Robert Dream- Managing Director, HDR Company LLC
Cells are the basic building blocks of all living things, and genes can be found deep within cells. Genes are small sections of DNA that carry genetic information and instructions for making proteins, which help build and maintain the body. 29
Cells can control which genes get transcribed and which transcripts get translated. Further, they can biochemically process transcripts and proteins in order to affect their activity. Regulation of transcription and translation occurs in both prokaryotes and eukaryotes, but it is far more complex in eukaryotes.
As we describe the different approaches of cell and gene therapy we often say “genetic material” is used or delivered to cells. Genetic material is a broad term and there are different types that may be used.
Genetic Material
Genetic material most commonly refers to DNA or RNA. These are strings of molecules with the information to instruct cells to produce proteins. Proteins play an important role in how living things function.
DNA
DNA stores the genetic information so the cell can continue building proteins. It is permanent and stored in the nucleus in a form called chromosomes. DNA is made up of two strands and is much larger than RNA. Genes are specific sections of DNA that encode sequences (i.e., a set of instructions) for making proteins. Other sections of DNA can control when, where, and how much of the protein is made.
RNA
RNA is a copy of the genetic information contained within DNA. While DNA is the permanent storage format of genetic material, RNA molecules help turn those instructions into proteins. After RNA is made within the nucleus of a cell, most RNA moves to the cytoplasm, which is the fluid space between the nucleus and cell membrane. There are many different types of RNA. Some RNA carries the instructions for making proteins, while other types of RNA can prevent proteins from being made. RNA molecules are only active for a limited period of time in the cell.
Cell Therapy
Cell therapy refers to the transfer of autologous or allogeneic cellular material into a patient for medical purposes. Stem cells used or targeted by cell therapy can be grouped into three categories: pluripotent stem cells (PSCs), adult stem cells (ASCs), and cancer stem cells (CSCs).
Pluripotent Stem Cells - PSCs
Pluripotent stem cells (PSCs) are a group of cells that can maintain an undifferentiated state indefinitely and can differentiate into most, if not all, cells of the body.
PSCs give rise to all cell types except extraembryonic placental cells; they include embryonic stem cells (ESCs), found in the inner blastocyst cell mass of preimplantation embryos; epiblast stem cells (EpiSCs) and embryonic germ cells (EGCs), found in post implantation embryos; and induced pluripotent stem cells (iPSCs), derived from direct reprogramming of postnatal/adult somatic cells in vitro.1,2,3
Adult Stem Cells - ASCs
ASCs are rare, undifferentiated cells distributed among differentiated or specialized cells in organs of a developed organism.4 With more limited self-renewal and differentiation potentials than PSCs, ASCs replenish lost cells or contribute to the healing or growth of cells by giving rise to precursor or progenitor cells and ultimately differentiated cells.5 ASCs include hematopoietic stem cells (HSCs), skin stem cells (SSCs), neural stem cells (NSCs), and mesenchymal stem cells (MSCs).6 HSCs are mostly found in the bone marrow (BM) and give rise to all mature blood cells: red blood cells, white blood cells, and platelets.7 SSCs, such as epidermal stem cells and hair follicle stem cells, maintain skin integrity.8 NSCs are self-renewable stem cells found in the central nervous system and can give rise to nerve cells, oligodendrocytes, and astrocytes.9 MSCs are of mesodermal, non-hematopoietic origins and are present in multiple tissues, including BM, adipose tissue, peripheral blood, and placenta.10 They can differentiate into bone, cartilage, and fat cells, as well as cells of ectodermal or endodermal parentage.11,12 Unlike ESCs, which are mainly defined by their origin in embryos using molecular and functional assays, ASCs have varying defining criteria, with cell morphology and surface markers being the go-to in most experimental evaluations.5 However, morphology and surface markers of ACSs are generally indistinguishable from those of mature cells; therefore, ASCs cannot be readily isolated from tissues, but enriched to varying degrees of purity in tissue extracts.4,5 The use of ASCs is mainly observed with HSCs or MSCs and envelops several clinical fields.
Cancer Stem Cells - CSCs
CSCs, or tumor-initiating cells, are found within solid and blood tumors and originate from normal stem cells or progenitor cells by several proposed mechanisms, such as mutations, gene transfer, epigenetic alterations, and microenvironmental factors.13,14 CSCs possess self-renewal, differentiation, metastasis, and immunosuppressive properties and play an important role in cancer growth, metastasis, relapse, and resistance to chemotherapy and radiotherapy.14,15 Identification criteria of CSCs generally include surface protein markers (e.g., CD133, CD44, tumor-associated antigens) and metabolic/ functional properties: e.g., high metabolism, slow cell division; however, they might overlap with those of normal somatic/germ cells or of other stem cells.3 Generally, the clinical use of CSCs is seen in cancer settings and involves targeting CSCs by different signaling pathway-interfering agents that subsequently prevent cancer growth and relapse.16,17
Regulatory Considerations for Cell Therapy
Human cells, tissues, and cellular and tissue-based products (HCT/P) are defined by the FDA under Title 21 of the Code of Federal Regulations [21 CFR Part 1271.3(d)], as “articles containing or consisting of human cells or tissues that are intended for implantation, transplantation, infusion, or transfer into a human recipient.” Falling under this definition are several examples, including HSCs/progenitor cells derived from peripheral blood or Cord Blood (CB), manipulated autologous chondrocytes, and epithelial cells on a synthetic matrix. If the therapy does not meet the definition of HCT/P in 21 CFR 1271.3(d), such as blood components/derivatives; e.g., Platelet-Rich Plasma (PRP) and minimally manipulated Bone Marrow Aspirate (BMA), the regulations in 21 CFR Part 1271 do not apply.18
For therapies meeting the definition of HCT/P in 21 CFR 1271.3(d), the 21 CFR 1271.15(b) further guides how HCT/P are regulated. The “same surgical procedure (SSP) exception” in 21 CFR 1271.15(b) states that it is not required to comply with the requirements in 21 CFR 1271 if the establishment is collecting and administering the HCT/P autologously, within the same surgical procedure, and in their original form (if processed, only rinsing, cleansing, sizing, and shaping are allowed).18,19 Otherwise, the algorithm progresses to the requirements of 21 CFR 1271.10(a). The criteria under this title specify that the HCT/P is minimally manipulated; intended for homologous use; not combined with other active agents; without a systemic effect; and if with a systemic effect administered autologously or to first-/second-degree blood relatives.18 If these criteria are met, the FDA allows the use of the cell therapy in the framework of regulatory guidelines governing disease transmission, yet without premarket approval/biologics license application, solely under section 361 of the Public Health Service (PHS) Act and regulations in 21 CFR 1271. Otherwise, if the cell therapy does not meet the criteria under 21 CFR 1271.10(a), it is regulated as a biological product under the Federal Food, Drug, and Cosmetic (FD&C) Act and/or section 351 of the PHS Act and applicable regulations. In this case, the cell therapy would require premarket approval, and the establishment needs to register the therapy and apply for a biologics license for lawful marketing, or have an investigational new drug (IND) application in effect if the therapy is investigational.18,19
The importance of being well informed about the above regulations becomes more obvious with the recent aggressive enforcement the FDA has begun to undertake to protect patients from risks of unapproved products being otherwise dispensed as HCT/P falling under section 361 of the PHS Act and regulations in 21 CFR 1271. In May 2018, the FDA initiated an action against a stem cell clinic for administering non-compliant autologous Stromal Vascular Fraction (SVF) to patients. On June 3, 2019, the Florida court ruled in favor of the FDA because, according to the FDA arguments, the isolated SVF no longer represented adipose tissue (i.e., not in its original form, or adipose tissue) after removal from the patient, and because the therapeutic use of the SVF differed from the natural function of adipose tissue (i.e., not intended for homologous use). Although the stem cell clinic argued that CFR 1271.15(b) and 21 CFR 1271.10(a) apply to their SVF product, the court saw otherwise, considering the case as a violation of federal laws and the product as a “drug” falling under the FD&C Act and necessitating extensive pre-approval. On June 25, 2019, the court ordered the stem cell clinic to cease offering SVF services until further FDA compliance. In addition to that SVF clinic, the FDA has issued multiple warnings to other clinics working with stem cells and umbilical cord-derived products.20,21 Counterintuitively, a California federal judge has denied a government motion initiated simultaneously with the former lawsuit, against a stem cell treatment center. In the trial, the FDA argued that the center was using illicit SVF therapies that are manipulated prior to implantation to treat degenerative diseases. The manipulation according to the FDA occurred in the removal step of the adipose tissue, thus generating an SVF product to which the SSP exception does not apply. The defendant countered that their SVF is unaltered, despite the removal of adipose tissue, and thus complies with all requirements in 21 CFR Part 1271.22 In the hearing,23 the judge considered that the SSP exception is unambiguous and read that it does not require the reimplantation of all the removed tissue, much like coronary artery bypass procedures in which surgeons do not implant the removed blood and excess artery. Based on this logic, the judge considered that the SSP exception applies to the SVF product, whose natural host tissue was removed as part of the collection process without further alteration to the SVF content. The court saw that the FDA’s interpretation of the SSP exception is “unreasonable and creates enforcement inconsistency” and considered that “the agency’s reading must fall within the bounds of reasonable interpretation… a requirement an agency can fail.”23 These incidents are indicative that the FDA regulations governing the use of cell therapy products are confusing and might not be safe from misinterpretations or dispute.
On another note, other multicellular products, such as Bone Marrow Aspirate Concentrate (BMAC), have not received FDA warnings and continue to be used as HCT/P under section 361 of the PHS Act and regulations in 21 CFR Part 1271.
Gene Therapy
Gene therapy products are biological products regulated by the FDA’s Center for Biologics Evaluation and Research (CBER). Clinical studies in humans require the submission of an investigational new drug application (IND) prior to initiating clinical studies in the United States. Marketing a gene therapy product requires submission and approval of a biologics license application (BLA), Figure 1, and Table 1.
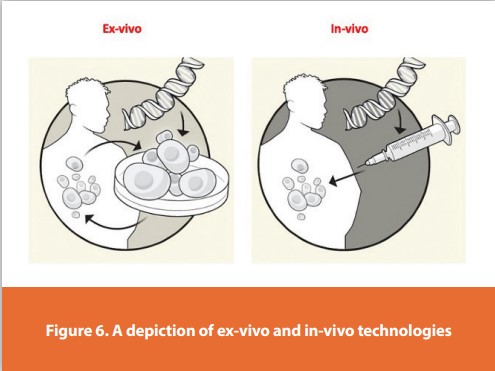
In vivo versus ex vivo therapies
In in-vivo gene therapy, a vector (typically, a virus) is introduced to the patient, which then achieves the desired biological effect by passing the genetic material (e.g., for a missing protein) into the patient’s cells, Figure 2 and Figure 3.
In ex vivo gene therapies, such as CAR-T therapeutics, Figure 4, the patient’s own cells (autologous) or healthy donor cells (allogeneic) are modified outside the body (hence, ex vivo) using a vector to express a particular protein, such as a chimeric antigen receptor.
In vivo gene therapy is seen as simpler, since it does not require the harvesting of mitotic cells. However, ex vivo gene therapies are better tolerated and less associated with severe immune responses, Figure 5, and Figure 6.


The concept and application of gene therapy is closely related to the idea of cell therapy, which can be roughly defined as an approach where cells are used as therapy or vehicle for therapy. Cell therapy has been used for many years, considering, e.g., blood transfusions and bone marrow transplants. Currently cell therapy has an enormous potential in regerative medicine, even without genetic modifications of the cells. The immunologic issues associated with cell transplants opened an opportunity for the combination of cell and gene therapy. Several clinical trials have involved both gene and cell therapies, where defective (or not) cells are isolated from patients, treated with the therapeutic gene (using the appropriate vector) Figure 1 and Figure 5, and then reinfused into the patient. There is a clear overlap between both strategies combined, they can be defined as a therapeutic intervention based on the administration of genetic material in order to modify or manipulate the expression of a gene product, altering the biological properties of living cells.
Human gene therapy seeks to modify or manipulate the expression of a gene or to alter the biological properties of living cells for therapeutic use,28 Table 2.
Gene therapy is a technique that modifies a person’s genes to treat or cure disease. Gene therapies can work by several mechanisms:
- Replacing a disease-causing gene with a healthy copy of the gene
- Inactivating a disease-causing gene that is not functioning properly
- Introducing a new or modified gene into the body to help treat a disease
Gene therapy products are being studied to treat diseases including cancer, genetic diseases, and infectious diseases. There are a variety of types of gene therapy products, including:
- Plasmid DNA: Circular DNA molecules can be genetically engineered to carry therapeutic genes into human cells.
- Viral vectors: Viruses have a natural ability to deliver genetic material into cells, and therefore some gene therapy products are derived from viruses. Once viruses have been modified to remove their ability to cause infectious disease, these modified viruses can be used as vectors (vehicles) to carry therapeutic genes into human cells.
- Bacterial vectors: Bacteria can be modified to prevent them from causing infectious disease and then used as vectors (vehicles) to carry therapeutic genes into human tissues.
- Human gene editing technology: The goals of gene editing are to disrupt harmful genes or to repair mutated genes.
- Patient-derived cellular gene therapy products: Cells are removed from the patient, genetically modified (often using a viral vector) and then returned to the patient.
Later studies led to advances in gene therapy techniques. A newer technique, called genome editing (an example of which is CRISPR-Cas9), uses a different approach to correct genetic differences. Instead of introducing new genetic material into cells, genome editing introduces molecular tools to change the existing DNA in the cell. Genome editing is being studied to:
- Fix a genetic alteration underlying a disorder, so the gene can function properly.
- Turn on a gene to help fight a disease.
- Turn off a gene that is functioning improperly.
- Remove a piece of DNA that is impairing gene function and causing disease.
Gene therapies are being used to treat number of diseases, including an eye disorder called Leber congenital amaurosis and a muscle disorder called spinal muscular atrophy. Many more gene therapies are undergoing research to make sure that they will be safe and effective. Genome editing is a promising technique also under study that doctors hope to use soon to treat disorders in patients.
Gene therapy is a technique that uses a gene(s) to treat, prevent or cure a disease or medical disorder. Often, gene therapy works by adding new copies of a gene that is broken, or by replacing a defective or missing gene in a patient’s cells with a healthy version of that gene, Table 2. Both inherited genetic diseases (e.g., hemophilia and sickle cell disease) and acquired disorders (e.g., leukemia) have been treated with gene therapy.
Gene therapy is a direct way to treat genetic conditions as well as other conditions. There are also other related approaches like gene editing. There are many different versions and approaches to gene therapy and gene editing. It all rests on understanding how genes work and how changes in genes can affect our health. Researchers all over the world are studying many different facets of gene therapy and gene editing.
The Center for Biologics Evaluation and Research (CBER) regulates cellular therapy products, human gene therapy products, and certain devices related to cell and gene therapy. CBER uses both the Public Health Service Act and the Federal Food Drug and Cosmetic Act as enabling statutes for oversight.
Cellular therapy products include cellular immunotherapies, cancer vaccines, and other types of both autologous and allogeneic cells for certain therapeutic indications, including hematopoietic stem cells and adult and embryonic stem cells. Human gene therapy seeks to modify or manipulate the expression of a gene or to alter the biological properties of living cells for therapeutic use. CBER has approved both cellular and gene therapy products.
Cellular and gene therapy-related research and development in the United States continue to grow at a fast rate, with a number of products advancing in clinical development. In addition to regulatory oversight of clinical studies, CBER provides proactive scientific and regulatory advice to medical researchers and manufacturers in the area of novel product development.
Holistic Viral Vector Production Processes
What is a Viral Vector?
Viruses are infectious agents that can only replicate inside of living cells. This trait is used by molecular biologists for delivery of genetic materials into cells. Viral vectors are also explored for use in gene and cell therapy and as basis for prophylactic and therapeutic vaccines. In gene therapy, viral vectors can be used for delivery of functional genes to replace defective genes to cure genetic disorders. As a vaccine platform, viral vectors can be used for expression and presentation of pathogenic antigens to induce an immune response by mimicking a natural infection. Viral vectors can also be used in oncolytic therapies to specifi cally target and kill tumor cells.
Viral vector systems
Although tailored to their specific applications, viral vectors share some key attributes. Vectors should be modified to provide safe handling (no production of new virions in host) and low toxicity (no effect of the physiology of the normal host cell). They should also be stable (no rearrangement of genome), and for manufacturing, it is important that the viral vector is easily quantifi ed and that it lends itself to large-scale production. Example of viral vector systems are retrovirus, lentivirus, poxvirus, adenovirus, and adeno-associated virus.
Retrovirus
Recombinant retroviruses have the ability to stably integrate into the host genome. These viruses express a reverse transcriptase to copy its RNA genome into DNA and an integrase to integrate the DNA copy into the genome of the host cell. Typically, replication-defective retroviruses are used in medicine, as these viruses can infect and deliver its viral genome, but fail to lyse and kill the host cell. Retroviruses, however, can only integrate into the genome of actively dividing cells. Hence, many cells (e.g., neurons) are resistant to retrovirus infection and integration.
Lentivirus
Lentiviruses are a subclass of retroviruses, but in contrast to other retroviruses, lentiviruses can integrate into the genome of non-dividing cells. As retrovirus vectors, lentivirus vectors never include genes for replication. Lentivirus production therefore require propagation in, so called, packaging cell lines such as HEK293 cells transfected with plasmids that encode the virion proteins. Lentiviruses are commonly used for cell therapy, Figure 7.
Poxvirus
The poxvirus family comprises numerous species, of which one is vaccinia virus (VACV). As it induces a strong immune response in humans, VACV is tested in recombinant vaccines as a vector for expression of foreign proteins. In wild type form, VACV has also been successfully used to eradicate smallpox. VACV is a double-stranded DNA virus that enters its host cell by cell fusion. Its large genome (185 kilobases) tolerates insertions of foreign DNA fragments of more than 25 kilobases, creating an opportunity for use of VACV in vaccines with large or even several antigens. Poxviruses have also been modifi ed and tested as oncolytic therapies.
Adenovirus
Adenoviruses are double-stranded DNA viruses that replicate in the cell nucleus of vertebrates. In opposite to retroviruses and lentiviruses, adenoviruses do not integrate into the genome of the host cell. Adenoviruses allows foreign DNA to easily be introduced into their DNA, and they can be propagated in several cell types. In addition, adenoviruses have been shown to induce a broad immune response, including cytotoxic T-cells. Hence, adenovirus is one of the most explored viral vectors for use in vaccines against infectious diseases and in oncolytic therapies. It has also been used in the development of therapeutic vaccines, and in gene therapies.
Adeno-Associated Virus (AAV)
AAV is a single-stranded DNA virus that can infect both actively dividing and non-dividing cells of humans and some other primates. It can integrate into the genome of the host cell but mostly, as adenovirus, AAV replicate without incorporating its genome into the host cell chromosome. As opposed to adenovirus, which is a larger virus that can deliver DNA inserts of up to 36 kilobases, AAV is a small virus that can only deliver smaller inserts of up to 5 kilobases. AAV is mainly used for gene therapy.
Manufacturing of viral vectors
The promising results from clinical studies of the use of viral vectors to address important medical needs, have surged the interest in developing scalable and cost-efficient manufacturing processes. For gene therapy alone, the global market value is estimated to exceed 10 billion USD by 2025. For regulatory compliance, products intended for therapeutic use should be well characterized and manufactured to high purity, efficacy, and safety, and high levels of GMP compliance should be met. The continuous development of recombinant viral vectors expands the commercial product pipeline, prompting the use of virus vector manufacturing platforms.
In 2020, the FDA received more than 900 new investigational gene or cell therapy drug applications.30 By the year 2025, the agency anticipates that 10 to 20 gene therapies will be approved per year.31 Gene therapy sponsors need to consistently meet the challenge of conducting safe, ethical, patient-focused studies in a dynamic regulatory and clinical trial environment. To successfully navigate the journey to marketing authorization, sponsors must understand and plan for all of the nuances associated with designing and executing these complex studies.
Below is a list of licensed products from the Office of Tissues and Advanced Therapies (OTAT).
List of Approved Products
Approved Cell and Gene Therapy Products
- ABECMA (idecabtagene vicleucel)
Celgene Corporation, a Bristol-Myers Squibb Company
Ferring Pharmaceuticals A/S
- ALLOCORD (HPC, Cord Blood)
SSM Cardinal Glennon Children’s Medical Center
Juno Therapeutics, Inc., a Bristol-Myers Squibb Company
- CARVYKTI (ciltacabtagene autoleucel)
Janssen Biotech, Inc.
- CLEVECORD (HPC Cord Blood)
Cleveland Cord Blood Center
Duke University School of Medicine
- GINTUIT (Allogeneic Cultured Keratinocytes and Fibroblasts in Bovine Collagen)
Organogenesis Incorporated
- HEMACORD (HPC, cord blood)
New York Blood Center
CSL Behring LLC
Clinimmune Labs, University of Colorado Cord Blood Bank
- HPC, Cord Blood – MD Anderson Cord Blood Bank
MD Anderson Cord Blood Bank
- HPC, Cord Blood – LifeSouth
LifeSouth Community Blood Centers, Inc.
- HPC, Cord Blood - Bloodworks
Bloodworks
- IMLYGIC (talimogene laherparepvec)
BioVex, Inc., a subsidiary of Amgen Inc.
- KYMRIAH (tisagenlecleucel)
Novartis Pharmaceuticals Corporation
Fibrocell Technologies
Spark Therapeutics, Inc.
- MACI (Autologous Cultured Chondrocytes on a Porcine Collagen Membrane)
Vericel Corp.
Dendreon Corp.
Enzyvant Therapeutics GmbH
- SKYSONA (elivaldogene autotemcel)
bluebird bio, Inc.
Stratatech Corporation
- TECARTUS (brexucabtagene autoleucel)
Kite Pharma, Inc.
- YESCARTA (axicabtagene ciloleucel)
Kite Pharma, Incorporated
- ZYNTEGLO (betibeglogene autotemcel)
bluebird bio, Inc.
- ZOLGENSMA (onasemnogene abeparvovec-xioi)
Novartis Gene Therapies, Inc.
References
- Singh VK, Saini A, Kalsan M, Kumar N, Chandra R. Describing the stem cell potency: the various methods of functional assessment and in silico diagnostics. Front Cell Dev Biol. (2016) 4:134. 10.3389/fcell.2016.00134 [PMC free article] [PubMed]
- Hanna JH, Saha K, Jaenisch R. Pluripotency and cellular reprogramming: facts, hypotheses, unresolved issues. Cell. (2010) 143:508–25. 10.1016/j.cell.2010.10.008 [PMC free article] [PubMed]
- Chu DT, Nguyen TT, Tien NLB, Tran DK, Jeong JH, Anh PG, et al. Recent Progress of stem cell therapy in cancer treatment: molecular mechanisms and potential applications. Cells. (2020) 9:563. 10.3390/cells9030563 [PMC free article] [PubMed]
- Chagastelles PC, Nardi NB. Biology of stem cells: an overview. Kidney Int Suppl. (2011) 1:63–7. 10.1038/kisup.2011.15 [PMC free article] [PubMed]
- NIH Stem Cell Information Home Page. The Adult Stem Cell. Bethesda, MD: (2016). https:// stemcells.nih.gov/info/2001report/chapter4.htm (accessed May 3, 2021).
- Gurusamy N, Alsayari A, Rajasingh S, Rajasingh J. Adult stem cells for regenerative therapy. Prog Mol Biol Transl Sci. (2018) 160:1–22. 10.1016/bs.pmbts.2018.07.009 [PubMed]
- Mosaad YM. Hematopoietic stem cells: an overview. Transfus Apher Sci. (2014) 51:68–82. 10.1016/j.transci.2014.10.016 [PubMed]
- Zouboulis CC, Adjaye J, Akamatsu H, Moe-Behrens G, Niemann C. Human skin stem cells and the ageing process. Exp Gerontol. (2008) 43:986–97. 10.1016/j.exger.2008.09.001 [PubMed]
- Grochowski C, Radzikowska E, Maciejewski R. Neural stem cell therapy—brief review. Clin Neurol Neurosurg. (2018) 173:8–14. 10.1016/j.clineuro.2018.07.013 [PubMed]
- Shammaa R, El-Kadiry AEH, Abusarah J, Rafei M. Mesenchymal stem cells beyond regenerative medicine. Front Cell Dev Biol. (2020) 8:72. 10.3389/fcell.2020.00072 [PMC free article] [PubMed]
- Wei X, Yang X, Han Z, Qu F, Shao L, Shi Y. Mesenchymal stem cells: a new trend for cell therapy. Acta Pharmacol Sin. (2013) 34:747–54. 10.1038/aps.2013.50 [PMC free article] [PubMed]
- Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause DS, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. the international society for cellular therapy position statement. Cytotherapy. (2006) 8:315–7. 10.1080/14653240600855905 [PubMed]
- Soltanian S, Matin MM. Cancer stem cells and cancer therapy. Tumor Biol. (2011) 32:425– 40. 10.1007/s13277-011-0155-8 [PubMed]
- Codd AS, Kanaseki T, Torigo T, Tabi Z. Cancer stem cells as targets for immunotherapy. Immunology. (2018) 153:304–14. 10.1111/imm.12866 [PMC free article] [PubMed]
- Atashzar MR, Baharlou R, Karami J, Abdollahi H, Rezaei R, Pourramezan F, et al.. Cancer stem cells: a review from origin to therapeutic implications. J Cell Physiol. (2020) 235:790– 803. 10.1002/jcp.29044 [PubMed]
- Lathia J, Liu H, Matei D. The clinical impact of cancer stem cells. Oncologist. (2020) 25:123– 31. 10.1634/theoncologist.2019-0517 [PMC free article] [PubMed]
- Clarke MF. Clinical and therapeutic implications of cancer stem cells. N Engl J Med. (2019) 380:2237–45. 10.1056/NEJMra1804280 [PubMed]
- US FDA. Regulatory Considerations for Human Cells, Tissues, and Cellular and Tissue-Based Products: Minimal Manipulation Homologous Use - Guidance for Industry and Food and Drug Administration Staff. (2020). https://www.fda.gov/media/109176/download
- US FDA. Same Surgical Procedure Exception under 21 CFR 1271.15(b): Questions Answers Regarding the Scope of the Exception; Guidance for Industry. (2017). https://www.fda. gov/media/89920/download
- Bloomberg Law. INSIGHT: FDA’s Aggressive Enforcement Against Stem Cell Companies Starting to Ripen. US Law Week. (2019). https://news.bloomberglaw.com/us-law-week/ insight-fdas-aggressive-enforcement-against-stem-cell-companies-starting-to-ripen
- US FDA. Statement on stem cell clinic permanent injunction FDA’s ongoing efforts to protect patients from risks of unapproved products. FDA Statement. (2019). https://www. fda.gov/news-events/press-announcements/statement-stem-cell-clinic-permanent[1]injunction-and-fdas-ongoing-efforts-protect-patients-risks
- Los Angeles Times. Column: Judge Hands FDA a Loss on Stem Cell Clinics. (2020). https:// www.latimes.com/business/story/2020-01-28/judge-fda-stem-cell-clinics
- United States District Court. United States of America v. California Stem Cell Treatment Center, Inc., et al. California: (2020). https://s3.documentcloud.org/documents/6682558/ Stem-Cell-Berman-Ruling.pdf
- Title 21 - Food and Drugs Chapter I - Food and Drug Administration, Department of Health and Human Services Subchapter L - Regulations Under Certain Other Acts Administered by the Food and Drug Administration Part 1271 - Human Cells, Tissues, and Cellular and Tissue-Based Products. eCFR: 21 CFR 1271.3 -- How does FDA define important terms in this part?
- 1271.15 Are there any exceptions from the requirements of this part? eCFR: 21 CFR 1271.15 -- Are there any exceptions from the requirements of this part?
- Regulatory Considerations for Human Cells, Tissues, and Cellular and Tissue-Based Products: Minimal Manipulation and Homologous Use, Guidance for Industry and Food and Drug Administration Staff. Does your HCT/P meet the criteria in 21 CFR 1271.10(a)? Regulatory Considerations for Human Cells, Tissues, and Cellular and Tissue-Based Products: Minimal Manipulation and Homologous Use; Guidance for Industry and Food and Drug Administration Staff, (fda.gov)
- Cellular & Gene Therapy Products, Cellular & Gene Therapy Products | FDA
- Long Term Follow-Up After Administration of Human Gene Therapy Products, Guidance for Industry; Long Term Follow-Up After Administration of Human Gene Therapy Products; Guidance for Industry, January 2020
- National Institutes of Health (NIH) U.S. National library of medicine. What is a gene? https://ghr.nlm.nih.gov/primer/basics/gene.
- Cell Culture DISH. A Remarkable Year for Gene Therapies. https://cellculturedish.com/ remarkable-year-for-gene-therapies/.
- U.S. Food and Drug Administration. Statement from FDA Commissioner Scott Gottlieb, M.D. and Peter Marks, M.D., Ph.D., Director of the Center for Biologics Evaluation and Research on new policies to advance development of safe and effective cell and gene therapies. https://www.fda.gov/news-events/press-announcements/statement-fda-commissioner-scott-gottlieb-md-and-peter-marks-md-phd-director-center-biologics
Subscribe to our e-Newsletters
Stay up to date with the latest news, articles, and events. Plus, get special
offers from American Pharmaceutical Review delivered to your inbox!
Sign up now!