School of Pharmacy, Temple University
School of Pharmacy, Temple University
Introduction
In recent years, many scientists in the pharmaceutical industry are focusing part of their research activity on the development and use of oral strip technology (OST)1. Medicated oral strips can be used for local effect2,3, rapid release and absorption as well as controlledrelease systemic drug delivery via mucoadhesive principles4-6. The advantages of OST include the ease of administration especially for pediatric and geriatric patient population who may have the difficulty of swallowing larger oral dosage forms. It also offers an alternative platform for molecules that undergo hepatic first-pass metabolism and avoids the drug degradation and pre-systemic elimination within the gastrointestinal tract7,8. Table 1 lists some commercially approved oral strip products for transmucosal drug delivery. However, development of oral strip with high drug content uniformity, uniform appearance and adequate physical and mucoadhesive strength remains a challenge for pharmaceutical scientists especially when the drug dose is high. Furthermore, lack of standardized test methods and monographs in the US Pharmacopeia (USP) makes it more difficult to develop and compare different oral strip products in terms of their dissolution performance, formulation differences, excipient effects and regulatory assessment.
Table 1. Examples of marketed oral strip products for transmucosal drug delivery
Production of Medicated Oral Strips
Oral strips are usually prepared by conventional casting methods in which the solution or emulsion of the polymers, drug and other excipients including plasticizers, sweeteners, surfactants, preservatives, salivary stimulating agents etc. are poured into a suitable mold and allowed it to dry. This process usually consists of six steps including: preparation of casting solution; deareation of the solution; transfer of the prepared solution into an appropriate mold with defined depth and volume; drying the deposited polymeric film; cutting the prepared oral film into the desired size; and packaging of the final oral strip product. When manufacturing the oral strips using the casting method, particular attention must be given to the rheological properties of the casting solution, absence of entrapped air bubbles, film uniformity and content uniformity in the final dosage form.
Oral films can also be prepared by using other technologies such as direct compression and hot-melt extrusion (HME)9,10. The advantages of using the HME technique is that it avoids the use of water or other organic solvents and therefore expedites the drying process. However, it is undesirable for heat labile drugs and the mixing is less homogeneous compared to preparation of a drug-polymer solution.
In-vitro Characterization of Medicated Oral Strips
Characterization of critical properties such as the mechanical strength, drug content uniformity, dissolution rate and permeation rate represent some of the major research areas in the design of oral strips.
Content uniformity is a major challenge associated with the conventional solvent casting method. Historically production of films have suffered from particle aggregation and non-uniformity due to the large number of excipients used in their formulation including, soluble polymers, surfactants, flavors, sweeteners, plasticizers, preservatives and drugs. Yang et al. indicated that self-aggregation was one of the main causes of poor uniformity and in particular the relatively long drying time was found to facilitate intermolecular attractive forces, convection forces, air bubbles and the like to form such aggregation11. The formed agglomerates randomly distribute inside the cast film and result in an inaccurate amount of active ingredient inside each strip after the cutting process. In order to obtain uniform oral strips, many attempts have been made such as optimization of film composition, addition of viscous agents such as gel formers or polyhydric alcohols12,13, use of controlled drying process for example radiation drying11. Furthermore other techniques for determining drug content assay, such as X-ray diffraction, and scanning electron microscopy can be used to evaluate the content uniformity of oral strips.
Non-aggregating strips are characterized as an amorphous state with the absence of significant sharp peaks during X-ray diffraction (XRD) analysis. A rough and uneven surface with lumps in the microscopic or SEM images of oral strips is an indicator of self-aggregation and nonuniformly dispersed formulation.
The determination of properties of polymeric films including oral strips is based on standard mechanical testing methods as presented in this work using textural analyzer (Figure 1)14. During the tensile testing, the oral strip was mounted between two clamps and the stressstrain curve (or load-time profile) was recorded when the strips were pulled by the top clamp at a fixed rate. From the stress-strain curve, the tensile strength, percentage elongation at break and the elastic modulus (also known as Young’s modulus) are calculated.
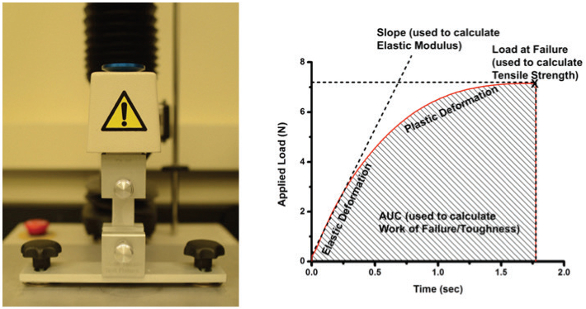 Figure 1. Texture analyzer equipped with grips for measuring the mechanical properties of oral strip (left) and typical load-time profile of oral strip under mechanical stress (right).
Figure 1. Texture analyzer equipped with grips for measuring the mechanical properties of oral strip (left) and typical load-time profile of oral strip under mechanical stress (right).Despite intensive work on oral strip technology, there is no official standardized method or monograph in the US Pharmacopeia (USP) for evaluating its “in vitro dissolution” behavior. Most of the studies have used the paddle over disc method (similar to USP apparatus 5) to assess the release of drug from the prepared films10,15. Briefly, the film is fixed on a glass plate and is immersed in the dissolution medium below the paddle and the paddle is rotated at a fixed rotation per minute (rpm) speed. Nevertheless, in most of the studies the provision has been made such that the drug release occurs from a single side of the strip. This is inconsistent with the real situation “in vivo” where the drug release can happen from both sides of the oral strip. Therefore, our lab is proposing a modified UPS Apparatus II with double mesh assembly to be considered for dissolution testing of oral-soluble films. The double mesh design allows the free drug release from both sides of the oral strip. It also allow allows an easy switch from 2-side to 1-side release by simply incorporated another plastic film between the bottom mesh and the oral strip. This design offers more flexibility compared to other methods (Figure 2).
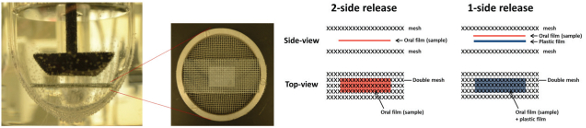 Figure 2. Modified UPS Apparatus II with double mesh assembly used for dissolution testing of oral-soluble films and illustration of 2-side and 1-side release design.
Figure 2. Modified UPS Apparatus II with double mesh assembly used for dissolution testing of oral-soluble films and illustration of 2-side and 1-side release design.Experimental Section
Materials and methods
In one of the studies, we developed a new postage stamp size oral strip of water-soluble model drug tramadol HCl using the casting method according to the formula shown in Table 2. The aqueous solutions of each component were thoroughly mixed with the help of a glass mortar and pestle then poured into the glass/plastic molds with defined depth and dried inside the hood for 14 hours. The resultant films were cut into stamp size (2.5 cm×1.75 cm) oral strips having final composition (w/w) of 21.78% API (tramadol HCl), 4.95% carbopol, 49.5% PEO, 4.95% HPMC, 3.96% glycerol, 9.9% mannitol/sorbitol and 4.95% citric acid in the dry form. The dissolution studies of prepared stamp size oral strips were carried out using modified UPS apparatus II (paddle with double mesh assembly) (Figure 2) at a stirring speed of 25 rpm and 50 rpm in 500 ml simulated saliva (pH 6.8) at 37 ºC. The samples were withdrawn at predetermined time intervals and the percentage dissolved of the drug was determined using a UV spectrophotometer at 271 nm. The rheological properties of the films such as tensile strengths, percent elongation, viscoelasticity, structural recovery were evaluated using a computerized textural analyzer.
Table 2. Compositions of studied tramadol HCl oral strips.

Results and Discussion
The resultant stamp-size oral films have an average weight of 0.08g and average thickness of 140 μm. On exposure to modified dissolution testing, the oral strips quickly hydrated and about 80% of the drug was released within 15 minutes at a stirring speed of 25 and 50 rpm irrespective of the type of mesh device assembly used (i.e. 2-side or 1-side release) (Figures 3 and 4). More consistent and slower release was apparent when only one side of the film was exposed to dissolution medium.
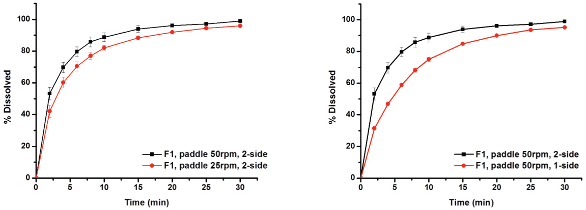 Figure 3. Dissolution profiles of tramadol-HCl oral strip (Formulation 1) using modified dissolution apparatus II with inserted double-mesh assembly at stirring speed of 50 rpm and 25 rpm. Drug release was occurring from 2-side and 1-side of oral strip.
Figure 3. Dissolution profiles of tramadol-HCl oral strip (Formulation 1) using modified dissolution apparatus II with inserted double-mesh assembly at stirring speed of 50 rpm and 25 rpm. Drug release was occurring from 2-side and 1-side of oral strip.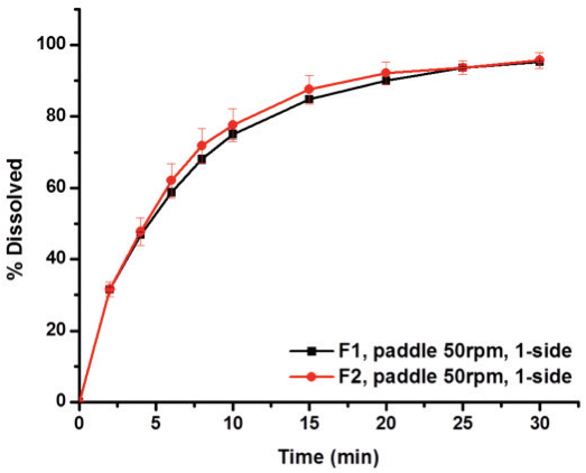 Figure 4. Comparison of dissolution rate of tramadol-HCl from Formulation 1 and 2 when only one side of film was exposed.
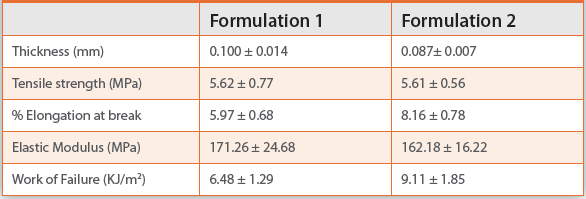
Figure 4. Comparison of dissolution rate of tramadol-HCl from Formulation 1 and 2 when only one side of film was exposed.Textural analysis of the prepared oral strips (without tramadol-HCl) showed acceptable physical properties with tensile strength around 5.62 MPa, percent elongation at break of about 5.97% and 8.16% under studied condition (Table 3).
Table 3. Mechanical properties of studied oral films (mean ± SD, n=6)
Conclusion
This study highlights the importance of content uniformity and in vitro characterization of oral strips using mechanical testing techniques and proper dissolution methodology. As described in the experimental section, a stamp-size oral-soluble film with non-self-aggregating characteristics was successfully developed with acceptable viscoelasticity, physical strength and release of ≥80% of the drug within 15 minutes using a casting method. Due to the ease of administration and avoidance of hepatic first-pass metabolism, oral strip technology has been explored extensively during the last decades. The goal is to overcome some of the disadvantages associated with conventional oral drug delivery where drug and the dosage form is extensively exposed to the milieu of the gastrointestinal tract with potential drug degradation, metabolism, slower onset effect and consequently lower bioavailability. Oral strips offer an alternative dosage form for patients having difficulty in swallowing of tablets or capsules and exhibit ease of administration and improved patient compliance. The oral strip technology is an ideal choice for administration of potent drugs used to treat acute conditions where rapid onset of action is required. The improvement of manufacturing processes and evaluation of oral strips presented in this work is expected to assist pharmaceutical scientists to produce oral strips with precise dose, better content uniformity and esthetically more attractive dosage forms for patients.
References
- 1. R.P. Dixit, S.P. Puthli. Oral strip technology: overview and future potential. Journal of controlled release, 139.2 (2009) 94-107.
- 2. S. Senel, G. Ikinci, S. Kas, A. Yousefi-Rad, M. Sargon, A. Hincal, Chitosan films and hydrogels of chlorhexidine gluconate for oral mucosal delivery, International Journal of Pharmaceutics 193 (2000) 197–203.
- 3. S. Singh, S. Jain, M. Muthu, S. Tiwari, R. Tilak, Preparation and evaluation of buccal bioadhesive films containing clotrimazole, AAPS Pharmaceutical Science and Technology 9 (2008) 660–667.
- 4. G. Chen, C. Bunt, J. Wen, Mucoadhesive polymers-based film as a carrier system for sublingual delivery of glutathione, Journal of Pharmacy and Pharmacology 67.1 (2015) 26-34.
- 5. C. Li, P.P. Bhatt, T.P. Johnston, Evaluation of a mucoadhesive buccal patch for delivery of peptides: in vitro screening of bioadhesion, Drug Development and Industrial Pharmacy 24 (1998) 919.
- 6. Y. Lee, Y. Chien, Oral mucosa controlled delivery of LHRH by bilayer mucoadhesive polymer systems, Journal of Controlled Release 37 (1995) 251–261.
- 7. C. Squier, P. Wertz, Structure and function of the oral mucosa and implications for drug delivery, in: M.J. Rathbone (Ed.), Oral Mucosal Drug Delivery, Informa Health Care, 1996.
- 8. A.H. Shojaei, Buccal mucosa as a route for systemic drug delivery: a review, J Pharm. Pharmaceut. Sci. 1 (1998) 15–30.
- 9. M. Repka, S. Prodduturi, S. Stodghill, Production and characterization of hot melt extruded films containing clotrimazole, Drug Development and Industrial Pharmacy 29 (2003) 757–765.
- 10. M.A. Repka, K. Gutta, S. Prodduturi, M. Munjal, S.P. Stodghill, Characterization of cellulosic hot-melt extruded films containing lidocaine, Eur. J. Pharm. Biopharm. 59 (2005) 189–196.
- 11. R.K. Yang, R.C. Fuisz, G.L. Myers, et al., Thin film with non-self-aggregating uniform heterogeneity and drug delivery systems made therefrom: U.S. Patent 7,425,292. 2008-9- 16.
- 12. M. Horstmann, W. Laux, S. Hungerbach. Rapidly disintegrating sheet-like presentations of multiple dosage units: U.S. Patent 5,629,003. 1997-5-13.
- 13. H.G. Zerbe, J.H. Guo, A. Serino. Water-soluble polymer; at least one member selected from the group consisting of a polyalcohol, a surfactant and a plasticizer; at least one cosmetic or pharmaceutically ingredient; and a flavoring agent: U.S. Patent 5,948,430. 1999-9-7.
- 14. L. Sievens-Figueroa, A. Bhakay, J.I. Jerez-Rozo, et al. Preparation and characterization of hydroxypropyl methyl cellulose films containing stable BCS Class II drug nanoparticles for pharmaceutical applications. International journal of pharmaceutics, 423.2 (2012) 496- 508.
- 15. L. Perioli, V. Ambrogi, F. Angelici, M. Ricci, S. Giovagnoli, M. Capuccella, C. Rossi, Development of mucoadhesive patches for buccal administration of ibuprofen, J. Control. Release 99 (2004) 73–82.