Introduction
Today, more than 2500 medical entities are approved in the United States alone and more than 4000 on a global scale1. Still, there exists notable unmet medical need, which is being addressed by significant investments into the development of various kinds of innovative medicines. This has led – among other things – to the approval of 41 new medical entities by the FDA in 20142. In addition, dozens of mature drug delivery technologies are available today, and a substantial number of novel ones is under current development. Looking at the large group of approved medical entities as well as all available and emerging drug delivery technologies together, it becomes obvious that there is a huge opportunity space for innovation. Hence, it may be tempting for many drug delivery scientists and drug developers to start the development of new medicines with a strong focus on technology. However, innovation in this domain should not be created via a pure technology push. In order to effectively address unmet medical need and ultimately provide improved patient outcomes, the innovation process should be carried out in a technology-agnostic way in the beginning and start with a focused patient pull.
Past Drug Delivery Innovation Provided Medicines that Benefit Patients Today
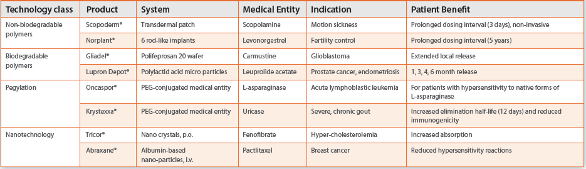
Looking at the history of drug delivery innovation, it becomes evident that the field has made many important medicines available to patients3. Several waves of innovation occurred over the past five decades and delivered medicines based on a variety of technology classes, including non-biodegradable and biodegradable polymers, pegylated macromolecules, and nanotechnology, among others (see Table 1)4.
Table 1. Examples of drug delivery enabled medicines providing specific patient benefits
While the mostly technology driven development of drug delivery systems in the period from the 1970s to 2000s has led to impactful innovations, more recently one of the most frequently asked questions in drug development as a whole is: “How to innovate in a way which reliably delivers improved patient outcomes?” This important question has led to a variety of initiatives and regulatory documents, which in aggregate shed some light on the tasks and opportunities at hand.
The Evolving Field of Patient-Centricity in Drug Development
In the recent past, regulatory guidance as well as various initiatives started to focus on meeting patient need and thus helped to frame the evolving field of patient-centricity. ICH Q8(R2) Pharmaceutical Development5 for example states that “In all cases, the product should be designed to meet patients’ needs and the intended product performance.” In the area of medical device design a draft guidance from 2011 discusses the need for applying human factors and usability engineering to optimize medical device design6. The Patient-Centered Outcomes Research Institute (PCORI) shared its National Priorities and Research Agenda in 2012 with “Accelerating patient-centered outcomes research and methodological research” being one of the priorities7. Recently, the FDA’s “Patient-focused drug development initiative” took shape, and a series of meetings in specific disease areas, including narcolepsy, lung cancer and fibromyalgia, started in 2013. Webcasts of past meetings are available online8. More recently, the AAPS Focus Group on Patient-Centric Drug Development, Product Design, and Manufacturing has been established9, aiming at the development of the science around patients, their needs, and their interface with drug products. Very recently, the Catalent Applied Drug Delivery Institute with the support of the Lung Cancer Alliance surveyed a group of lung cancer patients relative to unmet needs in therapeutic and supportive care which revealed that even patients with excellent therapeutic outcomes continued to have unmet needs in the areas of patient experience and quality of life10.
For many scientists and development teams working on future drug delivery enabled medicines, these are helpful documents and initiatives. Yet, several questions still remain to be answered, including: “How to best utilize the derived patient need insights?” and “How to design and run a coherent process for patient-centered drug delivery innovation?”
Patient Pull Versus Technology Push
 Figure 1. Technology push (in red) vs. patient pull (in blue)
Figure 1. Technology push (in red) vs. patient pull (in blue)Both the de novo creation of a patient-centered innovation process as well as the transformation of an existing innovation process to a patient-centered one starts at the conceptual level. Figure 1 compares the difference between the technology push and the patient pull principle in drug development.
The main distinction between both principles is the investment in an in-depth understanding of unmet patient need already at the outset of the concept phase of drug delivery system development. While it may seem intuitive and simple at the conceptual level to use the patient pull principle in the development of a new medicine, it may not be as intuitive how to implement it in a meaningful way. Drug delivery scientists often have primarily been trained in the domains of science and technology and frequently are keen on applying technology in the creation of a novel medicine. As Maslow succinctly stated in 1966 “I suppose it is tempting, if the only tool you have is a hammer, to treat everything as if it were a nail11.” However, at the outset of the development of a novel medicine, one must be careful not to blindly follow the law of the instrument. Rather than focusing on a certain technology or tool early on, the overall innovation process benefits from being executed in a technology-agnostic and even medical entity-agnostic way in the beginning. The focus of the development team needs to lie on developing a deep understanding of patient needs which then serves as a guidepost throughout the overall development process.
The Patient Pull Principle in More Detail
The ultimate goal of utilizing the patient pull principle is enabling innovation that is capable of providing improved patient outcomes. A process based on this principle starts with the gathering of information in five layers (see Figure 2).
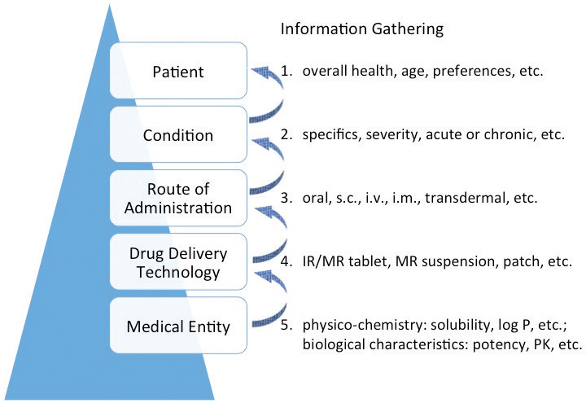 Figure 2. Applying the patient pull principle to drug delivery innovation
Figure 2. Applying the patient pull principle to drug delivery innovationThe top two layers of information gathering concern the understanding of patient needs, which may be determined by the patient’s overall health status, age and preferences as well as by the specifics of the condition – acute or chronic - to be treated. Only after these two information layers have been thoroughly investigated, the next three layers should be explored. This entails considerations with regard to the usefulness of particular routes of administration and consequently suitability of certain drug delivery technologies. Ultimately, the infor-mation gathering will lead to the question which medical entity could be utilized, and in how far its physicochemical and biological characteristics would be suitable for the development of the targeted new medicine. Drug delivery experts often are highly experienced and rely on multiple resources when it comes to addressing the questions from the layers three to five - route of administration/drug delivery technology/medical entity - in Figure 2. However, information gathering at the top two layers – patient/indication – has been less routinely done in the past. Therefore, ways to do that and resources available will be addressed in more detail below.
How to Learn About Patient Needs
The successful use of processes based on concepts like human centered design,12,13 and the lead user concept14 in the development of medical devices and surgical dressings has demonstrated that the sound understanding of human/customer needs can be paramount for successful product innovation in the life sciences space and beyond. The herein discussed patient pull principle follows a logic comparable to the ones of the aforementioned concepts by putting the patient and his or her needs at the center of the new medicine’s development. Drug development scientists and teams can obtain highly relevant information in a variety of ways, including by directly connecting with:
- Patients
and learning how they use their medicines, in their own environment, what they like, what they don’t like, what they want, etc. - Patient Advocacy Groups
like NORD (www.rarediseases.org), Geriatric Medicine Society (www.geriatric-medicine.org), Prostate Cancer Foundation (www.pcf.org), etc. - Caregivers
like caregivers for pediatric patients or geriatric patients, etc.
It is of utmost importance, that the team members working on the concept and realization of the novel medicine themselves are deeply involved in the information gathering, which must not be delegated outside the development team. This direct and personal immersion into patient needs is the basis for executing new medicine development in the desired patient-centered manner. It guarantees, that critical project decisions along the way will more often be grounded on what they might bear for the patient, rather than for the technology or the product itself.
Optimized Design and Use of Clinical Studies
Another significant source of information relative to patient needs and patient experiences are data from clinical trials conducted with the developmental drug delivery system. While this in itself is intuitive, it seems that there is room for improvement when it comes to the design and execution of clinical trials with an emphasis on patient needs and outcomes. Basch stated in 2013 “As an oncologist, when I sit with patients to discuss starting a new chemotherapy regimen, their first questions are often ‘How will it make me feel?’ and ‘How did patients like me feel with this treatment?’ Regrettably, this information is generally missing from U.S. drug labels and from published reports of clinical trials15 …”
 Figure 3. Patient-centered optimization of clinical studies
Figure 3. Patient-centered optimization of clinical studiesMain levers for the optimization of clinical trials include patient involvement in clinical study design, clinical study participation (study accessibility for the right patients), and recording of patient reported outcomes (PRO; see Figure 3).
Galsky16 advocates the use of patient insights for the design of clinical trials for example via the use of crowdsourcing across a large number of patients, but also including researchers and advocates.
He, furthermore, points out that some cancer trials are geographically inaccessible to certain patients and that clinical research centers do not always provide good accessibility for patients. Hence, he suggests the use of telemedicine and telemonitoring among other things as a means to reach patients that need those clinical trials17. A study published by BayBio emphasizes the need to ask the right questions during the execution of cancer clinical studies with an emphasis on patient reported outcomes in addition to efficacy and safety data18. This assessment is based on an evaluation of 300 cancer trials of which 126 had been conducted without the documentation of PRO.
While the involvement of patients during the design of clinical studies, providing study accessibility to the right patients and recording patient reported outcomes will be beneficial in the optimization of almost any developmental medicine, these levers are particularly powerful when it comes to the development of new drug delivery systems. Examining patient experiences like ease-of-use and reliability in cases of complex systems, wear properties like skin tolerability and adhesion in cases of transdermal patches, swallowability and taste in cases of pediatric oral dose forms are just a few examples from the drug delivery domain to be named here. As a result, valuable feedback directly from the patient can be utilized to design and develop medicines which will provide better outcomes.
Important Building Blocks of the Patient-Centered Drug Delivery Innovation Process
The building blocks supporting the creation of patient-centered drug delivery innovation are depicted in Figure 4.
 Figure 4. Building blocks of the patient-centered drug delivery innovation process
Figure 4. Building blocks of the patient-centered drug delivery innovation processThe development of a new medicine typically follows a stage gate process – comprising at the highest level of granularity a concept phase, pre-clinical and clinical phases as well as market introduction. It is depicted in blue in Figure 4. Many aspects of this process are defined by both international regulatory guidance and proven concepts of new drug development. In order to run a truly patientcentered innovation process under the umbrella of such a stage gate process, it is important to apply the patient pull principle from the outset, whereas the clinical phases and studies benefit from the use of patient design input, participation, and PRO with the ultimate goal to enable improved patient outcomes. Patient-centered drug delivery innovation should be performed in a technology-agnostic and medical entity-agnostic way in the early phases. Only later on, the selection of a suitable drug delivery technology and medical entity should be carried out by applying of comprehensive technology know-how. Insights from patients, advocacy groups and caregivers as well as relevant regulatory guidance should be utilized throughout.
Summary
The availability of more than 4000 medical entities together with today’s access to dozens of established and evolving drug delivery technologies creates a significant opportunity space for the development of innovative drug delivery systems. The generation of valuable medicines in this domain will benefit from an in-depth understanding of unmet patient needs by every member of the development team and the use of the patient pull principle early on. A patient-centered innovation process should be applied throughout the development of the new medicine, thus enhancing its ability to ultimately provide improved patient outcomes.
References
- Huang R, Southall N, Wang Y, et al. The NCGC Pharmaceutical Collection: A comprehensive resource of clinically approved drugs enabling repurposing and chemical genomics. Sci Transl Med. 2011;3(80):16.
- http://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/DrugInnovation/UCM430299.pdf. Accessed July 23, 2015.
- Hoffman AS, The origins and evolution of “controlled” drug delivery systems. J. Control Release. 2008;132, 153-163.
- Lipp R, The evolution of controlled release and patient-centered drug delivery. BioPharma Asia. 2014;3, 42-47.
- Guidance for Industry, Q8(R2) Pharmaceutical Development, ICH, November 2009.
- Draft Guidance for Industry and Food and Drug Administration Staff, Applying human factors and usability engineering to optimize medical device design, June 23, 2011. http://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/UCM259760.pdf. Accessed July 23, 2015
- http://www.pcori.org/research-results/research-we-support/national-priorities-andresearch-agenda. Accessed July 23, 2015
- http://www.fda.gov/ForIndustry/UserFees/PrescriptionDrugUserFee/ucm347317.htm. Accessed July 23, 2015.
- http://www.aaps.org/Patient-Centric/. Accessed July 23, 2015.
- Savla R, Cornell S, Therapeutic and supportive care unmet needs in lung cancer patients, Thorac Oncol 2015;10 (9) suppl 2:S517.
- Maslow AH, The psychology of science, New York, NY, USA: Harper and Row, 1966: 16.
- Kelley T, Littman J, The art of innovation, Doubleday, New York, NY USA: Random House, 2001.
- http://www.ideo.com/about/. Accessed July 23, 2015.
- von Hippel E, Thomke S, Sonnack M, Creating breakthroughs at 3M, Harvard Business Review, 1999 Sept. –Oct., p. 3-9, Reprint 99510.
- Basch E, Toward patient-centered drug development in oncology, N Engl J Med 2013; 369:397-400, 2013.
- http://www.pcf.org/site/c.leJRIROrEpH/b.8964757/k.188D/PatientCentered_Drug_Development_video.htm. Video 1, accessed July 23, 2015.
- http://www.pcf.org/site/c.leJRIROrEpH/b.8964757/k.188D/PatientCentered_Drug_Development_video.htm. Video 2, accessed July 23, 2015.
- http://baybio.org/patient-centered-outcomes-in-phase-iiiii-and-phase-iii-oncologyindications-are-manufacturers-focusing-on-the-patient/. Accessed July 23, 2015.
Author Biography
Ralph Lipp, PhD, President and CEO of Lipp Life Sciences LLC, advises clients on various aspects of innovation-based value creation and generates new product opportunities by addressing unmet medical need with patient-centered innovation. He also serves as the founding Advisory Board Member of the Catalent Applied Drug Delivery Institute. Before founding Lipp Life Sciences LLC, Ralph served as Vice President Pharmaceutical Sciences R&D at Eli Lilly and Company and Head of Pharmaceutical Development at Schering AG. Ralph holds a degree in Pharmacy from Johannes Gutenberg University in Mainz, Germany and obtained a Ph.D. in Medicinal Chemistry as well as a Habilitation for Pharmaceutical Technology from Freie Universität Berlin, Germany. His scientific contributions comprise over 130 publications, including more than 20 patents, covering 5 marketed medicines.