Abstract
A multiparticulate formulation technology can be beneficial in designing a patient-centric dosage form. One such dosage form is minitablets, which are compressed tablets with typical diameters of one to four millimeters. Minitablets can offer versatile applications, including as a pediatric dosage form, for patients with dysphagia, and uses where rapid or flexible dose adjustments are needed. Variations of the tablet formulation and coating systems can achieve specific functionalities such as orally disintegrating tablets (ODTs), extended release formulations, or gastrointestinal-targeted delivery. Many of the manufacturing unit operations used to produce minitablet-based dosage forms are the same as those employed in manufacturing of larger tablet images. However, due their unique size, some adjustments to the manufacturing processes and testing approaches may be required. These considerations are discussed in this paper, along with perspectives of the challenges and opportunities of designing a minitablet-based dosage forms.
Background and Potential Applications of Minitablets
The term “minitablets” commonly refers to compressed tablets with size smaller than typical tablets. Although there are currently no regulatory guidelines that define minitablets (sometimes referred to as microtablets),1 the term has been used to describe tablets with diameters between one to four millimeters (mm). Since oral dosage forms smaller than 2.5 mm can be considered as oral granules,2 many minitablet products are focused at this size range, to take advantage of the potential flexibility in dosage form administration (e.g. mixed with soft foods).
 Figure 1. Minitablets with (from top to bottom) four, three, and two millimeter diameters, pictured with a U.S. penny to illustrate their sizes.
Figure 1. Minitablets with (from top to bottom) four, three, and two millimeter diameters, pictured with a U.S. penny to illustrate their sizes.From a product design perspective, minitablets have many potential advantages.3 First, minitablets enjoy the benefits of larger size oral tablets, such as being convenient to administer, cost effective to ship, and can be afforded protection against moisture or light. Minitablets also allow the opportunity to present a multiparticulate dosage form manufactured via compression, which is more efficient than extrusion-spheronization, allows a larger active pharmaceutical ingredient (API) weight than coating layers, and may avoid the use of aqueous or organic solvents. By utilizing a minitablet multiparticulate system, modified release profiles have been demonstrated, including extended or sustained release,4-8 chronotherapeutic,9 enteric or colonic release,10 biphasic pharmacokinetic profile,11,12 and floating bioadhesive dosage form to present a sustained pharmacokinetic profile.13,14 Minitablets have also been shown as a potential dosage form for companion animals.15
For pediatric patients, minitablets allow the delivery of an ageappropriate dosage form to children as young as six months.16-19 The ability to adjust the dose by varying the number of minitablets administered allows the use of the same primary dosage form in different pediatric age groups. Minitablets can also be mixed with soft foods during administration to younger pediatric patients20 or patients who have swallowing difficulties (dysphagia). The small size of minitablets enables rapid disintegration times, which permits their use as an orally disintegrating dosage form if properly formulated,21 and allows their dispersion in liquid prior to administration. And for disease areas where the treatment paradigm requires the use of a combination product (e.g. infectious diseases), minitablets containing separate actives can be formulated, and then combined either in a capsule or sachet during packaging for a combination product presentation to the patients.
Despite potential advantages with minitablets, there are also potential challenges in working with this dosage form. Due to their small size, minitablets are not easy to handle individually. Thus, minitablets may not be the appropriate dosage form for patients with motor impairment or geriatric patients, unless administered with the help of a caregiver or a dosing device. Caution should be exercised when designing minitablets for compounds with relatively low threshold for toxicity (highly potent compounds). Stray minitablets can be more easily dropped and lost relative to larger tablets, which may then lead to inadvertent loss of dose or accidental ingestion by children or pets, although these risks can be mitigated through the appropriate choice of package presentation. In contrast, difficulty may also be encountered when designing a minitablet-based dosage form for high-dose drugs (compounds with low potency), since the number of minitablets per dose can be prohibitively large. From a manufacturing perspective, multiple minitablets have to be packaged together to provide a single dose, which lowers the dose-based production rate. As such, minitablets seem best implemented for small volume, highvalue products, especially for specific patient populations that would benefit from their distinguishing features.
The remainder of this paper reviews some of the potential opportunities and challenges in designing minitablets as a drug product, including manufacturing, packaging, and performance assessment.
Manufacturing and Packaging of Minitablets
Compression of Minitablets
Minitablets are generally manufactured by compression using a rotary tablet press.22 Multi-tip tooling is typically used for two reasons. First, it increases the production throughput and reduces the dwell time of the powder in the feed frame that can lead to over-lubrication or powder segregation. Second, by increasing the number of tips, the force applied to one pair of opposing punch tips is multiplied by the number of tips, resulting in an overall larger compression force that can be more accurately controlled.
Multiple-tip punches are available from tableting tool suppliers as multiple-part assemblies and as monoblocks. Monoblock punches offer faster tooling installation and easier cleaning, can be manufactured to tighter tolerances, as well as are more resistant to tip breakage than assembled multiple part tooling. However, multiple-part punches allow the replacement of damaged punch parts. Multi-tip tooling in general must meet tighter requirements for machining and mechanical stability compared to larger tablet tooling, and are more labor-intensive to manufacture, which leads to higher production costs.
The approximate compression weights for round minitablets with 2, 3, and 4-mm diameters are 7, 20, and 40 mg, respectively. Minitablets with height-to-width ratios close to one are desirable, as this will aid in packaging and dispensing. A deeper cup design may be beneficial for packaging, since it leads to more spherical minitablets. However, minitablets compressed with deeply concaved tooling can have larger tablet density gradients compared to standard or shallow concave designs. Such gradients can lead to tablet attrition during coating, packaging, or other handling steps. The use of tapered die designs can aid in decreasing residual stresses, resulting in smaller or fewer microdefects and more robust minitablets.
Effects of Powder Blend Flow Property and Particle Size on Minitablet Weight Uniformity
 Figure 2. Different designs exist for minitablet multi-tip tooling, such as multiple part cap-and-pin design (left) and monoblock (center). In a monoblock design, all tips are machined from one piece of stainless steel. Minitablet tooling can also be produced with different shapes and varying number of tips (right). The upper punch for minitablet tooling is keyed to maintain its rotational orientation. Pictures are courtesy of The Elizabeth Companies.
Figure 2. Different designs exist for minitablet multi-tip tooling, such as multiple part cap-and-pin design (left) and monoblock (center). In a monoblock design, all tips are machined from one piece of stainless steel. Minitablet tooling can also be produced with different shapes and varying number of tips (right). The upper punch for minitablet tooling is keyed to maintain its rotational orientation. Pictures are courtesy of The Elizabeth Companies.The weight uniformity of minitablets is crucial because it impacts content uniformity and dosing accuracy. The tolerance for weight variability in minitablets is smaller than for larger tablets, since small absolute weight variations will lead to more significant relative variations in potency. Among the factors that contribute to tablet weight variability, the flow of the powder is one of the most important. A systematic study was undertaken to evaluate the impact of variations in powder flow properties to weight uniformity of 2- and 3-mm minitablets. In this study, placebo formulations composed of lactose monohydrate, microcrystalline cellulose, croscarmellose sodium, and magnesium stearate were prepared. By varying the ratio of different grades of lactose monohydrate, blends with different flow properties (as evidenced through variations in Flodex values from 15 to 26) were prepared. Minitablets were then compressed via direct compression using seven- tip round standard concave 2- and 3-mm punches installed on a tablet press equipped with a two-paddle feeder mechanism. The tablet press speed was varied from 5 to 25 RPM, while the feeder paddle speed was varied between 10 to 30 RPM in a full-factorial two-factor, two-level DOE approach with one center point (replicated). The weights of produced minitablets were assessed using appropriate top-loading analytical balances, and collected data were analyzed.
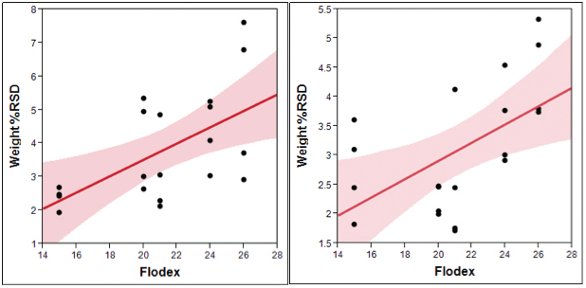 Figure 3. Statistically significant correlations were found between minitablet weight % relative standard deviation (%RSD) and Flodex values for (left graph) 2-mm and (right graph) 3-mm minitablets. The shaded region represents weight %RSD prediction interval with a=0.05.
Figure 3. Statistically significant correlations were found between minitablet weight % relative standard deviation (%RSD) and Flodex values for (left graph) 2-mm and (right graph) 3-mm minitablets. The shaded region represents weight %RSD prediction interval with a=0.05.The results obtained from this study showed a correlation between the flow property of the blend as indicated by Flodex values and tablet weight %RSD (P-values of 0.0069 and 0.0106 for 2- and 3- mm minitablets, respectively). Powder blends that were less free-flowing, as evidenced by higher Flodex values, yielded progressively greater minitablet weight variability upon compression, and this effect was more pronounced for the smaller minitablet tooling. Thus, to minimize minitablet weight variability, it is important to ensure good flow properties of the final blend. In this study, no statistically significant correlations were found between weight %RSD and press speed or feeder paddle speed.
The flow properties of powder blends are affected by particle attributes such as size, shape, surface roughness, and surface energy.23 In compression of larger tablets, larger particles can typically achieve better flow, which will result in lower weight variability. For blends containing small particles, size enlargement to improve flow properties can be accomplished via granulation (e.g. fluid bed granulation, high-shear granulation, or roller compaction). In the case of minitablets, it is important to balance the need to improve the flow properties through granulation with the impact of particle size on die fill uniformity. Typically, the optimum ratio of particle-todie diameter to minimize weight variability in tablet compression is between 1:20 to 1:30.24-25 A large proportion of particles larger than the optimum ratio in minitablet manufacturing can subsequently lead to increased tablet weight variability.
Film Coating of Minitablets
Two methods of film coating can be applied to minitablets: pan coating and Würster coating. Pan coating is commonly used to coat larger-sized tablets, and can also be employed for minitablets. The only difference is that the size of the perforations in the coating pan should be designed so as to allow proper venting, while at the same preventing the minitablets from passing through them. To achieve this, pans with small openings or solid wall pans should be used.26 In Würster coating, the minitablets are circulated in a vertical expansion chamber equipped with the Würster column, while the coating solution is sprayed from an upward-pointing gun. Since this process is commonly used for coating round pellets, no extensive adjustments are needed for the equipment to coat similarly-sized minitablets.
Regardless of the coating method employed, minitablets with suitable hardness and friability should be used for successful coating application. In addition, the appropriate process parameters (e.g. fluidizing or drying air flow rate, drying air temperature and relative humidity, spray rate, atomization pressure, etc.) should be carefully evaluated, and the specific values will vary depending on the equipment, batch size, and the type of coating formulation employed.
When compared against other multiparticulate systems such as pellets, microspheres, and granules, minitablets have more uniform sizes and porosities, narrower size distributions, smoother surfaces, and higher tensile strengths, which lead to more reproducible coating. The uniform sizes and smoother surfaces of minitablets lead to 2.5 -3 times lower levels of functional coating needed when compared against granules.27 However, the surface area-to-volume ratio for a 2-mm minitablet with 2 mm thickness varies from 2.9 to 3.0 mm-1 (see Figure 4). These values are significantly larger than for a typicalsized tablet (for example, the surface area-to-volume ratio for a 10 mm round tablet with 5 mm thickness is 0.8 mm-1). Thus on a weight gain basis, the amount of coating material deposited on a batch of 2-mm minitablets would be approximately four times larger than what is needed by larger tablets to achieve the same coating thickness, leading to the need for coating weight gains of up to 10-15%.
 Figure 4. Surface-area-to-volume ratio of 2-mm minitablets with different cup depth designs. As the cup depth decreases from deep or standard concave minitablets to shallow concave and further to flat (cylinders with no concave), the surface area-to-volume ratio also increased for the same diameter, and larger coating weight gain is needed to achieve the same coating thickness.
Figure 4. Surface-area-to-volume ratio of 2-mm minitablets with different cup depth designs. As the cup depth decreases from deep or standard concave minitablets to shallow concave and further to flat (cylinders with no concave), the surface area-to-volume ratio also increased for the same diameter, and larger coating weight gain is needed to achieve the same coating thickness.Functionalized Tablet Matrix and Film Coating Formulations
Different tablet matrix or film coating systems can be applied to minitablets depending on the desired functionalities. For example, tastemasking coatings may be important for certain active pharmaceutical ingredients (APIs) and/or for pediatric applications. This can be achieved by coating the minitablets using specially-designed taste-masking coating systems. If a sustained-release effect is desired as opposed to a burst effect, a functional coating system that imparts a sustained drug release profile can be applied on the minitablets, or the solid dose matrix formulation approach can be utilized. The use of hypromellose polymer matrices or lipidic excipients such as glyceryl dibehenate have been shown to achieve these effects. 7,28
Packaging of Minitablets
A variety of packaging options is available for minitablets, and selection of the appropriate package presentation depends on the product design criteria or the target product profile. If flexible dose adjustment with fine granularity is not needed, then the minitablets can be encapsulated or packaged into unit-dose presentations such as stick-packs or sachets. Certain encapsulation machines offer the ability to perform filling based on counting. For example, dosing discs with cavities designed to be filled with minitablets are available for some encapsulators. This approach results in an accurate count of minitablets being filled into the capsules across a wide range of target fills.
The maximum number of minitablets that can be filled into each capsule depends on the size of the capsule and the minitablets, and are listed in Table 1 for 2-mm minitablets.
Table 1. The Number of 2-mm Minitablets that can be Filled into Capsules of Different Sizes

Another type of unit-dose packaging suitable for packaging relatively large numbers of minitablets are stick-packs and sachets. For the purpose of this discussion, these two types of packaging are considered together, with the main difference being the fill volume: stick-packs have smaller fill volumes, whereas sachets have larger fill volumes. As with encapsulation, sachet and stick-pack packaging requires specific equipment. The selection of capsules vs. sachets/ stick-packs for bulk minitablet packaging may depend on a number of factors, as illustrated in the following table.
Table 2. Considerations for Selecting Capsules or Sachets/Stick-packs for Packaging of Minitablets

When rapid dose adjustment with fine granularity is needed, as in clinical trials, for example, then a measuring or dispensing device can be utilized in place of capsules of sachets. Measuring or dispensing devices vary in their capabilities and complexities. A relatively lowcomplexity device is a measuring spoon, which is a passive device used to assist in counting the required number of minitablets. The plastic spoon is fabricated with cavities corresponding to the number of minitablets needed for one dose. One step up in complexity are manual counting and dispensing devices. More complex devices can incorporate electronic controls and be automated, which can potentially achieve individualized dosing.29 With increasing complexity, more options can be included, such as an increased number of minitablets per dose, or the possibility of dispensing two or even more products simultaneously.
Assessing the Quality and Performance of Minitablets
Since compression of minitablets can be considered as analogous to the compression of larger tablets, it is important to properly characterize the powder blends and produced tablets. Evaluation of the physical and analytical properties of the powders and produced minitablets can help define the optimum formulation composition and processing window, and can be leveraged to assess manufacturing risks.30 Many of the tests applied to larger-sized tablets can also be employed for minitablets, although some modifications may be needed. These techniques, as well as application and modifications required for minitablets, are discussed below.
Physical Properties of Powder Blends and Produced Minitablets
As in the case of larger tablets, proper characterization and optimization of powder blends used in the manufacturing of minitablets is needed to ensure that quality products can be produced. The properties of the powder blends that should be characterized include densities (bulk density/BD and tapped density/TD), flow properties, and segregation potential. All these tests can be performed as discussed in Compendial standards for larger sized tablets, although few published studies highlight how results produced with these methods apply to minitablets.
After the minitablets are produced, properties such as weight, tensile strength, disintegration time, friability, as well as uniformity and quality of coating need to be assessed. Weight and tensile strength tests can be done using methods applied to larger tablets; however such is not the case for the disintegration test. The size of the screen opening specified in US Pharmacopeia Chapteras <701> as 2.0 mm is too large for most minitablets, so the screens in the disintegration tester should be replaced by screens with smaller openings. It should be noted, however that the disintegration of minitablets can be much more rapid than that of larger tablets, and although an assessment of minitablet disintegration time can be performed as described, its value may be limited. It may instead be more informative to directly assess the dissolution rate of the API from the finished dosage form.
Friability is another measure of tablet strength and integrity. As described in US Pharmacopeia Chapter <1216>, it is performed by placing a set amount of tablets into a wheel-like apparatus rotated at a set speed for a set amount of time (e.g. 25 RPM for 20 minutes), which subjects the tablets to a defined number of drops from a defined height. After removing any loose dust, the tablets are weighed, and the percentage weight loss as a function of the initial weight is determined. While this technique can be applied to minitablets, the results obtained may be misleading. Since the weights of minitablets are low, they are prone to static build-up, and may not properly tumble during the measurement. Variations of this test for minitablets include increasing the number of rotations, or adding glass beads or other objects inside the friabilator wheel while performing the test. The potential difficulty with applying such alterations to the testing method is how to correlate the results obtained to gauge the risk of chipping or other defects during minitablet processing and handling such as during coating, packaging, or shipping.
Lastly, imaging techniques can be applied to evaluate the structural integrity of minitablets, as well as the thickness and uniformity of coatings applied. One such technique is X-ray computed tomography (xRCT). This technique can be applied to non-invasively image the tablets31 to allow inspection of potential defects, coating thickness, and coating uniformity. Other techniques that can be utilized include terahertz (THz) spectroscopy, and light or scanning electron microscopy imaging.
Content Uniformity and Dissolution Testing
Content uniformity (CU) testing (US Pharmacopeia Chapter <905>, Uniformity of Dosage Units) is performed to demonstrate the consistency of API content within individual dosage units. For larger tablets, CU testing is applied to single tablets. For minitablets, considering a patient dose may consist of multiple minitablets, a determination must be made on the number of minitablets to be considered as one unit for the purpose of CU testing. This determination should take into account the stage of the project and the purpose of the testing. Most often, the work undertaken will fall into one of the following three categories:
- Formulation development and optimization
- Early phase clinical trials
- Late phase clinical trials and commercialization
To best support formulation development and optimization, testing each minitablet as a single unit can provide useful insight. Individual minitablet testing will afford the greatest amount of scrutiny, thereby providing the most useful information to drive formulation selection, development and optimization. However, testing individual minitablets greatly increases the risk of out-of-specification results, if this methodology was used as a product release test.
By the time of late phase clinical trials and commercial product testing, the intended doses are typically well established. These doses should drive the decision for the number of minitablets required for testing. Specifically, the number of minitablets per dose can be considered as one unit for the purposes of CU testing. If one lot of minitablets is to be packaged in multiple configurations, then the lowest minitablet count (i.e. the lowest dose) can be used as one unit for the release of the batch.
During support of early phase clinical trials, the choice can be less clear. The primary consideration is that the amount of minitablets included in one unit should be similar to the lowest planned clinical dose. In cases where the dose is known, then CU testing should proceed just as for late phase clinical trials as discussed above. In cases where a wide potential range of doses are being considered, a unit should be defined as the number of minitablets at or near the low end of the potential range. In the absence of definitive dose information, five minitablets per unit is recommended as a default for initial clinical release testing.32 Unless the clinical plan involves dosing a single minitablet per patient, testing CU on individual minitablets represents an unnecessary regulatory risk and should be avoided as a product release strategy.
Many of the considerations for dissolution testing of minitablets are the same as for other traditional oral dosage forms, including media selection, choice of baskets or paddles, and determination of paddle/ spindle rate. Further discussions here cover additional considerations and potential issues that are specific to minitablets. As with CU, the number of minitablets per unit is an important consideration. For dissolution testing, this determination should be made based upon the phase of development cycle and the type of testing: formulation development, or quality control (QC) dissolution testing (for stability assessment and release testing).
During formulation development and optimization, dissolution data should be generated in multiple minitablet counts. The lowest and highest number of minitablets to be dosed in animal or clinical studies should be evaluated according to the dissolution methodology, so as to provide a better context for the appropriate interpretation of pharmacokinetic (PK) results. Additionally, dissolution tests done on single minitablets can provide information on the variability of the material produced.
It is recommended that QC dissolution testing, whether for release or stability testing, aligns with the CU test in terms of the number of minitablets per unit. In addition to practical reasons for alignment, the decision criteria applies are the same for the CU and dissolution tests. Testing the number of minitablets per vessel at the lowest dose will provide more information as to the expected variability than testing at the highest dose. Dissolution profiles should also be generated at the highest dose planned for clinical trials, to ensure the consistency of the dissolution profiles across the expected dose range.
In the case of minitablets produced in support of a pediatric program, a comparison against the adult formulation should be performed prior to any bioavailability (BA) study. In pediatric development programs, alignment of the dissolution testing methodology with the adult program should be considered, but is not explicitly required. Due to the lower doses used in pediatrics, the QC methodology for the adult product may be inappropriately aggressive or perhaps indefensible for the dissolution testing of minitablets, either with respect to rotational speed or media composition, for example. When possible, similar methodology can be used between the adult and pediatric products; for example: using the same pH, but a lower surfactant level for the lower-dosed pediatric product.
In many instances, minitablets may employ film coating. For film coating systems applied to provide taste-masking, pH-dependent solubility may be inherent to the coating system, which can present challenges during the development of the testing method, especially if the matrix or API formulation also has pH-dependent solubility. In cases with conflicting pH-dependent solubility profiles, a dissolution design-of-experiment (DOE) study is recommended to understand the performance of coated and uncoated minitablets across the relevant pH range. It is also important to remember that both film coating and matrix dispersion can be influenced by increasing the ionic strength of the media. While it is not necessary for the dissolution of the coated and uncoated tablets to match per se, it is beneficial to understand the impact of the film coating on the dissolution results, so that the impact of other formulation changes may be better understood.
As minitablets smaller than 2.5 mm can be considered as oral granules, dissolution testing may not be a part of the required regulatory specification. However it is recommended to develop the necessary method and build the knowledge per the recommendations above to help guide formulation development and optimization. The dissolution test results can be maintained as internal targets against which to compare future batch data so as to gain further product understanding.
In-Use Analytical Testing
It is sometimes beneficial to allow dosing of minitablets with soft foods to help with swallowing. For the finished commercial products, the ideal situation is if the product can be incorporated into as wide a range of soft foods as possible. However, in support of a clinical study, it may be desirable to carefully select a food which will ensure that the minitablet remains intact in the food, so that the pharmacokinetics of the formulations can be reliably measured.
Prior to the clinical dosing, the mechanical integrity of minitablets under conditions which mimic the dosing instructions can be evaluated by means of an in-use test. An example of the procedure for such a test is as follows:
- Select the relevant number of minitablets and the volume, or mass, of soft food to be evaluated.
- Add the minitablets into the food (see Figure 5a), and stir for the proscribed time. One sample for each time point should be prepared, and examples of recommended time points are 5 and 15 minutes.
- At the given time points, place the entire sample onto a sieve that has apertures in the range of e.g. 1.0-1.5 mm. Place a weigh boat behind the sieve, and use compressed air to push the soft food through the sieve, while retaining intact minitablets. Figure 5c shows material retained on the sieve, and Figure 5d shows material passed through the sieve. Intact minitablets will be retained on the sieve, while disintegrated minitablets will pass through the sieve and be assayed.
- A portion of the soft food from the weigh boat should be placed into a pre-weighed, wide-mouth volumetric flask. The amount of material and size of flask should be chosen to provide the desired concentration and the standard prepared to match. Efforts for full recovery should be made and to ensure reasonable accuracy, the sample mass should be at least 50% of the sample size for that time point.
- Sample preparation can be continued in a typical sample diluent using mixtures of aqueous and organic solvents. The selection of a higher detection wavelength can help reduce the chance of interfering peaks from the food. If interfering peaks are present, a longer chromatographic method or a higher detection wavelength may need to be employed.
- The percentage of API released as a function of time can then be calculated using methods similar to percent released of a dissolution test (with the mass of API added via the minitablets and the mass of food used in performing the test above).
 Figure 5. (a) The minitablets are mixed into soft foods for the in-use test. (b) After appropriate mixing, samples are placed onto sieves with appropriately-sized apertures. Compressed air can then be used to separate intact from disintegrated minitablets. (c) Intact minitablets will be retained on the sieve, while (d) disintegrated minitablets will be pushed through sieve apertures. The material that passed through the apertures can then be prepared for API content assay as a measure of percentage of minitablets that disintegrated into the food.
Figure 5. (a) The minitablets are mixed into soft foods for the in-use test. (b) After appropriate mixing, samples are placed onto sieves with appropriately-sized apertures. Compressed air can then be used to separate intact from disintegrated minitablets. (c) Intact minitablets will be retained on the sieve, while (d) disintegrated minitablets will be pushed through sieve apertures. The material that passed through the apertures can then be prepared for API content assay as a measure of percentage of minitablets that disintegrated into the food.The results from such in-use tests can ensure that the integrity of the minitablets is not compromised prior to ingestion, and can evaluate the effectiveness of functionalized coatings. When combined with dissolution tests, a complete analytical assessment of the quality and potential behavior of the minitablets can be achieved prior to preclinical or clinical dosing.
Concluding Remarks

From the discussions above, it is clear that minitablets present a unique dosage form. First and foremost, minitablets appear to be a very promising dosage form for pediatric patients. Beyond that, minitablets also have potentials in modified and controlled release applications, for therapeutic areas where dysphagia is one of the symptoms, even or rapid dose adjustments and treatment personalization during clinical trials or beyond. The manufacturing techniques needed to produce robust minitablet-based dosage forms are extensions of typically employed unit operations such as compression, Würster or pan coating, and encapsulation. And while the finish product may be labelled as oral granules, analytical and preformulation tests similar to those employed during the development of larger tablets, e.g. flow property assessment and dissolution testing, can provide useful insights to help direct the development efforts. Due their unique size, some adjustments to the manufacturing process steps and analytical testing may be required, but these challenges should not detract from the opportunities offered by this unique dosage form.
Acknowledgements
The authors wish to thank Ronald Smith, Karen Thompson, Christopher Granelli, Matt Bolton, Jerry Klinzing, and Adam Procopio for their input and helpful discussions in preparing this paper. Anthony Pecora and Paul Sakowicz are thanked for minitablets manufacturing support.
References
- Tissen C, Woertz K, Breitkreutz J, Kleinebudde P. Development of mini-tablets with 1 mm and 2 mm diameter. Int J Pharm. 2011;416(1):164-170.
- Guidance for Industry: Size of Beads in Drug Products Labeled for Sprinkle. In: U.S. Department of Health and Human Services FDA, Center for Drug Evaluation and Research (CDER); 2012.
- Aleksovski A, Dreu R, Gasperlin M, Planinsek O. Mini-tablets: A contemporary system for oral drug delivery in targeted patient groups. Expert Opin Drug Deliv. 2015;12(1):65-84.
- Munday DL, Fassihi AR. Controlled release delivery: Effect of coating composition on release characteristics of mini-tablets. Int J Pharm. 1989;52(2):109-114.
- Goole J, Amighi K, Vanderbist F. Evaluation and floating enhancement of levodopa sustained release floating minitablets coated with insoluble acrylic polymer. Drug Dev Ind Pharm. 2008;34(8):827-833.
- Goole J, Deleuze P, Vanderbist F, Amighi K. New levodopa sustained-release floating minitablets coated with insoluble acrylic polymer. Eur J Pharm Biopharm. 2008;68(2):310-318.
- Roberts M, Vellucci D, Mostafa S, Miolane C, Marchaud D. Development and evaluation of sustained-release Compritol® 888 ATO matrix mini-tablets. Drug Dev Ind Pharm. 2012;38(9):1068-1076.
- Mohamed FAA, Roberts M, Seton L, Ford JL, Levina M, Rajabi-Siahboomi AR. The influence of HPMC concentration on release of theophylline or hydrocortisone from extended release mini-tablets. Drug Dev Ind Pharm. 2013;39(8):1167-1174.
- Biswas N, Sahoo RK, Guha A, Kuotsu K. Chronotherapeutic delivery of hydroxypropylmethylcellulose based mini-tablets: An in vitro-in vivo correlation. Int J Biol Macromolec. 2014;66:179-185.
- Filho VJT, Andreazza IF, Sato MEO, Murakami FS. Development of a multiparticulate system containing enteric-release mini-tablets of omeprazole. Braz J Pharm Sci. 2014;50(3):505-512.
- Lopes CM, Lobo JMS, Pinto JF, Costa P. Compressed mini-tablets as a biphasic delivery system. Int J Pharm. 2006;323(1-2):93-100.
- Aleksovski A, Lustrik M, Sibanc R, Dreu R. Design and evaluation of a specific, bi-phase extended release system based on differently coated mini-tablets. Eur J Pharm Sci. 2015;75:114-122.
- Goole J, Vanderbist F, Amighi K. In vitro evaluation of two concepts of sustained release floating minitablets according to the model drug used. J Drug Deliv Sci Technol. 2008;18(2):133-138.
- Zhu X, Qi X, Wu Z, Zhang Z, Xing J, Li X. Preparation of multiple-unit floating-bioadhesive cooperative minitablets for improving the oral bioavailability of famotidine in rats. Drug Deliv. 2014;21(6):459-466.
- Hautala J, Airaksinen S, Naukkarinen N, Vainio O, Juppo AM. Evaluation of new flavors for feline mini-tablet formulations. J Excipients and Food Chem. 2014;5(2):81-99.
- Spomer N, Klingmann V, Stoltenberg I, Lerch C, Meissner T, Breitkreutz J. Acceptance of uncoated mini-tablets in young children: Results from a prospective exploratory cross-over study. Arch Dis Child. 2012;97(3):283-286.
- Klingmann V, Spomer N, Lerch C, et al. Favorable acceptance of mini-tablets compared with syrup: A randomized controlled trial in infants and preschool children. J Pediatr. 2013;163(6):1728-1732.e1721.
- Preis M. Orally Disintegrating Films and Mini-Tablets - Innovative Dosage Forms of Choice for Pediatric Use. AAPS Pharm Sci Tech. 2015;16(2):234-241.
- Thomson SA, Tuleu C, Wong ICK, Keady S, Pitt KG, Sutcliffe AG. Minitablets: New modality to deliver medicines to preschool-aged children. Pediatrics. 2009;123(2):e235-e238.
- Sznitowska M, Kluk A, Brandt A, et al. Can preschool-aged children swallow several minitablets at a time? Results from a clinical pilot study. Int J Pharm. 2015;485(1-2):1-6.
- Stoltenberg I, Breitkreutz J. Orally disintegrating mini-tablets (ODMTs) - A novel solid oral dosage form for paediatric use. Eur J Pharm Biopharm. 2011;78(3):462-469.
- Qiu Y, Zhang G. Chapter 21 - Development of Modified-Release Solid Oral Dosage Forms. In: Qiu Y, Chen Y, Zhang GGZ, Liu L, Porter WR eds. Developing Solid Oral Dosage Forms 1st ed. Cambridge, MA: Academic Press; 2009:501-517.
- Prescott JK, Barnum RA. On powder flowability. Pharm Technol. 2000;24(10):60-84+236.
- Arambulo AS, DeardorffDL. Compressed tablets, average weight. J Am Pharm Assoc. 1953;42(11):690-691.
- Arambulo AS, Fu HS, DeardorffDL. Compressed tablets; weight variation. J Am Pharm Assoc. 1953;42(11):692-694.
- Passerini N, Albertini B, Rodriguez L, Funaro C, Mondelli G. Directly compressed mini-tablets coated in a solid-wall pan for sustained drug release. 10th World Meeting on Pharmaceutics, Biopharmaceutics, and Pharmaceutical Technology; 2012.
- Munday DL. A Comparison of the Dissolution Characteristics of Theophylline from Film Coated Granules and Mini-Tablets. Drug Dev Ind Pharm. 1994;20(15):2369-2379.
- Mohamed FAA, Roberts M, Seton L, Ford JL, Levina M, Rajabi-Siahboomi AR. Production of extended release mini-tablets using directly compressible grades of HPMC. Drug Dev Ind Pharm. 2013;39(11):1690-1697.
- Bredenberg S, Nyholm D, Aquilonius SM, Nyström C. An automatic dose dispenser for microtablets - A new concept for individual dosage of drugs in tablet form. Int J Pharm. 2003;261(1-2):137-146.
- Tehseen N, Rao V, Hadi MA. Design and characterization of twice daily mini-tablets formulation of Pregabalin. Int J Pharm Pharm Sci. 2013;5(SUPPL.1):168-175.
- Zeitler JA, Gladden LF. In-vitro tomography and non-destructive imaging at depth of pharmaceutical solid dosage forms. Eur J Pharm Biopharm. 2009;71(1):2-22.
- Flanagan F, Kozlowski B, Hein E, Romberger G, Do M. Utilization of Automation to Enhance and Facilitate Development of a Mini-Tablet Formulation. Amer Pharm Rev. 2015;18(6):98-102.