SARS-CoV-2 infection, the virus that causes COVID-19. Billions of COVID-19 mRNA vaccine doses have been administered worldwide. This cutting-edge technology no doubt presents a novel approach for the development of COVID-19 vaccines; however, it is not free from certain valid scientific concerns. For example, in the individuals positive for HIV or other retroviral infections, SARS-CoV-2-spike mRNA delivered to the cytoplasm of retrovirus-infected cells via mRNA-containing lipid vesicles (i.e., by COVID-19 mRNA vaccination) may be vulnerable to reverse transcription by retrovirus-associated reverse transcriptase and integration into the genomic DNA by retrovirus-associated integrase. A new type of retroviral strain thus produced expressing both HIV receptor-binding domain (HIV-gp120) and SARS-CoV-2 receptor-binding domain (SARS-CoV-2-spike RBD) can bind to both HIV receptor (CD4) expressed on cells of the immune system (e.g., T-cells, macrophages) and certain neuronal cells as well as to SARS-CoV-2 receptor, ACE2, expressed on a variety of non-immune cells and can infect them regardless of the immune status of the infected individuals. This realistic possibility posing more medical challenges and likely much worse health consequences needs immediate attention.
In this article, I have tried to bring up the aforementioned concerns in an easy-to-understand format based on the wealth of knowledge we have gained on retrovirology in more than four decades. I strongly believe that a sound and careful evaluation of the role of SARS-CoV-2-spike mRNA in retroviral infections and pathogenesis is extremely important. These studies would provide valuable insights into possible secondary consequences of the COVID-19 mRNA vaccine administration in the individuals who are infected with retroviruses, latently or active, and also those who are at high risk to acquiring retroviral infections. The issues raised in this article necessitate strong consideration for a thorough scientific investigation to cautiously yet urgently prepare ourselves against the possibility of unforeseen future disastrous public health crises.
Biosynthesis of Proteins and Assembly in Normal Cells
Figure 1 shows basic steps in protein biosynthesis in normal cells. It involves transcription of DNA to mRNA inside the nucleus. This is the first step in protein biosynthesis. During protein biosynthesis, amino acids bind to specific molecules of transfer RNA and assemble by ribosomes into a sequence specified for messenger RNA (not shown in the diagram), which in turn transcribes from the genomic DNA. The transcribed mRNA translocated to the cytoplasm is translated into a polypeptide corresponding to the genetic codes of the codons in the mRNA. The coding sequence assemble nucleotide bases into codons, which are three specific nucleotides corresponding to a particular amino acid defined by the genetic code. Initiation of the translation process involves consecutive recruitment of the small and large subunits of ribosomes to specific mRNAs with the formation of an active ribosome at the translation initiation site the efficiency of which is determined by the factors that influence the translation initiation. Once the polypeptide chain is completed, the subsequent folding, post-translational modifications and protein packaging control functional properties of the protein using the primary sequence of amino acids.

Systemic Host Metabolic Dysfunctions in SARS-CoV-2 Infection
While the differential regulation of gene expression primarily occurs at the level of transcription, regulation of gene expression can also take place at the post-transcriptional level.

Cells within the tissues of the human body have variable phenotypic expression involved in crucial tissue organization and function in spite of being identical genomes due to the differential expression of genes. Any physiological variations, inflammatory conditions, oxidative states or metabolic changes (e.g., in SARS-CoV-2 infection as shown in Figure 2) could affect cellular functions, such as the uncoating of lipid vesicles, alteration of mRNA synthesis, endoplasmic reticulum (ER)/ ribosomal function, incomplete or defective translation, and, more importantly, incorrect protein folding. Post-translational modifications and subsequent transport could also alter the function of the synthesized protein. These possibilities cannot be ruled out, unless proved otherwise, in COVID-19 mRNA vaccinated individuals.
Biosynthesis of Proteins and Assembly in HIV-1-infected Cells
While in normal cells, transcription of DNA to mRNA is a unidirectional process which takes place in the nucleus (as shown in Figure 1); however, in HIV and other retrovirus-infected cells, mRNA in the cytoplasm is reverse transcribed to DNA and translocated to the cell nucleus (Figure 3).
The main early event in the life cycle of HIV-1 is the reverse transcription of viral RNA to DNA by virion-associated reverse transcriptase which is translocated to the nucleus as shown in Figure 3. In the nucleus, the viral integrase catalyzes a series of reactions whereby the intact viral RNA is inserted into the cellular chromosomal DNA forming provirus followed by translation of genomic and viral mRNA to respective proteins.
Viral integration and consequences on host gene expression has long been known.4 Moreover, recently published preclinical studies by Alden et al. of COVID-19 mRNA vaccine BNT162b2 (developed by Pfizer and BioNTech) showed reversible hepatic effects in animals that received the BNT162b2 injection.5 Although the experimental data reported by Alden et al. appear reasonable; however, this study was questioned by Merchant.6 In addition, another study published by Zhang et al. showed that SARS-CoV-2 RNA, at least in part, can be reverse-transcribed and integrated into the genome of human cells.7
Viral integration into the genomic DNA was extensively debated and recently reported in MedPage Today by Hackethal.8 Prominent scientists believed in the findings reported by Zhang et al. (see reference 8). Obviously, this is a highly concerning issue because of the issues related to possible modifications of the genomic DNA either by natural SARS-CoV-2 infection or by the administration of COVID-19 mRNA vaccine. This is particularly important in case of SARS-CoV-2- spike mRNA delivered by COVID-19 mRNA vaccines to the cytoplasm of cells in individuals infected with HIV or other retroviruses, a critical step that cannot be unequivocally proved in every single recipient of the vaccine.
Biosynthesis of SARS-CoV-2-spike Receptor-Binding Domain
Figure 4 illustrates basic steps in protein biosynthesis using modified N1-methylpseudouridine (m1Ψ) incorporated into a synthetic mRNA template (ACS Cent. Sci. 2021, 7, 748−756) to produce mRNA vaccines.9 Notably, the natural messenger RNAs, but not the N1-methylpseudouridine (m1Ψ) modified mRNA, are present in every cell of our body. The synthetic mRNA template used in the COVID-19 mRNA vaccine consists of SARS-CoV-2 spike receptor-binding domain (RBD) that the virus uses for entry into the cell. The synthetic SARS-CoV-2 mRNA encapsulated in a lipid vesicle is administered for immunization.
As shown in Figure 4, mRNA-containing lipid vesicle invaginates into the plasma membrane of the cells, randomly taken up by cells in the vaccinated area by non-receptor-mediated endocytosis, and the synthetic mRNA is released into the cytoplasm. This synthetic mRNA binds to ER/ribosomes to initiate the protein biosynthesis.
The nascent spike SARS-CoV-2 RBD (or polypeptide) after folding to proper conformation and post-translation modifications is transported to the cellular membrane or cytosol, depending upon the hydrophobicity or hydrophilicity of the amino acid residues in the synthesized protein, for eliciting the immune response specifically to SARS-CoV-2-spike RBD. Evidently, this complicated vaccination strategy is based on the assumption of efficiently producing SARS-CoV-2-spike RBD from the corresponding mRNA template injected intramuscularly in the vaccine recipients, and relies solely on cells in tissues performing normal physiological functions.

Importantly, on the other hand, in retroviral infections, for example HIV as depicted in Figure 5, however, the SARS-CoV-2-RBD mRNA delivered to the cytoplasm can be reverse-transcribed and subsequently integrated into the genomic DNA producing a new replicating HIV virion expressing both HIV and SARS-CoV-2-spike proteins rendering a new type of HIV that could target both immune cells as well as non-immune cells. Figure 5 also depicts how SARS-CoV-2-spike mRNA may be introduced into the cell cytoplasm by COVID-19 mRNA vaccination that can be reverse transcribed to DNA and incorporated into the chromosomal DNA along with HIV DNA for producing HIV virion expressing both HIV and SARS-CoV-2-spike proteins rendering a new type of HIV. Such type of produced HIV could target both immune cells as well as non-immune cells.
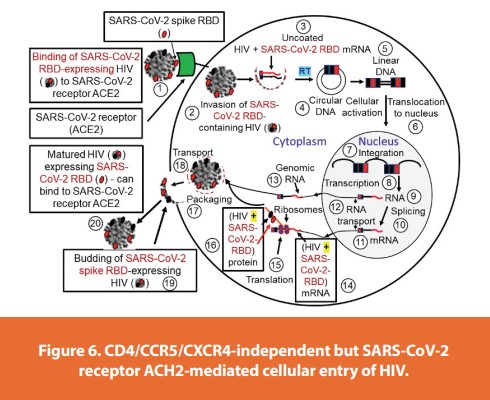
This is a highly concerning matter because the newly generated retrovirus expressing both HIV-RBD as well as SARS-CoV-2-spike RBD could not only bind, invade and replicate in cells with CD4/ CCR5/CXCR4-positive surface phenotypes but also CD4/CCR5/CXCR4-negative cells via SARS-CoV-2 receptor ACE2 (Figure 6). Host transcription factors then enable the HIV provirus to use the cellular transcription machinery to multiple repeats and then transported to cell membrane where a matured virus is released. This realistic possibility is again highly concerning as the cells of non-immune systems could also become viable target for HIV infection. Figure 7 illustrates a model diagram depicting this possibility.
Adding to these unanswered questions is controversy around the efficacy of COVID-19 mRNA vaccine. This may, however, be possible due to different opinions of scientists or inconsistent interpretation of experimental or clinical data. For example, in a recently published article,10 Plummer and Pavia’s description of COVID-19 vaccines in HIV infected patients seems to be unclear. On one hand, these authors have stated “Limited clinical trials have also shown that the currently available COVID-19 vaccines have gone through rigorous safety tests and have met both safe and effective in affording protection to HIV/ AIDS patients”, and “COVID-19 vaccines have gone through rigorous safety tests and have met or even exceeded similar standards.” On the other hand, however, in the same article, they state that people with HIV have been included in clinical trials though there is “limited safety and efficacy data available as they pertain specifically to this group.” They further state, “The majority of the published literature has not supported a significantly higher risk for severe disease among HIV/AIDS patients in the United States and Europe, although a large population-based study in South Africa reported a higher rate of death due to COVID-19 (Viruses 2021, 13, 1890, page 13)”. Nonetheless, the authors recognize that “higher rates of comorbidities associated with COVID-19 disease severity among HIV/AIDS patients is an area that still needs to be monitored closely”.

With frequent mutations in SARS-CoV-2 spike protein, variability in different codons rendering the translated protein with altered amino acid residues may not only cause misfolding, but also form insoluble aggregate clusters inside the cell. Misfolding of even normal proteins is known to cause diseases (such as Alzheimer’s, Prion (PrPsc) disease, etc.). Therefore, a clear scientific understanding of any of these intracellular events is required to prevent undesired secondary consequences in the COVIC-19 mRNA-vaccinated individuals.
Conclusion and Perspective
The COVID-19 vaccines are widely used to prevent severe illnesses, hospitalizations, and deaths in the general population and those who are at high risk to acquiring SARS-CoV-2 (the virus that causes COVID-19) infections. The basic principle of COVID-19 mRNA vaccine is primarily to generate SARS-CoV-2-receptor binding domain (RBD) by intracellular machinery in the tissues to subsequently elicit specific immune response against the SARS-CoV-2-RBD. Because the hydroxyl groups make RNA less stable as it is more prone to hydrolysis and, therefore, is highly unstable. Instead N1-methylpseudouridine (m1Ψ) modified base is used to chemically synthesize the RNA template which is encapsulated in lipid vesicles to generate COVID-19 vaccine. The vaccine is injected intramuscularly for immunization. While this cutting-edge technology presents a novel approach for the development of a vaccine, it has certain limitations or drawbacks, as may be expected with any vaccine. This brief article, brings up a few realistic possibilities in a positive manner where COVID-19 mRNA vaccines need a careful scientific evaluation; particularly, in metabolic disorders, retrovirus infections, and other medical conditions in which cells within the tissues may not perform efficient normal physiological functions thus potentially hamper any number of steps during the natural protein biosynthesis.
Reverse-transcribed SARS-CoV-2-spike mRNA in COVID-19 mRNA-vaccinated individuals with retroviral infections is vulnerable to generating new types of retroviruses with novel tropism. The new retroviral variant(s) could bind and infect both CD4-positive cells (target for HIV) as well as CD4-negative but ACE2-expressing cells (target for SARS-CoV-2). As of August 2022, an estimated 38 million people are living with HIV11 and, as of March 2021, an estimated 5-10 million people globally were reported to be infected with human T-cell leukemia virus type-1 or T lymphotropic virus type-1, (HTLV-1),12 the first human retrovirus reported to infect T-cells,13 and is present in diverse regions of the world. Therefore, a thorough scientific study on COVID-19-spike RBD synthetic mRNA in retroviral infections and also in COVID-19 mRNA-vaccinated individuals living with HIV, HTLV-1 and other retroviruses, including those who are at high risk to acquiring retroviral infections, would allow a better understanding of potentially risky, perhaps more deadly, public health consequences and to prepare ourselves ahead of time to face such challenges.
References
- Davies NG, Abbott S, Barnard RC., et al. Estimated transmissibility and impact of SARS[1]CoV-2 lineage B.1.1.7 in England. Science. 2021,372(6538):eabg3055.
- WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int/
- Chemaitelly H, Ayoub HH, AlMukdad S, et al. Duration of mRNA vaccine protection against SARS-CoV-2 Omicron BA.1 and BA.2 subvariants in Qatar. Nature Comm. (2022) 13:3083, 3082 | https://doi.org/10.1038/s41467-022-30895-3
- Desfarges S, Ciuffi A. Viral integration and consequences on host gene expression. Viruses: Essential Agents of Life. 2012 Sep 25:147–175. doi: 10.1007/978-94-007-4899-6_7
- Aldén M, Olofsson Falla F, Yang D, et al. Intracellular reverse transcription of Pfizer BioNTech COVID-19 mRNA vaccine BNT162b2 in vitro in human liver cell line. Curr. Issues Mol. Biol. 2022. 44(3),1115-1126. https://doi.org/10.3390/cimb44030073
- Merchant HA. Comment on Alden et al. Intracellular reverse transcription of Pfizer BioNTech COVID-19 mRNA vaccine BNT162b2 in vitro in human liver cell line. Curr Issues Mol Biol 2022. 2022. 44(4),1661–1663. doi: 10.3390/cimb44040113
- Zhang L, Richards A, Barrasa MI; et al. Reverse-transcribed SARS-CoV-2 RNA can integrate into the genome of cultured human cells and can be expressed in patient-derived tissues. Proc Natl Acad Sci USA. 2021,118,e2105968118, https://doi.org/10.1073/pnas.210596811
- Hackethal V. Can COVID-19 Genes Integrate Into Human DNA? — Debate rages over whether SARS-CoV-2 can insert bits of its RNA into the human genome. MedPage Today, May 17, 2021; https://www.medpagetoday.com/special-reports/exclusives/92632
- Nance KD, Meier JL. Modifications in an Emergency: The role of N1-methylpseudouridine in COVID-19 vaccines. ACS Cent. Sci. 2021,7,748–756, https://doi.org/10.1021/ acscentsci.1c00197
- Plummer MM, Pavia CS. COVID-19 Vaccines for HIV-Infected Patients. Viruses 2021, 13,1890; https://doi.org/10.3390/v13101890
- The global HIV/AIDS epidemic. 2022. Global statistics/HIV.gov
- New WHO report on human T-lymphotropic virus type-1 highlights strategies for its prevention and control. 2021. https://www.who.int
- Gallo RC, Sarin PS, Gelman EP, et al. Isolation of human T-cell leukemia virus in acquired immune deficiency syndrome (AIDS). Science 1983;220(4599),865-867. https://doi. org/10.1126/science.6601823
Acknowledgments: This article is dedicated to loving memory of my Guruma Mrs. Savita Gupta.
Funding: This work received no external funding.
Conflicts of Interest: The author declares no conflict of interest.
Author Biography
Dr. Subhash Dhawan is a viral immunologist. He retired after serving for nearly 25 years as Chief of Viral Immunology Section in the Laboratory of Molecular Virology, Division of Emerging and Transfusion Transmitted Diseases, Center for Biologics Evaluation and Research, U.S. Food and Drug Administration. Dr. Dhawan is now an independent writer and provides guidance on research and regulatory projects related to in vitro diagnostics, vaccines, and therapeutics.
Subscribe to our e-Newsletters
Stay up to date with the latest news, articles, and events. Plus, get special
offers from American Pharmaceutical Review delivered to your inbox!
Sign up now!