Abstract
Since the first monoclonal antibody (mAb) drug was approved in 1986, more than 100 different mAbs have been approved by the U.S. FDA (Food and Drug Administration) and EMA (European Medicines Agency). During this period, manufacturing scaled up from an almost lab-like process to pharma-grade manufacturing with greater standardization and quality, to address the increasing demands for the treatment of more patients in a variety of therapeutic areas. In 2013, EMA approved the first biosimilar version of the monoclonal antibody infliximab, opening a new market for biosimilars.
After mAbs, cell and gene therapy represents the next frontier of personalized medicine, and the recent success of Chimeric Antigen Receptor T-cell (CAR-T) therapies in certain types of blood tumors is fostering higher demand for patient treatment, and expansion of their development in other therapeutic areas, such as neuroscience and immunology, or solid tumors. In this article, we evaluate the probability of a future market for biosimilar versions of CAR-T therapies or “CAR-T-similars,” assessing the factors that would support or preclude its birth and expansion.
Introduction
The use of monoclonal antibodies (mAbs) has been leading a therapeutic revolution towards more personalized medicine, and their success is underpinned by biotechnology products representing more than 60% of the top-selling products in 2023 versus conventional therapy.1
The first licensed monoclonal antibody was Orthoclone OKT3 (muromonab-CD3), approved in 1986 for use in preventing kidney transplant rejection.2 However, its use was limited due to reported side effects. Now, there are more than 100 approved mAb-based drugs,3 with an estimated market value of $208.32B in 2022, growing at a 12% compound annual growth rate (CAGR) through 2032. Many of the first mAbs licensed to the market (such as Rituximab, Infliximab, or Adalimumab) quickly achieved blockbuster sales volume.
Many factors in mAbs development converged to create a compelling business case for investors to think about biosimilars as a new cost-effective, differentiated therapy for patients. First and most important was the massive, growing market of biological medications with a higher cost per dose versus conventional therapy, as well as approaching patent expirations of the originator drugs. Then there were manufacturing process improvements with increased efficiency and reduced cost of production that favored more competitive price offerings compared to the originator drug(s).
For example, the number of biosimilar versions (or “competitors”) of the originator drug is a key aspect. The erosion of the originator’s price reached a 25% average at the entry of the first biosimilar and could fall below 50% with the third version, or even 70% when the number of competitors achieves or exceeds five.6
Today, the biosimilar global market is projected to reach $66.9B by 2028 with a CAGR of 17.8%.5
The Cell and Gene Therapy Revolution and the Promise of CAR-T Therapy
The progress towards personalized medicine recently received a boost with the success of the first licensed cell and gene therapy (CGT) products. Thanks to the advancements in our understanding of cell biology, we are becoming increasingly precise in designing and implementing genetic modifications to treat diseases that were previously considered untreatable or characterized by a very high mortality rate.
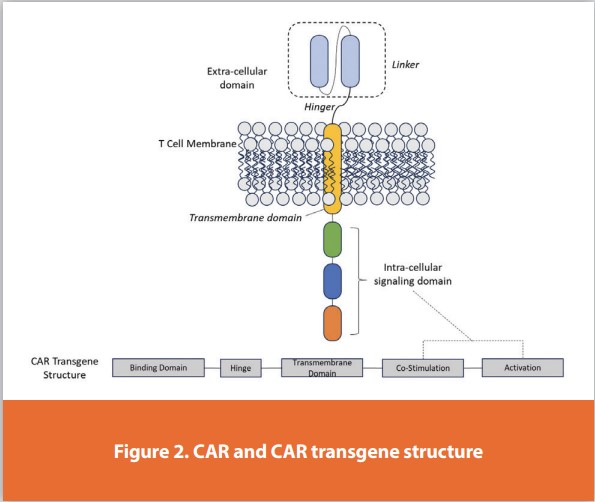
Among emerging CGTs, Chimeric Antigen Receptor T-cell therapy (CAR-T) is gaining special attention for its potential implications in a wide array of diseases. CAR-T therapy is a type of treatment in which a patient’s T cells (a type of immune system cell) are modified to attack cancer cells.8 T cells are taken from a patient’s blood, and then the gene (Figure 2) for a special receptor that binds to certain proteins on the patient’s cancer cells is added to the T cells in the laboratory.
The first FDA-approved CAR-T therapy was Kimryah (tisagenlecleucel) in 2017, for the treatment of Acute Lymphoblastic Leukemia, Diffuse Large B-cell lymphoma, and Follicular Lymphoma. Since then, another five CAR-T therapies have been approved for the treatment of hematological malignancies.9
Because CAR-T therapies are directed against antigens normally expressed on B cells, and B cell dysregulation is also involved in autoimmune conditions, clinical trials are rapidly expanding into other indications, such as Systemic Lupus Erythematosus (where successful results are already published), Lupus Nephritis and Multiple Sclerosis. The interest of the scientific community in CAR-T therapy is confirmed by the number of ongoing clinical trials: 716 active recruiting studies.10
However, despite the remarkable outcomes in clinical trials and the excitement around benefits for patients, CAR-T therapies come with a cost, estimated between $373,000 and $475,000 per infusion, excluding extra procedures and facility costs.11 In fact, such therapy is usually performed in an inpatient environment, since it requires the infusion of modified T cells and consequent monitoring of the disease status, costing an additional $79,466 to $85,267.12
A Business Case for CAR-T-Similars – Promoting and Limiting Factors
In a 2019 statement, former FDA commissioner Scott Gottlieb declared that the FDA was witnessing a surge of cell and gene therapy products entering early development. By 2025, he predicted that the FDA will be approving 10 to 20 CGT products a year, based on an assessment of the current pipeline and the clinical success rates.13
The Alliance for Regenerative Medicine reported in its January 2024 meeting that up to 17 regulatory CGT approvals in the U.S. and Europe are anticipated by the end of 2024, compared to eight approvals in 2023.10 Therefore, the forecasted surge of cell and gene therapy products development is occurring at a fast pace.
Accordingly, two contributing factors for the “business” case of biosimilar development are already present: 1) the higher cost of therapies compared to conventional therapy products, and 2) the growing market of CGT products, with CAR-T therapy market size valued at $1.75B in 2023 and expected to be worth $88.52B in 2032 growing at a CAGR of 29.8%.14
The manufacturing and administration of CAR-T therapies represent one component of their high prices because it is a multi-step process including leukapheresis (a procedure needed to remove white cells from the blood), genetic engineering of T cells using viral vectors, and expansion of modified T cells in a controlled environment. The patient-tailored nature of autologous CAR T-cell therapy further raises the cost of production. Patient-specific features also impose additional logistical expenses relating to the apheresis process, cryopreservation, transportation of patient-derived cells to specialized manufacturing facilities, and the subsequent shipment of the final therapeutic product back to the clinical site.15
The broad clinical trials pipeline of CAR-T and the promise of more approvals coming soon are creating the need for more scalable, robust,t and cost-effective manufacturing. Ayala Ceja et al. summarized next-generation strategies for CAR-T cell manufacturing16 to overcome the current low-throughput, resource-intensive limitations of the conventional cell manufacturing process:
- Accelerated cell manufacturing – next-generation manufacturing processes arriving at the final product formulation within 24 hours. The bulk of the time savings result from a significant shortening of the ex vivo expansion period.
- Process automation – this has the potential to reduce production costs, the probability of manufacturing failures attributed to human error, and contamination via touchpoints. Automation could also significantly reduce the numbers and experience levels required of the manufacturing staff.
- In vivo cell manufacturing – the next-generation manufacturing process could eliminate ex vivo cell manipulation and expansion, leveraging the ability to transduce T cells in vivo, using alternative types of carriers that have been shown to deliver nucleic-acid payloads to T cells in vivo.
The convergence of the high costs of CAR-T therapies, the estimated growth of the market, and improved efficiency in manufacturing can promote the development of a CAR-T-similars market as the first CAR-T therapies would approach patent expiration. However, other factors will be limitations on the “business case” for CAR-T-similars:
- The specific manufacturing process could preclude achieving enough efficiency to generate needed profit margins while ensuring a competitive cost reduction of the final drug products.
- The accelerated manufacturing process could potentially produce “over-active” T cells leading to increased toxicities, and process automation could reduce the ability to respond to patient-specific cell behavior. This could potentially be avoided by the allogeneic approach versus autologous, but it entails additional considerations and hurdles, such as graft-versus-host disease.
The fast-paced progress versus alternative manufacturing or in vivo, transduction techniques could potentially make CAR-T-similars obsolete in a few years. Beyond manufacturing, another critical aspect would be the applicable regulatory frames and rules to demonstrate the “similarity” of CAR-T-similars versus their originator products.
Conclusion
Ten years after EMA approved the first biosimilar version of a mAb, CGT products are starting a second revolution, with CAR-T therapies claiming a major stake. The benefits and wider applications of CAR-T therapies are supported by very promising outcomes of clinical trials and will provide more effective treatment options to patients suffering from oncological and autoimmune diseases.
There are several common features that can recreate for CAR-T-similars the same conditions that favored the boom of the biosimilar market. Transgene engineering, automated closed system manufacturing, and transduction techniques are rapidly scaling up from lab-based processes to pharma-grade manufacturing with increased yields, standardization, quality, and purity.
While the experience with biosimilars to date provides an example of a successful business case, there are uncertainties linked to the manufacturing complexities and limitations of CAR-T therapy, and an as-yet nonexistent regulatory frame, which could make CAR-T-similars an interesting but premature thought. In the short term, the industry focus will be on the expansion of CAR-T applications and the optimization of the manufacturing process. It may be years before we see the first CAR-T-similar licensed for the market. In the meantime, regulatory guidance would be needed about how “comparability” should be proved.
References
- Evaluate – World Preview 2023.
- Justin K.H. Liu, The history of monoclonal antibody development – Progress, remaining challenges and future innovations, Ann Med Surg (Lond). 2014 Dec; 3(4): 113–116.
- The Antibody Society. Therapeutic monoclonal antibodies approved or in review in the EU or US. (May 2024); www.antibodysociety.org/resources/approved-antibodies.
- https://www.fda.gov/drugs/biosimilars/biosimilar-product-information.
- https://www.marketsandmarkets.com/Market-Reports/biosimilars-40.html.
- Jose Ignacio Diaz, The Second Waves of Biosimilars: New Scenarios, New Rules, Biosimilar Development, Guest Column | December 15, 2020.
- https://www.cancer.gov/about-cancer/treatment/research/car-t-cells.
- Yi-Ju Chen, Bams Abila, and Yasser Mostafa Kamel*, CAR-T: What Is Next, Cancers (Basel). 2023 Feb; 15(3): 663.
- Davide Garrisi, Kim Watanabe, From Hematologic to Autoimmune Disease – The CAR-T Therapy Second Revolution, Biospectrum Asia, 01 May 2024 | Opinion, https://www. biospectrumasia.com/opinion/26/24159/from-hematologic-to-autoimmune-disease[1]the-car-t-therapy-second-revolution-.html.
- Clinicaltrials.gov search for active and recruiting CAR-T clinical trials, May 2024.
- Fiorenza S., Ritchie D.S., Ramsey S.D., Turtle C.J., Roth J.A. Value and affordability of CAR T-cell therapy in the United States. Bone Marrow Transpl. 2020;55:1706–1715. Doi: 10.1038/s41409-020-0956-8.
- Lyman G.H., Nguyen A., Snyder S., Gitlin M., Chung K.C. Economic Evaluation of Chimeric Antigen Receptor T-Cell Therapy by Site of Care Among Patients With Relapsed or Refractory Large B-Cell Lymphoma. JAMA Netw. Open. 2020;3:e202072. Doi: 10.1001/ jamanetworkopen.2020.2072.
- https://www.fda.gov/news-events/press-announcements/statement-fda-commissioner-scott-gottlieb-md-and-peter-marks-md-phd-director-center-biologics#:~:text=Taken%20together%2C%20these%20guidance%20documents,of%20the%20most%20intractable%20diseases.
- https://www.biospace.com/article/car-t-cell-therapy-market-is-rising-rapidly-at-cagr-29-8-percent-by-2032/#:~:text=The%20global%20CAR%20T%2Dcell,USD%201.75%20 billion%20in%202023.
- Cliff et alt, High Cost of Chimeric Antigen Receptor T-Cells: Challenges and Solutions, 2023 ASCO EDUCATIONAL BOOK, DOI https://doi.org/10.1200/EDBK_397912.
- Ayala Ceja et al., CAR-T cell manufacturing: Major process parameters and next-generation strategies, Journal of Experimental Medicine, https://doi.org/10.1084/jem.20230903
Author Details
Rosa Rodriguez, Vice President, Biosimilar Intelligence Group, PPD clinical research business- Thermo Fisher Scientific; Davide Garrisi, Vice President, Cell and Gene Therapy Institute, PPD clinical research business- Thermo Fisher Scientific
Publication Details
This article appeared in American Pharmaceutical Review: Vol. 27, No. 6Sept/Oct 2024Pages: 31-33
Subscribe to our e-newsletters
Stay up to date with the latest news, articles, and events. Plus, get special
offers from American Pharmaceutical Review delivered to your inbox!
Sign up now!